

Abstract
Social inequality in adverse birth outcomes has been demonstrated in several countries. The present study examined the separate and joint effects of parental education and work in order to investigate the causal pathways of social class effects on adverse birth outcomes in Korea. The occurrence of low birth weight, preterm births, and intrauterine growth retardation was examined among 7,766,065 births in Korea from 1995 to 2008. The effect of social inequality, as represented by parental education and work, was examined against adverse birth outcomes using multivariate logistic regression after controlling for other covariates. Parental education had the most significant and greatest effect on all three adverse outcomes, followed by parental work and employment, which had lesser effects. For adverse birth outcomes, the gap between educational levels increased steadily in Korea from 1995 to 2008. Throughout the analysis, the effect of maternal manual work on adverse birth outcomes was apparent in the study results. Given this evidence of social inequality in education and employment, social interventions should aim at more in-depth and distal determinants of health.
Keywords: Social Inequality, Parental Education, Parental Work, Parental Occupation, Birth Outcome Effect, Low Birth Weight, Preterm Birth, Intrauterine Growth Retardation
INTRODUCTION
In Korea, whereas the total birth rate has been decreasing, the rate of adverse birth outcomes, including low birth weight (LBW) and preterm birth (PTB), has increased (http://www.kostat.go.kr). Research on the cause of this increase has focused more on maternal age and maternal parity (http://www.mw.go.kr) than on more profound social changes.
Several risk factors for adverse birth outcomes have been reported, including LBW, PTB, and delayed fetal development, mostly concentrating on maternal conditions, including cigarette smoking, alcohol/drug use, small stature of the mother (low weight gain, low body mass index, and short stature), primiparity (multiple births), previous history (history of prior PTB or a history of giving birth to small babies), maternal nutrition, maternal diseases (e.g., pregnancy-induced hypertension, genitourinary infection, incompetent cervix, abruptio placentae, pre-eclampsia, metabolic diseases, chronic maternal stress, infection and inflammation, and hypercholesterolemia), other genetic issues, and work (1-12). However, most of these conditions upon pregnancy could have been the result of previous social conditions, and conventional risk factors for adverse birth outcomes could be the mediators of socioeconomic disparities (1). Thus, an investigation of the causal pathways and mechanisms of social inequalities in adverse birth outcomes would be valuable.
As indices of social inequality in health, adverse birth outcomes, including LBW (1-3), PTB (1, 2, 4, 12, 13), and intrauterine growth retardation (IUGR) (1, 11, 12), have been examined in many different parts of the world. In Korea, several studies have also focused on the effects of parental social class on LBW (14-16). However, most of these studies have focused on the separate effect of parental social class such as education on limited scores of adverse birth outcomes.
The exact mechanism of social inequality in adverse birth outcomes is unknown. Education and work can be important social class mediators, and, in particular, parental work and employment and its interactions with education need to be examined more closely as risk factors for adverse birth outcomes. This is especially true in research on the underlying reasons for the ever-increasing trends in adverse birth outcomes in Korea. This study investigated the interactive effects of parental education and parental work on four adverse birth outcomes (LBW, PT, PT-LBW, and IUGR) in order to examine the effects of social inequality on birth outcomes. Parental education was used as a proxy for social inequality and parental work as an intermediating factor to identify the causal pathways and mechanisms that underlie the association between social inequality and increased risks of adverse birth outcomes.
MATERIALS AND METHODS
Data
A population of 7,810,689 newborn babies was identified from the national birth registry of the Korean National Statistics Office for a fourteen-year period (1995 to 2008). From this population, the following inadequate cases were excluded. First, 43,934 cases with missing values for birth weight or gestational age were discarded. Second, according to the WHO definition of live birth, the records with birth weights of less than 500 g (41 cases) or gestational ages less than 22 weeks (28 cases) were removed. Finally, 621 cases that were outliers in terms of the fetal growth curve were deleted. The remaining 7,766,065 cases, 99.4% of the total population, were included in the final analysis.
Variables
In Korea, all births are required by law to be registered within one month either by parents, family members, doctors, midwives, or maternity nurses who delivered the children, or others at a community administrative office. Birth certificates should be completed either by the medical doctors, the person who delivered the child, or relatives. For hospital delivered cases, about 98% of registrations were completed by medical doctors (http://kostat.go.kr/portal/korea/kor_nw/2/1/index.board?bmode=read&aSeq=65172).
The information registered upon birth includes socio-demographic profiles of the parents (address, age, marital status, marriage date, marriage duration, education, occupation), maternity-related characteristics (parity of all births, parity of all live births, deaths of previous children), and demographic and biological profiles of the infant (gestational age, birth weight, birth order, birth plurality, birth date, place of birth, year of birth).
Based on this information, birth outcome was classified into four groups: low birth weight (LBW, < 2,500 g), preterm (PTB, < 37 weeks), preterm and low birth weight (PT-LBW, < 37 weeks and < 2,500 g), and intrauterine growth retardation (IUGR, ≥ 37 weeks and < 2,500 g).
