

Abstract
The aim of this study was to investigate the prevalence and correlates of depressive symptoms in the largest number of Korean individuals examined to date. We analyzed cross-sectional data collected from 229,595 Korean adults aged 19 yr and above who participated in a Korean Community Health Survey conducted in 2009. The Center for Epidemiologic Studies Depression Scale (CES-D) was used as the measurement tool for depressive symptoms (CES-D score over 16) and definite depression (CES-D score over 25). Multivariate logistic regression analysis was performed to identify associations between sociodemographic factors and depressive symptoms. The percentages of depressive symptoms and definite depression in the total study population were 11% (7.8% for men, 14.0% for women) and 3.7%, (2.4% for men, 5.0% for women), respectively. Female gender, older age, disrupted marital status, low education and income level, multigenerational household composition and metropolitan residence were associated with greater risk of depressive symptoms. The present study provides a valid prevalence and correlates of depressive symptoms, using the largest representative sample of the Korean general population to date. Various sociodemographic factors contribute to the prevalence and effects of depressive symptoms in Korea.
Keywords: Depression, Epidemiology, Prevalence, Socioeconomic Factors
INTRODUCTION
Depression is one of the most common mental illnesses and a major public health concern throughout the world. According to the Global Burden of Disease study, depression ranks fourth in the world among causes of early death and disability, and is projected to become the second leading cause by 2020 (1, 2). In Korea, depression has also become a prominent social issue because of a rapid increase in suicides. The most recent report showed that the lifetime prevalence of major depressive disorder is 6.7% (4.8% in men and 9.1% in women), and has increased by 0.2% annually for the last decade (3).
To our knowledge, four representative published studies have reported the prevalence of depression in Korea using nationwide community samples (4-7). These epidemiological studies estimated the prevalence of depression and provided vital information for public mental health policy formulation in Korea. However, they had several methodological limitations. Some excluded people over 60 or 65 yr or collected their study samples from just 10 or 12 catchment areas (4-6). Another used a telephone survey method (7). All the studies also had sample sizes of only a few thousand people; these numbers could not reliably represent the general population of Korea.
In order to overcome these limitations, we analyzed data sets collected by the Korean Community Health Survey (KCHS) on individuals aged ≥ 19 yr in 16 metropolitan cities and provinces with 253 regional sites around the country in 2009 (8). The standardized questionnaire of the KCHS consisted of 358 questions in 13 fields and covered a wide variety of health topics including depression, which was assessed by the Korean version of the Center for Epidemiologic Studies Depression Scale (CES-D) (9).
Using data from the 2009 KCHS, we examined the prevalence of depressive symptoms and their association with sociodemographic factors, in the largest sample studied to date. The 2009 KCHS data allowed us to obtain a valid estimate of the prevalence of depressive symptoms and their correlates in Korea.
MATERIALS AND METHODS
Data and subjects
This study used data obtained from the Korean Community Health Survey (KCHS) conducted in 253 local districts in Korea in 2009. The KCHS is a nationwide health interview survey carried out by the Korean Centers for Disease Control and Prevention (KCDC) to estimate the pattern of disease prevalence and morbidity, as well as to understand the personal lifestyle and health behavior, of adults aged 19 yr and over. The KCHS was conducted on 800-900 subjects selected by the probability proportional to sampling method and the systematic sampling method among the adults aged 19 yr or older living in each area from September to November, 2009. The KCHS has a two-stage sampling process. The first sampling stage is the process of selecting a sample area (tong/ban/ri) that is a primary sample unit, using a probability proportional to the sampling method. In the second sampling stage, the number of households in the selected sample tong/ban/ri is identified to create a household directory, and sample households are selected through systematic sampling methods (10). For the sample to be statistically representative of the population, the data collected in the KCHS sample is weighted based on the sample design. The KCHS was administered by trained interviewers as face-to-face interviews. The KCHS collects detailed information on demographic and socioeconomic characteristics, health-related problems and past medical histories. There were 230,715 individuals included in the 2009 KCHS (8). We excluded 1,120 individuals due to the insufficient information on sociodemographic variables (age, marital status, residence location, generational household composition and educational status) or depressive symptoms. Finally, a total of 229,595 individuals (106,543 men and 123,052 women) were included in the analysis.
Variables
Ages were grouped into 19-29 yr, 30-39 yr, 40-49 yr, 50-59 yr, 60-69 yr, and 70 yr or over. Marital status was classified as spouse, separated, divorced, widowed and never married. Residence locations were classified into four groups according to the Korean administrative districts based on population: 1) county (less than 50,000), 2) small city (more than 50,000), 3) medium city (more than 500,000), 4) metropolitan (more than 1,000,000). Generational household composition was categorized into one generation family, two generation family and three generation family. Average monthly family income of the subjects was classified as one million Korean won (KRW) or less, two million KRW or less, three million KRW or less, four million KRW or less and 4.01 million KRW or more. Educational status was classified as non-educated, elementary school, middle school, high school and college or more.