As a proxy indicator of social inequality, this study used differences in levels of parental education. Education is known to indicate social class more clearly than any other proxy indicator (17, 18). Levels of parental education were categorized as: middle school education or lower (≤ 9 yr), high school education (10-12 yr), and university education or higher (≥ 13 yr).
Information about parental work was used as an intermediating factor of social inequality in adverse birth outcomes. Information about parental work was provided on the birth registration form by the parents, and coded according to the Korean Standard Classification of Occupations. Based on regrouping of parental occupation, the work variable was categorized into 3 groups, non-manual (legislators, senior officials, and managers, professionals, technicians and associates, professionals clerks), manual (service workers, sale workers, skilled agricultural, forestry, and fishery workers, craft and related trade workers, plant and machine operators and assembly workers, laborers), and economically inactive populations (students, the unemployed, housekeepers, and soldiers). Because education might determine work and employment, which, in return, would be mediating factors for social inequality in adverse birth outcomes, we attempted to combine the education and work variables.
Other risk factors, including infant sex, parental ages, multiple births, maternal parity, the death of previous children, and year of birth, were used as covariates. Parental ages were categorized into the following six groups: 25-29, 30-34, 35-39, 40-45, and ≥ 45. Multiple births were categorized into two groups: single and twins or more. Maternal parity was categorized into following three groups: first, second, and third or higher. History of death of previous children was dichotomized, yes/no. Ethnicity was not available in the dataset; however, Koreans are generally considered ethnically homogeneous. Information on marital status was not used because unmarried childbearing is rare in Korea.
Statistical methods
Multivariate logistic regression was used for the analysis of parental education effect on adverse birth outcomes, adjusting for parental ages, infant sex, multiple births, maternal parity, history of death of previous children, and year of birth.
Interactions between parental education and work were examined on the effects on adverse birth outcomes. Statistical associations were examined by calculating odds ratios for interactions between parental education and work after adjusting for infant sex, maternal age, parental age, multiple births, maternal parity, death of previous children, and year of birth. Two-way interactions between paternal education and maternal education, paternal education and paternal work, maternal education and maternal work, and paternal work and maternal work were investigated. Additionally, three-way interactions between parental education and parental work were investigated through an interaction test. A likelihood ratio was calculated between the model with interaction terms and the model without. The likelihood ratio statistic was used to test the evidence for an interaction between the effects of risk factors.
Time trends in the maternal age-adjusted rates of adverse birth outcomes from 1995 to 2008 were analyzed using a general linear model (SAS code: Proc GLM). The widening gap of the odds ratios' time trends in adverse birth outcomes between higher educational level and lower educational level from 1995 to 2008 was also explored, adjusting for parental age, infant sex, multiple births, maternal parity, and history of death of previous children. P < 0.05 was considered statistically significant.
RESULTS
The rates of adverse birth outcomes adjusted for maternal age are presented according to parental education, parental work, birth characteristics, and year of birth in Korea from 1995 to 2008 (Table 1 and Supplemental Table 1). The rates of adverse birth outcomes were higher for female infants, for older parents, for multiple births, for maternal parity ≥3, and for more than one death of a previous child. In particular, the rate of adverse birth outcomes tended to increase from 1995 to 2008 (Table 1).
Table 1.
Maternal age-adjusted rates of low birth weight, preterm birth, preterm birth and low birth weight, and intrauterine growth retardation according to parental education, parental work, and birth characteristics in Korea from 1995 to 2008
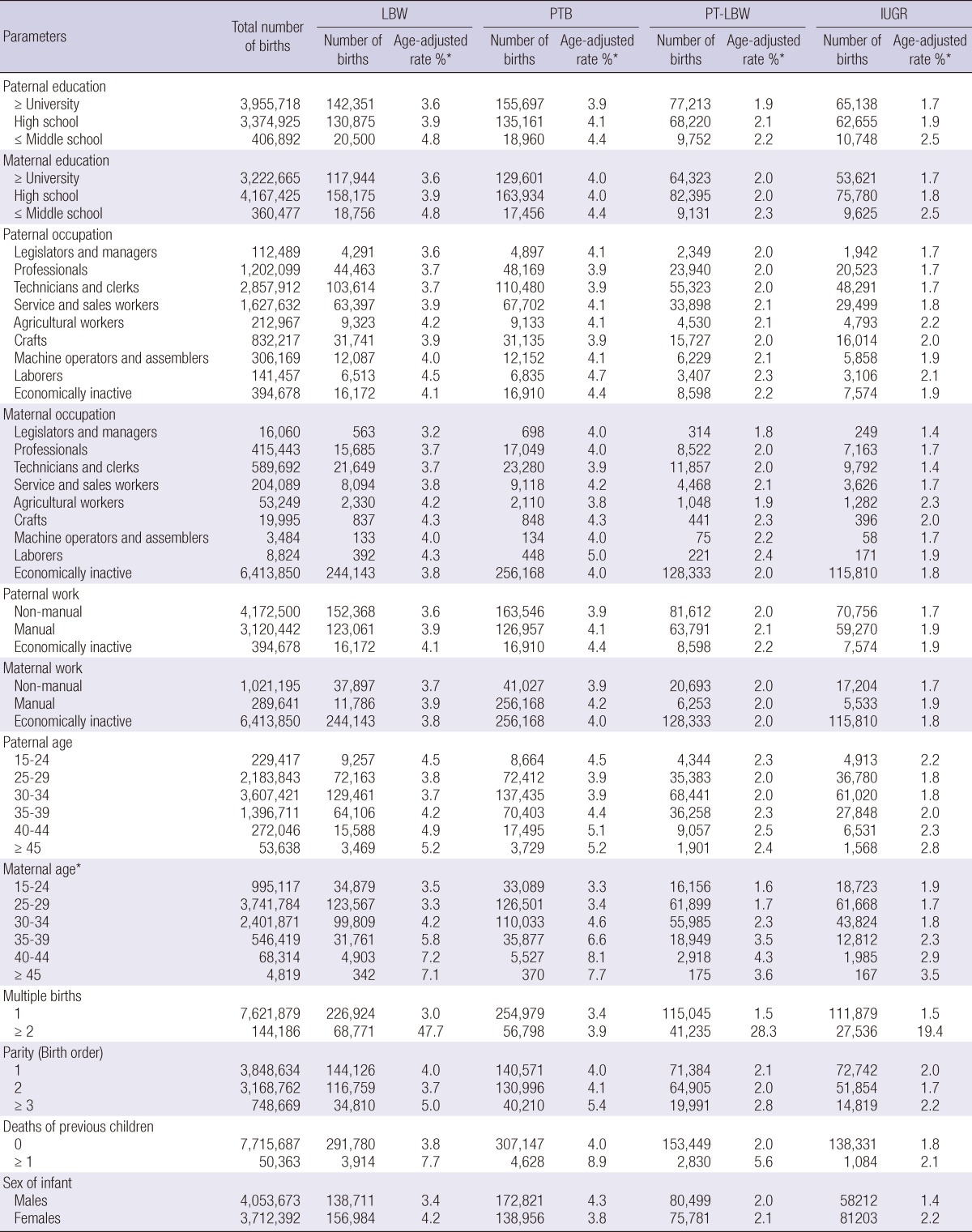
*All rates are adjusted for maternal age, with the exception of the maternal age categorical variable.
Effects of education
When we examined the effects of parental education, the maternal age-adjusted rates of adverse birth outcomes were higher with decreasing levels of education for both father and mother (Table 1). After adjusting for infant sex, parental age, maternal parity, multiple births, history of death of previous children, and year of birth, the odds ratios for four adverse birth outcomes among those parents with a middle school education or lower compared to those with a university education or higher were as follows for mothers and fathers, respectively: 1.56 (95% confidence interval, 1.54-1.59) and 1.62 (95% CI, 1.59-1.65) for LBW; 1.28 (95% CI, 1.26-1.3) and 1.32 (95% CI, 1.3-1.35) for PTB; 1.37 (95% CI, 1.34-1.40) and 1.45 (95% CI, 1.42-1.49) for PT-LBW; and 1.68 (95% CI, 1.64-1.71) and 1.70 (95% CI, 1.66-1.74) for IUGR.
Effects of work
Regarding parental work, the rates of adverse birth outcomes were higher when (comparing manual to non-manual workers) the father was economically inactive, while the rates were highest when the mother was engaged in manual work rather than economically inactive (Table 1). When we evaluated the detailed effects of occupation on adverse birth outcomes, occupations with the highest adverse birth outcomes differed according to four measures of adverse birth outcomes. The highest rates of LBW and IUGR were observed with maternal work in agricultural, forestry, and fishery jobs, while the highest rates of PTB and PT-LBW were observed when both father and mother were engaged in manual work (Table 2). In particular, physically demanding work, including laboring, agricultural, forestry, and fishery jobs, were highly related to LBW and PTB. Generally, employment of both fathers and mothers in manual work, including laborers, craft and related trade work, and plant and machine operation or assembly in the manufacturing industry as well as skilled agricultural, forestry, and fishery work in the agricultural sector were more highly associated with adverse birth outcomes (Table 2).
Table 2.