The Center for Epidemiological Depression Scale (CES-D)
The 20-item version of the CES-D (11), which has been previously validated in the Korean population (9), was used to measure depression. It is designed to identify the existence of depressive symptoms and to evaluate their severity. To estimate the prevalence of depressive symptoms (probable depression), we used a CES-D score of 16. To estimate the prevalence of definite depression, we defined a CES-D score of 25 as the cut-off (6, 12).
Statistical analysis
The CES-D scores were expressed as mean ± standard deviation (SD), and those of distributions were shown as percentages. A weighted prevalence was calculated for each respondent to approximate the national population with respect to age and gender, as defined in the 2005 census performed by the Korean National Statistical Office. Age-adjusted prevalence was calculated by the direct method and the age-distribution for the 2005 census population. Differences in CES-D scores were assessed using either Student's t-test or analysis of variance (ANOVA). Differences in distributions were assessed using the chi-squared test. P values for trend were calculated by the Cochran-Mantel-Haenszel test. The significance of various sociodemographic characteristics as risk factors for depressive symptoms was calculated by multivariate logistic regression analysis. Odds ratios (OR), 95% confidence intervals (CI) and P values were recorded as the outcomes. P values less than 0.05 were considered statistically significant. All analyses were performed using SAS 9.2 (SAS Inc., Cary, NC, USA).
Ethics statement
The protocol of the KCHS was reviewed and approved by the institutional review board of the KCDC (2010-02-CON-22-P). Written informed consent was obtained from all participants in the KCHS.
RESULTS
Sociodemographic characteristics of the study population
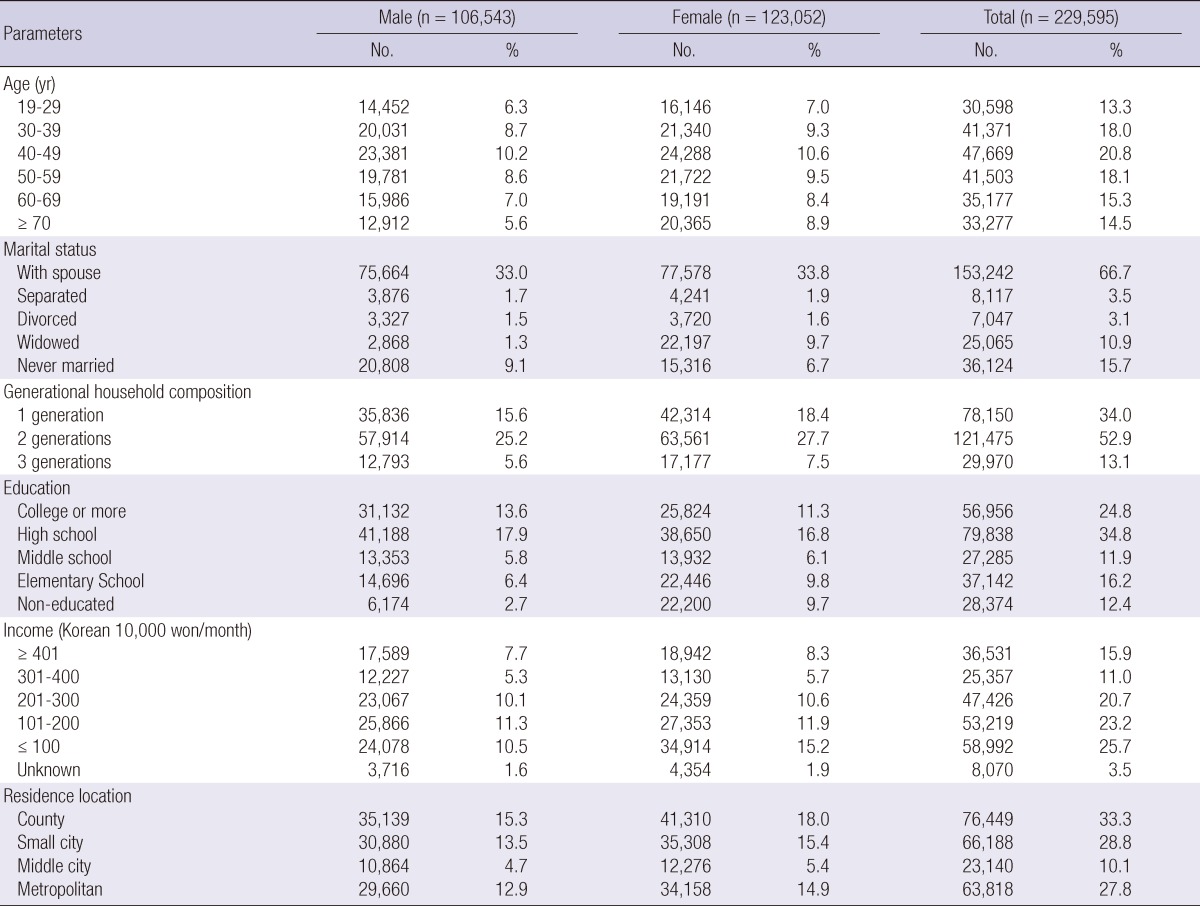
The sociodemographic characteristics of the study population are summarized in Table 1. The mean ages of the total study population, for males, and for females were 49.5 ± 16.7 (mean ± SD) yr, 48.6 ± 16.1 yr, and 50.4 ± 17.2 yr, respectively. The distributions of several sociodemographic characteristics tested in this study differed by gender. In particular, women had lower education levels. The frequency of widowed women was more than seven times that of widowed men.