Adjusted odds ratios (95% confidence interval [CI]) of low birth weight (LBW), preterm birth (PTB), preterm birth and low birth weight (PT_LBW), and intrauterine growth retardation (IUGR) according to parental education, parental work, and birth characteristics in Korea from 1995 to 2008
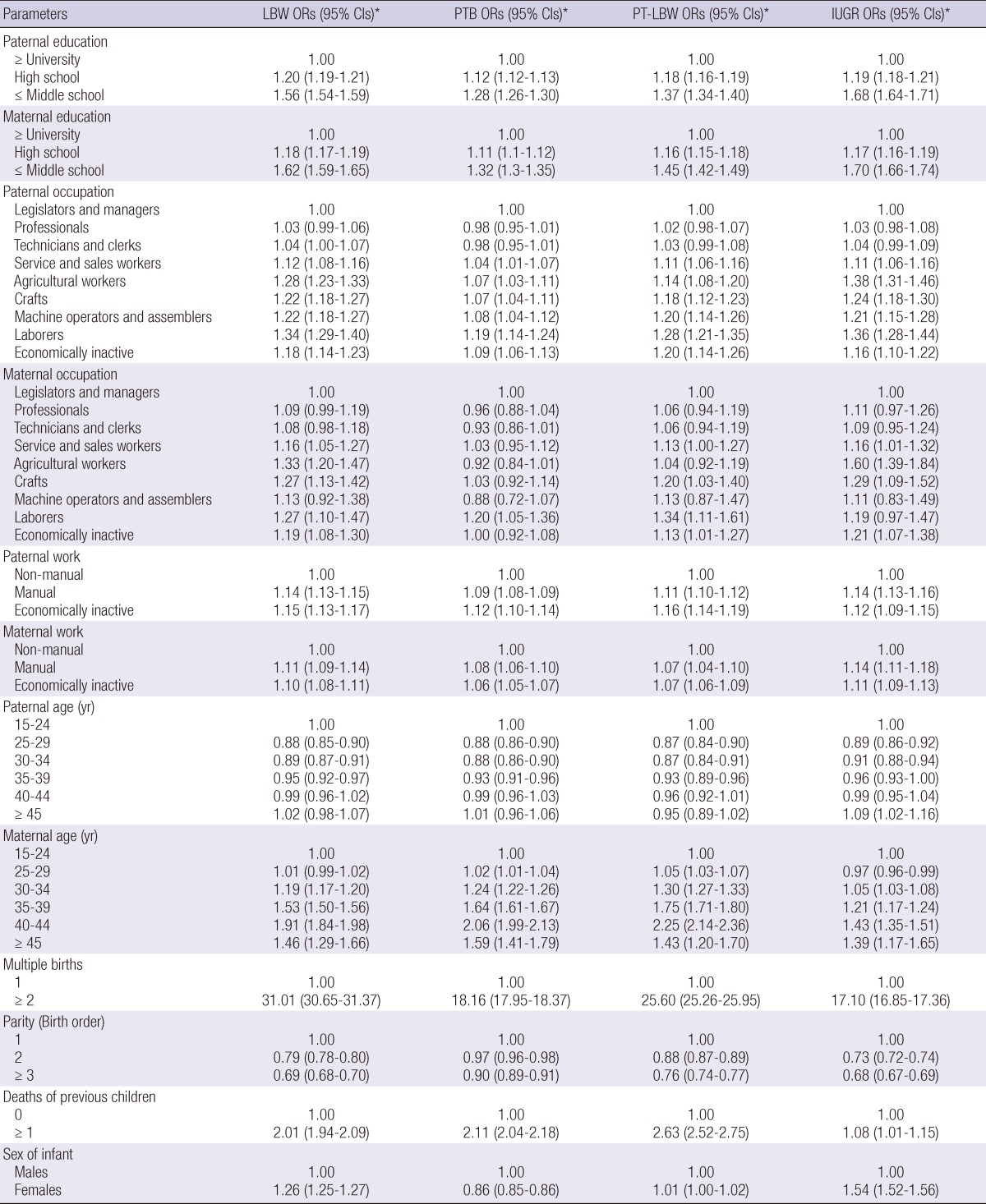
*The odds ratios (OR) for parental education, occupation, and work were calculated from each logistic regression model fitted after adjusting for infant sex, maternal age, parental age, multiple births, parity, death of previous children, and year of birth. In addition, the odds ratios for paternal age, maternal age, multiple births, parity (birth order), deaths of previous children, and sex of infant were calculated from each logistic regression model fitted after adjusting for infant sex, maternal age, parental age, multiple births, parity, death of previous children, and year of birth, parental education, occupation, and work.
Interactions between education and work
In terms of interactive effects, there were also significant interactions between parental education and parental work in their associations with adverse birth outcomes (log-likelihood test, P < 0.001 for all interactions in this study). The intermediating effects of parental education and parental work on adverse birth outcomes are presented in Tables 3-5.
Table 3.