Table 1.
Sociodemographic characteristics of the study population (Korean Community Health Survey, 2009)
Prevalence of depressive symptoms and definite depression
The mean CES-D scores for the total population, for males, and for females were 6.3 ± 7.9, 5.1 ± 7.0, and 7.3 ± 8.6, respectively: the mean CES-D score for females was significantly higher than for males (P < 0.001) (Table 2). The prevalence of depressive symptoms, as defined by a cutoff score of 16, for the total population was 11.0% (men, 7.8%; women, 14.0%); that of definite depression, as defined by a cutoff score of 25, for the total population was 3.7% (men, 2.4%; women, 5.0%). Women had a significantly higher prevalence of both depressive symptoms and definite depression than men (P < 0.001) (Table 2). In addition, as age increased, the prevalence of both depressive symptoms tended to increase for both men and women (Fig. 1). Interestingly, the prevalence of depressive symptoms in age group 19-29 yr was significantly higher than in age group 30-39 yr (P < 0.001).
Table 2.
Prevalences of depressive symptoms and definite depression according to age and sex
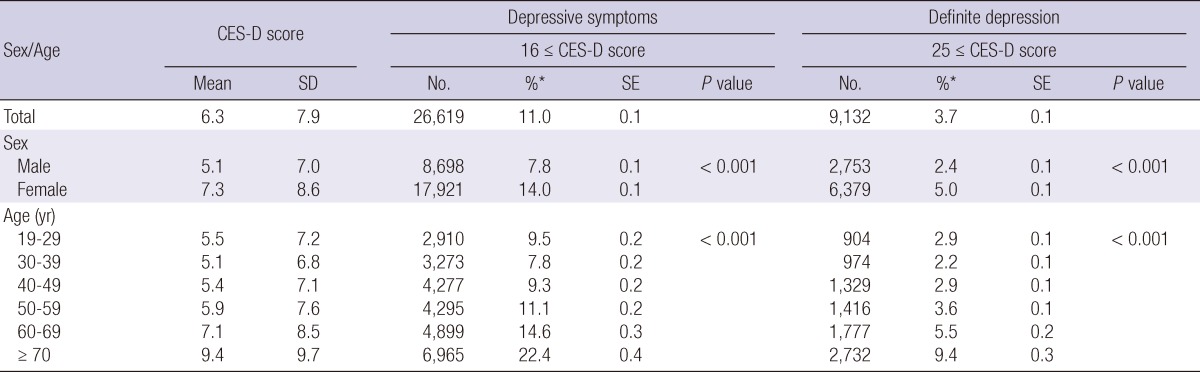
*The prevalence of depressive symptoms (or definite depression) was estimated from the percentage of subjects reporting depressive symptoms (or definite depression) after weighting for sex and age to approximate the national population in terms of sex and age as defined by the 2005 census performed by the Korean National Statistical Office.
CES-D, the Center for Epidemiologic Studies Depression Scale; SD, standard deviation; SE, standard error.
Fig. 1.

Prevalence of depressive symptoms according to age group.
The association between depressive symptoms and sociodemographic characteristics
The prevalence of depressive symptoms increased with disrupted marital status in both genders (P for trend < 0.001). As the generational household composition increased, the prevalence showed a tendency to decrease in both genders (P for trend < 0.001). However, the prevalence showed a tendency to increase with declining educational status and household income in both genders (P for trend < 0.001). It also showed a tendency to increase in both genders as residence location became more urbanized (P for trend < 0.001) (Table 3).
Table 3.
Prevalence of depressive symptoms according to sociodemographic characteristics by sex
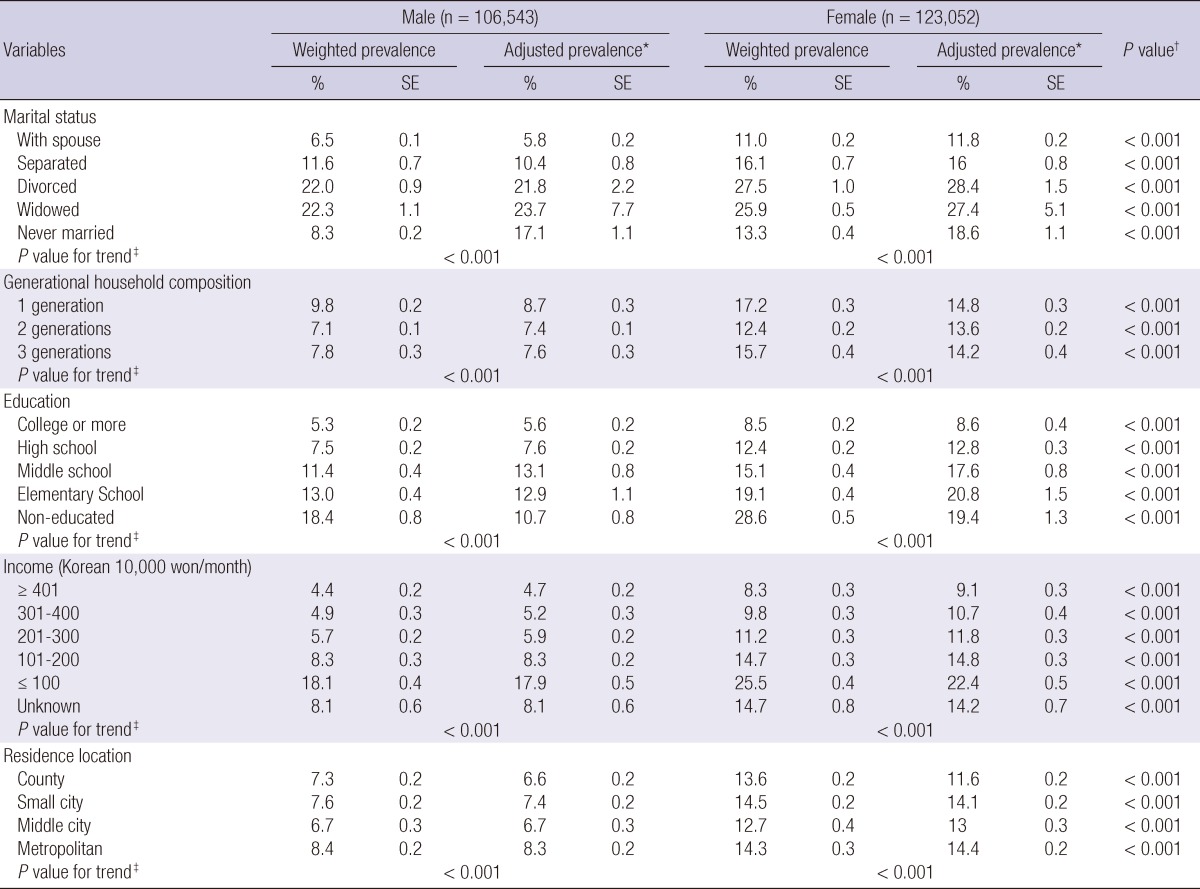
*adjusted for age by direct standardization using 2005 Census as standard population (categorical variable: units of 10 yr); †P values for the weighted prevalence of depressive symptoms using chi-square test; ‡P values for trend were calculated by the Cochran-Mantel-Haenszel test after adjustment for age (categorical variable: units of 10 yr). SE, standard error.