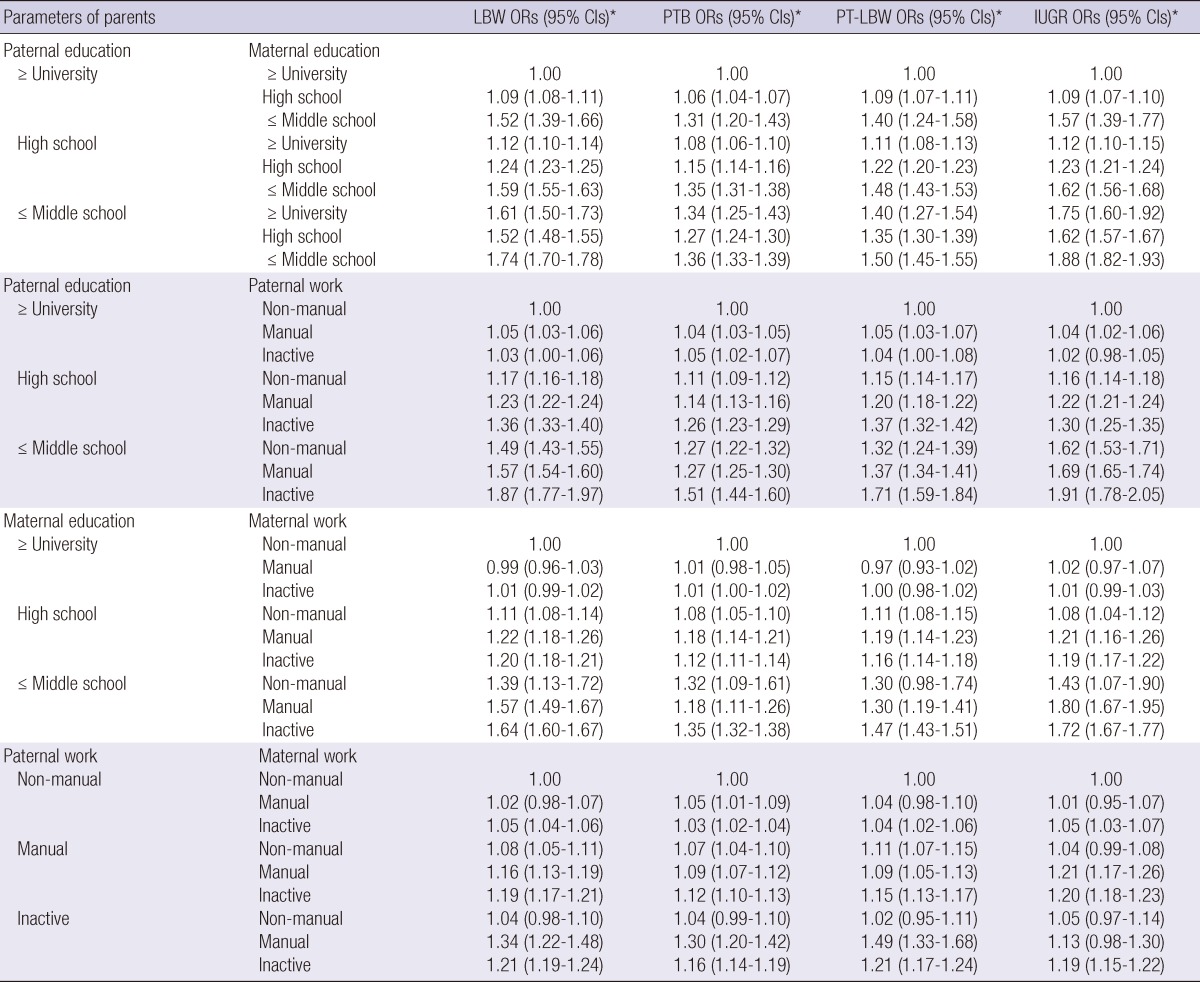
Adjusted odds ratios (95% confidence interval [CI]) of low birth weight (LBW), preterm birth (PTB), preterm birth and low birth weight (PT_LBW), and intrauterine growth retardation (IUGR) by two-way interactions of parental education and parental work in Korea from 1995 to 2008
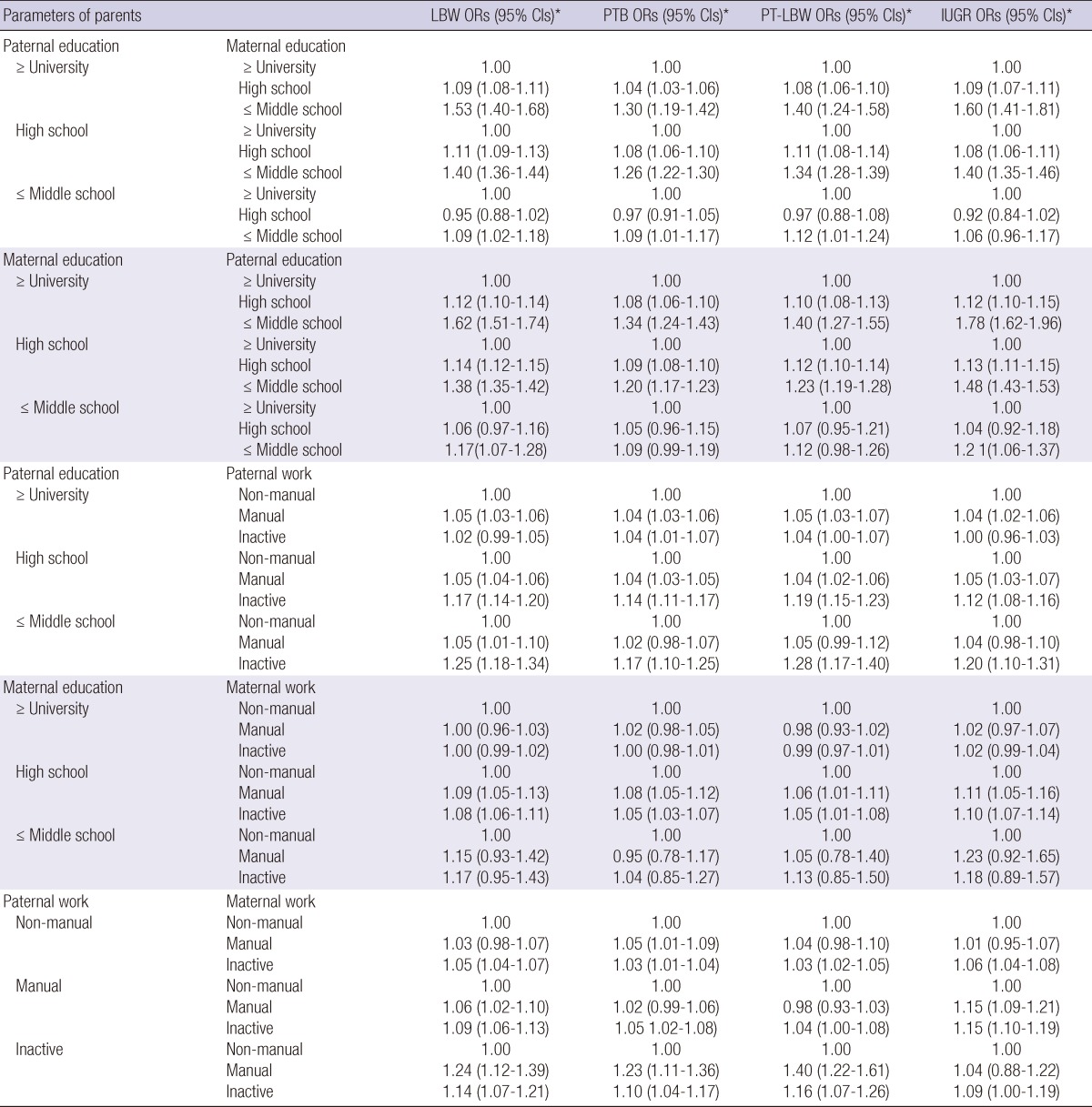
*ORs: Adjusted for infant sex, maternal age, parental age, multiple births, parity, death of previous children, and year of birth.
Table 5.
Adjusted odds ratios (95% confidence interval [CI]) of low birth weight (LBW), preterm birth (PTB), preterm birth and low birth weight (PT_LBW), and intrauterine growth retardation (IUGR) by three-way interactions of parental education and parental work in Korea from 1995 to 2008
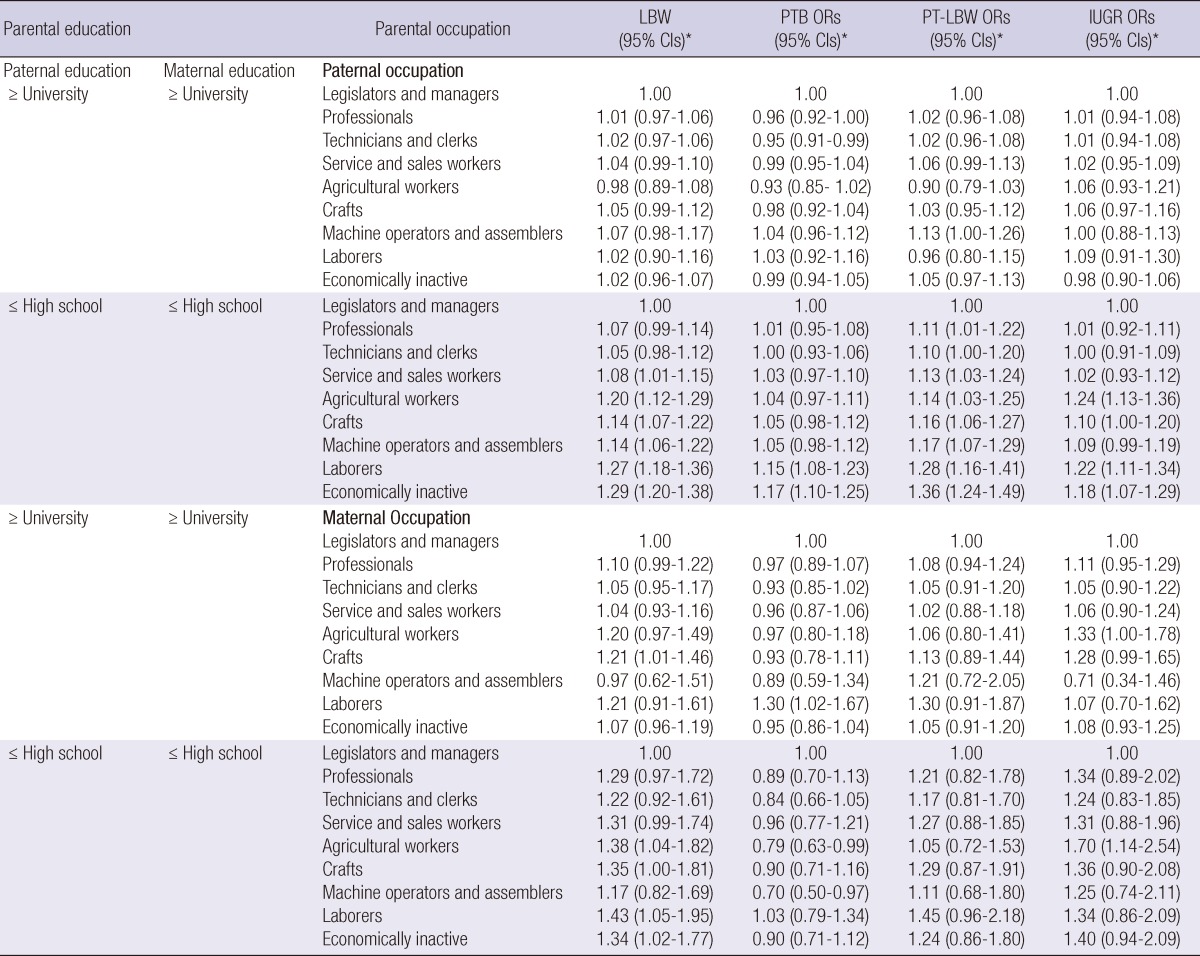
*ORs: Adjusted for infant sex, maternal age, parental age, multiple birth, parity, death of previous children, and year of birth.
When analyzed separately, social inequality in adverse birth outcomes showed similar patterns between paternal and maternal educational disparities (Table 2). However, when analyzed together, the effect of paternal education tended to be greater than that of maternal education (Table 3).
When one of the parents' education level was above high school, the education effect of the spouse on adverse birth outcomes was significant, while the effect of the spouse's education was not significant when the education level of the other parent was middle school or lower (Table 3). Moreover, the effect of maternal education on adverse birth outcomes disappeared with the lowest level of paternal education, while the effect of paternal education remained unchanged regardless of maternal education (Table 3).