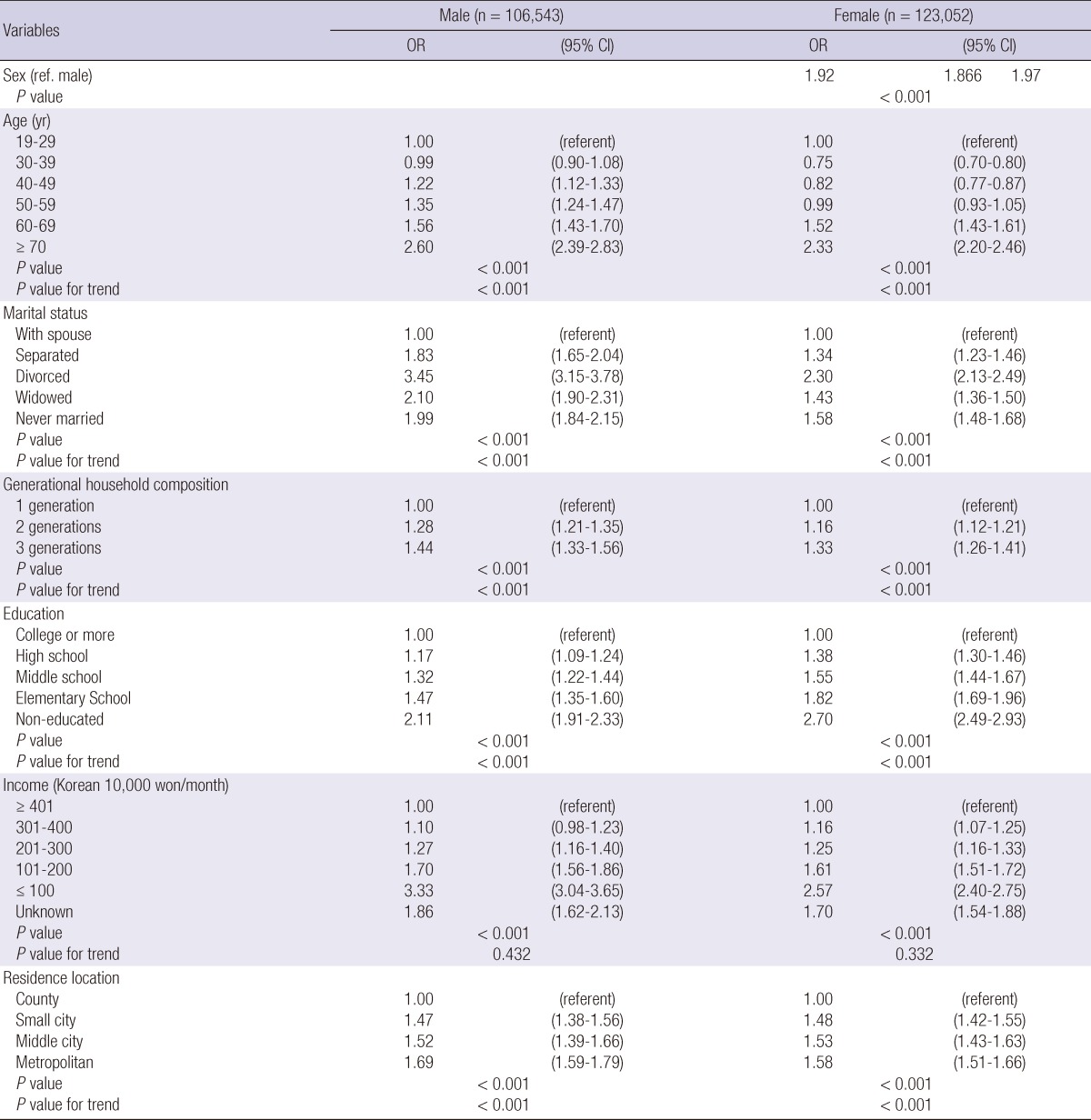
Table 4 gives the results of a multivariate logistic regression analysis in which the regression of presence or absence of depressive symptoms on sociodemographic characteristics was analyzed. Females were significantly more likely to have depressive symptoms than males (OR, 1.92; 95% CI, 1.89-1.97). In both genders, those who were older, of disrupted marital status, in three-generational households, had lower income, lower education level, and resided in higher levels of urbanization were likely to have significantly higher frequencies of depressive symptoms than their counterparts in other categories. In particular, the highest odds ratio in male was found for those who were divorced (OR, 3.45; 95% CI, 3.15-3.78). On the other hand, in female, it was found for those who had no education (OR, 2.70; 95% CI, 2.49-2.93).
Table 4.
Odds ratios (OR) and 95% confidence intervals (CI) from multivariate logistic regression analysis for the relation between depressive symptoms and the covariates in Korean adults, 19 yr or older (Korean Community Health Survey, 2009)
DISCUSSION
In this study, we found that the prevalences of depressive symptoms and definite depression were 11.0% and 3.7%, respectively. Comparing our results with those of previous nationwide epidemiologic studies, the prevalence of depressive symptoms found by us was much lower than that reported by Cho et al. (6) using the CES-D in 1998 (CES-D score of ≥ 16, 23.1% in males and 27.4% in females). However, the prevalence of definite depression obtained here is similar to those of recent epidemiological surveys of mental disorders in Korea using the Composite International Diagnostic Interview (CIDI). The results of these previous studies are summarized in Table 5.
Table 5.
Representative nationwide studies on the prevalence of depression in Korea

CES-D, the Center for Epidemiologic Studies Depression Scale; K-CIDI, the Korean version of Composite International Diagnostic Interview.
In general, previous studies using self-report depression scales such as CES-D or the Beck Depression Inventory (BDI) have yielded higher symptom scores and greater prevalence of depression in Korean samples than in Western countries (12). Culturally variable response styles among ethnic groups may be responsible for the difference (14, 15). Since we recorded a lower prevalence of depressive symptoms than previous studies using the same self-report scale (6, 16, 17) and a similar prevalence of definite depression to those of previous studies using fully structured interviews (4, 5), our findings raise the possibility that there has been a change of style of response to questionnaires for depression among Koreans over the last two decades. Increased awareness of depression and westernizing influences may have contributed to such a change.
The present study showed that females were 1.9 times more likely to have depressive symptoms than males. This is consistent with the fact that depressive disorders are twice as common in women as in men. Adverse experiences in childhood, depression and anxiety disorders in childhood and adolescence, socio-cultural roles and related adverse experiences, and psychological attributes affecting vulnerability to life events and coping skills are likely to be involved in the preponderance of depressive disorders in female (13). In addition, the hypothalamic-pituitary-adrenal (HPA) axis is more strongly activated in depressed women than in depressed men, and menopause, with the accompanying loss of estrogens, also causes the greatest disturbance of the HPA axis. It is possible that the constantly changing steroid milieu in women contributes to their vulnerability to depression (18).
We found that the prevalences of depressive symptoms and definite depression increased with age in both men and women. There is a great deal of evidences for increasing rate of depression as adults grow older. However, several previous studies have suggested that increasing age is not a risk factor for depression independent of the effects of other risk factors (19-23). Other risk factors associated with aging, such as poor physical health, not being married and low education level were found to be associated with depressive symptoms (23-25).
Interestingly, the results of this study show that the prevalences of depressive symptoms and definite depression were higher in people in their 20s than in those in their 30s. This finding is in accord with a recent review of epidemiologic studies on depression in Korea (12). Recently, youth unemployment has become a serious social problem across the world. The youth unemployment rate in Korea is also at a record high these days. Unemployment among the over 30s averages between 2 and 4%, whereas it is about at 7% or 8% among the under 30s (26). In addition, the problem of high tuition fees which has been raised by university students has become a sensitive political issue. According to OECD statistics, Korea has the second-highest tuition fees in the OECD, behind only the USA (27). These socio-environmental conditions may result in an increased psychological burden on young adults.
With regard to marital status, living with a spouse seems to be protective against depression in both genders. In particular, divorced men were about 3.5 times more likely to have depressive symptoms than males living with a spouse. The association of divorce with depressive symptoms was more pronounced in men (OR, 3.45; 95% CI, 3.15-3.75) than women (OR, 2.30; 95% CI, 2.13-2.49) on the basis of each reference condition. Disrupted marital status was more strongly associated with depressive symptom among men than among women. These findings agree with the longitudinal data from Statistics Canada's National Population Health Survey (NPHS) (28).
With regard to generational household composition, residing in multi-generational household is a risk factor for depressive symptoms. There is much evidence that depression is inversely related to the level of support, attachment, and approval adolescents experience in the family environment (29). However, the stress of living in multi-generational household may cause depressive symptom because of conflicts between family members.
In the present study, non-educated women were 2.7 times more likely to have depressive symptoms than women with college degrees. The association between lack of education and depressive symptoms was more pronounced in women (OR, 2.70; 95% CI, 2.49-2.93) than men (OR, 2.11; 95% CI, 1.91-2.33) on the basis of each reference condition. Individuals of higher socioeconomic position generally report lower levels of depression, regardless of their gender. Does education improve psychological well-being more for one sex than for the other? Data from a 1995 survey of US adults with follow-ups in 1998 and 2001 support the view that education improves well-being more for women, because socioeconomic disadvantage makes them depend more on education to achieve well-being. Depression decreases more steeply for women as their level of education increases than it does for men. The gender gap in depression essentially disappears among persons with a college degree or higher (30).
A greater prevalence of almost all major psychiatric disorders is associated with higher levels of urbanization (31). Our data showed that residents in metropolitan region were significantly more likely to have depressive symptoms than those living in the country side. This is in line with previous studies showing that psychiatric disorders are more prevalent and more complex among the inhabitants of more urbanized areas, probably due to various environmental stressors (32-35).
In conclusion, the present study provides a valid estimate of the prevalence of depressive symptoms in Korea, using the largest representative sample of Koreans to date. A relationship was found between depressive symptoms and various sociodemographic characteristics such as gender, marital status, generational household composition, education, income and type of dwelling place. The findings provide valuable help in formulation policies to sustain mental health in Korea. Further studies using various methods will be required to investigate the effects of sociodemographic factors and health-related behaviors on depression, and explore the causal relationships between them.
ACKNOWLEDGMENTS
The authors appreciated all participating citizens in 2009 KCHS and all members of the 2009 KCHS team. The authors have no conflicts of interest to disclose.
Footnotes
This work was supported by the research fund of Hanyang University Institute of Aging Society in 2009 (200900000000243).