As shown in Table 4, the risk of adverse birth outcomes was higher among parents with an educational level below middle school. There was a strong inverse relationship between adverse birth outcomes and the combination of both parents' educational level. The risk of adverse birth outcomes increased as the combination of both parents' educational level decreased.
Table 4.
Adjusted odds ratios (95% confidence interval [CI]) of low birth weight (LBW), preterm birth (PTB), preterm birth and low birth weight (PT_LBW), and intrauterine growth retardation (IUGR), considering the combined effects of paternal education and parental work in Korea from 1995 to 2008
*ORs: Adjusted for infant sex, maternal age, parental age, multiple birth, parity, death of previous children, and year of birth.
There was also an interaction between parental education and parental work (Table 3). When paternal education and work were analyzed together, the risk of adverse birth outcomes was higher among fathers who had a middle school education or lower and were economically inactive. In terms of maternal education and work, the risk was higher among mothers who had a middle school education or lower and were economically inactive or performing manual work (Table 3).
After stratifying according to paternal and maternal work, the risk of adverse birth outcomes was higher when the father was economically inactive and the mother was performing manual work, as well as when both parents were economically inactive (Table 3). When we combined parental education and parental work and organized them in order, the effects of social inequality became more profound when paternal education was lower, when parents were less educated and in the manual labor or economically inactive group, when fathers were economically inactive with mothers performing manual work, or when both parents were economically inactive (Table 4).
Table 5 shows the results of three-way interactions between parental education and parental work on adverse birth outcomes. When both the paternal and maternal educational status was university-level, the effect of work on adverse birth outcomes did not differ among legislators, senior officials, and managers. That is, no effect of work was found in mothers and fathers with a university-level education. In contrast, laborers and those who were economically inactive had higher risks of adverse birth outcomes when the paternal and maternal educational level was high school, middle school, or lower. This result is similar to those seen for mothers (Table 5).
Time trends
The maternal age-adjusted rates of LBW, PTB, and PT-LBW increased each year (P < 0.001 for LBW, PTB, and PT-LBW), while the rate of IUGR remained constant (P = 0.051) (Fig. 1). The increases in the rates of LBW, PTB, and PT-LBW remained significant after adjusting for infant sex, maternal age, parental age, multiple births, parity, and death of previous children; however, the rates of IUGR decreased each year after adjustment (Supplemental Table 2).
Fig. 1.