References
- 1.Lopez AD, Murray CC. The global burden of disease, 1990-2020. Nat Med. 1998;4:1241–1243. doi: 10.1038/3218. [DOI] [PubMed] [Google Scholar]
- 2.Ustun TB, Ayuso-Mateos JL, Chatterji S, Mathers C, Murray CJ. Global burden of depressive disorders in the year 2000. Br J Psychiatry. 2004;184:386–392. doi: 10.1192/bjp.184.5.386. [DOI] [PubMed] [Google Scholar]
- 3.Jeon HJ. Epidemiologic studies on depression and suicide. J Korean Med Assoc. 2012;55:322–328. [Google Scholar]
- 4.Cho MJ, Chang SM, Hahm BJ, Chung IW, Bae A, Lee YM, Ahn JH, Won SH, Son J, Hong JP, et al. Prevalence and correlates of major mental disorders among Korean adults: a 2006 National Epidemiologic Survey. J Korean Neuropsychiatr Assoc. 2009;48:143–152. [Google Scholar]
- 5.Cho MJ, Kim JK, Jeon HJ, Suh T, Chung IW, Hong JP, Bae JN, Lee DW, Park JI, Cho SJ, et al. Lifetime and 12-month prevalence of DSM-IV psychiatric disorders among Korean adults. J Nerv Ment Dis. 2007;195:203–210. doi: 10.1097/01.nmd.0000243826.40732.45. [DOI] [PubMed] [Google Scholar]
- 6.Cho MJ, Nam JJ, Suh GH. Prevalence of symptoms of depression in a nationwide sample of Korean adults. Psychiatry Res. 1998;81:341–352. doi: 10.1016/s0165-1781(98)00122-x. [DOI] [PubMed] [Google Scholar]
- 7.Ohayon MM, Hong SC. Prevalence of major depressive disorder in the general population of South Korea. J Psychiatr Res. 2006;40:30–36. doi: 10.1016/j.jpsychires.2005.02.003. [DOI] [PubMed] [Google Scholar]
- 8.Kim YT, Choi BY, Lee KO, Kim H, Chun JH, Kim SY, Lee DH, Ghim YA, Lim DS, Kang YW, et al. Overview of Korean Community Health Survey. J Korean Med Assoc. 2012;55:74–83. [Google Scholar]
- 9.Cho MJ, Kim KH. Diagnostic validity of the CES-D (Korean version) in the assessment of DSM-III-R major depression. J Korean Neuropsychiatr Assoc. 1993;32:381–399. [Google Scholar]
- 10.Rim H, Kim H, Lee K, Chang S, Hovell MF, Kim YT, Kim Y, Kang G, Tak Y, Im J. Validity of self-reported healthcare utilization data in the Community Health Survey in Korea. J Korean Med Sci. 2011;26:1409–1414. doi: 10.3346/jkms.2011.26.11.1409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Radloff LS. The CES-D scale: a self report depression scale for research in the general population. Appl Psych Meas. 1977;1:385–401. [Google Scholar]
- 12.Park JH, Kim KW. A review of the epidemiology of depression in Korea. J Korean Med Assoc. 2011;54:362–369. [Google Scholar]
- 13.Piccinelli M, Wilkinson G. Gender differences in depression. Critical review. Br J Psychiatry. 2000;177:486–492. doi: 10.1192/bjp.177.6.486. [DOI] [PubMed] [Google Scholar]
- 14.Jang Y, Kim G, Chiriboga D. Acculturation and manifestation of depressive symptoms among Korean-American older adults. Aging Ment Health. 2005;9:500–507. doi: 10.1080/13607860500193021. [DOI] [PubMed] [Google Scholar]
- 15.Lee JJ, Kim KW, Kim TH, Park JH, Lee SB, Park JW, McQuoid DR, Steffens DC. Cross-cultural considerations in administering the center for epidemiologic studies depression scale. Gerontology. 2011;57:455–461. doi: 10.1159/000318030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kim E, Jo SA, Hwang JY, Shin C, Kim DK, Woo EK, Kim SS, Shin KR, Jo I. A survey of depressive symptoms among South Korean adults after the Korean financial crisis of late 1997: prevalence and correlates. Ann Epidemiol. 2005;15:145–152. doi: 10.1016/j.annepidem.2004.05.004. [DOI] [PubMed] [Google Scholar]
- 17.Kim MD, Hong SC, Lee CI, Kwak YS, Shin TK, Jang YH, Oh EH, Lee JW, Jeon BH, Hwang SE. Prevalence of depression and correlates of depressive symptoms for residents in the urban part of Jeju Island, Korea. Int J Soc Psychiatry. 2007;53:123–134. doi: 10.1177/0020764006075022. [DOI] [PubMed] [Google Scholar]
- 18.Young E, Korszun A. Sex, trauma, stress hormones and depression. Mol Psychiatry. 2010;15:23–28. doi: 10.1038/mp.2009.94. [DOI] [PubMed] [Google Scholar]
- 19.O'Hara MW, Kohout FJ, Wallace RB. Depression among the rural elderly. A study of prevalence and correlates. J Nerv Ment Dis. 1985;173:582–589. doi: 10.1097/00005053-198510000-00002. [DOI] [PubMed] [Google Scholar]
- 20.Berkman LF, Berkman CS, Kasl S, Freeman DH, Jr, Leo L, Ostfeld AM, Cornoni-Huntley J, Brody JA. Depressive symptoms in relation to physical health and functioning in the elderly. Am J Epidemiol. 1986;124:372–388. doi: 10.1093/oxfordjournals.aje.a114408. [DOI] [PubMed] [Google Scholar]
- 21.Kennedy GJ, Kelman HR, Thomas C. The emergence of depressive symptoms in late life: the importance of declining health and increasing disability. J Community Health. 1990;15:93–104. doi: 10.1007/BF01321314. [DOI] [PubMed] [Google Scholar]
- 22.Blazer D, Burchett B, Service C, George LK. The association of age and depression among the elderly: an epidemiologic exploration. J Gerontol. 1991;46:M210–M215. doi: 10.1093/geronj/46.6.m210. [DOI] [PubMed] [Google Scholar]
- 23.Roberts RE, Kaplan GA, Shema SJ, Strawbridge WJ. Does growing old increase the risk for depression? Am J Psychiatry. 1997;154:1384–1390. doi: 10.1176/ajp.154.10.1384. [DOI] [PubMed] [Google Scholar]
- 24.Yu J, Li J, Cuijpers P, Wu S, Wu Z. Prevalence and correlates of depressive symptoms in Chinese older adults: a population-based study. Int J Geriatr Psychiatry. 2012;27:305–312. doi: 10.1002/gps.2721. [DOI] [PubMed] [Google Scholar]
- 25.Cho MJ, Lee JY, Kim BS, Lee HW, Sohn JH. Prevalence of the major mental disorders among the Korean elderly. J Korean Med Sci. 2011;26:1–10. doi: 10.3346/jkms.2011.26.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Statistics Korea. [accesseed on 1 August 2012]. Avaiable at https://www.index.go.kr/egams/stts/jsp/potal/stts/PO_STTS_IdxMain.jsp?idx_cd=1063&bbs=INDX_001.
- 27.OECD. Education at a Glance 2011: OECD Publishing. [accesseed on 1 August 2012]. Available at http://www.oecd-ilibrary.org/education/education-at-a-glance-2011_eag-2011-en.
- 28.Rotermann M. Marital breakdown and subsequent depression. Health Rep. 2007;18:33–44. [PubMed] [Google Scholar]
- 29.Sheeber L, Hops H, Alpert A, Davis B, Andrews J. Family support and conflict: prospective relations to adolescent depression. J Abnorm Child Psychol. 1997;25:333–344. doi: 10.1023/a:1025768504415. [DOI] [PubMed] [Google Scholar]
- 30.Ross CE, Mirowsky J. Sex differences in the effect of education on depression: resource multiplication or resource substitution? Soc Sci Med. 2006;63:1400–1413. doi: 10.1016/j.socscimed.2006.03.013. [DOI] [PubMed] [Google Scholar]
- 31.Cho SJ, Oh DH, Lee JA, Choi BY, Park YC, Nam JH. Prevalence of main psychiatric disorders in relation to urbanization in Gyeonggi Province by using the Korean Version of the Mini-International Neuropsychiatric Interview. J Korean Neuropsychiatr Assoc. 2011;50:288–296. [Google Scholar]
- 32.Peen J, Dekker J, Schoevers RA, Have MT, de Graaf R, Beekman AT. Is the prevalence of psychiatric disorders associated with urbanization? Soc Psychiatry Psychiatr Epidemiol. 2007;42:984–989. doi: 10.1007/s00127-007-0256-2. [DOI] [PubMed] [Google Scholar]
- 33.Dekker J, Peen J, Koelen J, Smit F, Schoevers R. Psychiatric disorders and urbanization in Germany. BMC Public Health. 2008;8:17. doi: 10.1186/1471-2458-8-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Peen J, Schoevers RA, Beekman AT, Dekker J. The current status of urban-rural differences in psychiatric disorders. Acta Psychiatr Scand. 2010;121:84–93. doi: 10.1111/j.1600-0447.2009.01438.x. [DOI] [PubMed] [Google Scholar]
- 35.Lin CH, Lee YY, Liu CC, Chen HF, Ko MC, Li CY. Urbanization and prevalence of depression in diabetes. Public Health. 2012;126:104–111. doi: 10.1016/j.puhe.2011.10.006. [DOI] [PubMed] [Google Scholar]