Maternal age adjusted rates of low birth weight (LBW), preterm birth (PTB), preterm birth and low birth weight (PT_LBW), and intrauterine growth retardation (IUGR in Korea from 1995 to 2008. *Test for trend: P < 0.001 for LBW, PTB, PT-LBW, P = 0.051 for IUGR.
Fig. 2 shows the odds ratios of adverse birth outcomes, after adjustment for infant sex, maternal age, parental age, multiple birth, parity, death of previous children, and year of birth, in Korea from 1995 to 2008. The annual changes in the adjusted odds ratios of parents with a lower educational level (e.g., high school and middle school or lower) compared to those with a university-level education showed significantly increasing trends for PTB (P < 0.001) and PT-LBW (P < 0.05). For LBW, there were no increasing trends for lower educational level among fathers, whereas significant increases for LBW were found among mothers with less than a middle school education (P = 0.008). However, no significantly decreasing trend for IUGR was identified for lower paternal educational levels (Fig. 2).
Fig. 2.

Adjusted odds ratios of low birth weight (LBW), preterm birth (PTB), preterm birth and low birth weight (PT_LBW), and intrauterine growth retardation (IUGR), adjusting for infant sex, maternal age, parental age, multiple births, parity, death of previous children, and year of birth in Korea from 1995 to 2008.
One interesting finding is that the gaps in the odds ratios for PTB and PT-LBW between university and middle school or lower (P < 0.001) and between university and high school (P < 0.05) broadened over time, but not between university and high school among fathers (P = 0.149), while no widening gaps in the odds ratios for LBW between different educational levels were found. However, the gaps in the odds ratios for IUGR among different parental educational levels were unchanged over time, and even decreased between university and middle school or lower among fathers (P = 0.040) (Fig. 2).
DISCUSSION
Social inequality was observed in all four adverse birth outcomes examined: LBW, PTB, PT-LBW, and IUGR. In particular, significant differences in IUGR, which have been addressed in only a few studies, were observed (1).
The risk factors for adverse birth outcomes were shown to be different for different socioeconomic groups. Kramer et al. (1) reviewed the mediators of socioeconomic disparities in IUGR, including cigarette smoking, low gestational weight gain and short stature, alcohol and drug abuse, and maternal work and physical activity, as well as the mediators of socioeconomic disparities in PTB, including socioeconomic gradients in bacterial vaginosis and cigarette smoking, cocaine use, and prolonged standing or other adverse working conditions (1). Our study results confirm that a lower education level, manual work, and insecure employment, which are the socioeconomic hallmarks of material deprivation, should have been reflected by fetal undernutrition, resulting in disproportionate fetal growth as a pathway of social inequality.
The effects of educational level were stronger for fathers than for mothers, possibly reflecting the bias of Korean society, which is male-dominated, with paternal education operating as a stronger social class determinant for a family. Upon closer examination of the interactive effects of paternal and maternal education, when one of the parents' education was lower than middle school, the effect of the other parent's education on adverse birth outcomes was not different, implying that a lower level of education for either parent is a crucial and dominant risk factor for adverse birth outcomes regardless of the other parent's education status.
In this study, we also found significant interactions between parental education and work. For parents with higher educational backgrounds, the effect of their work and employment status on adverse birth outcomes was minimal. However, for parents with lower educational backgrounds, parents in an economically inactive state had the highest rates of adverse birth outcomes, followed by parents in manual work, and finally those doing non-manual work. This result suggests that some parents in the highly educated group could live without doing work or economic activity, possibly with aid from family members (e.g., an inheritance). The most vulnerable population for adverse birth outcomes was those engaged in manual work or in an economically inactive state with an educational level of less than middle school, and probably with no inheritance or other social safety net.
Our data suggest that maternal manual work was associated with a higher risk of adverse birth outcomes. Maternal work and physical activity are mediating factors of socioeconomic disparities in adverse birth outcomes such as IUGR (1). Strenuous work and physical activity during pregnancy is associated with a risk of PTB (1). Pregnant women whose jobs require manual work, including prolonged standing, walking, or other physically demanding tasks, tend to be of lower socioeconomic status than women in more sedentary jobs (19-24).
Regarding the changes over time, our data suggest that the rates of LBW, PTB, and PT-LBW increased over the period studied, and that social inequalities in LBW, PTB, and PT-LBW rose concomitantly. However, IUGR showed no such trend. The gap between those with a high or middle school education or lower and those with a university education became wider for PTB, LBW, and PT-LBW in terms of the outcome rates (Fig. 2 and Supplemental Tables 1 and 2).
Maternal age and multiparity have been cited as risk factors for increased rates of LBW and PTB (25-28). The Korean government also regards maternal age and multiple births as major reasons for the increased rate of adverse birth outcomes (http://momplus.mw.go.kr). However, even after controlling for maternal age and multiparity, the rates of adverse birth outcomes increased significantly among parents in the less educated groups and those performing manual work as well as those in economically inactive states. Moreover, the expansion in social inequality could have contributed to the increased rates of adverse birth outcomes. In particular, the downgrading of employed women of lower social classes to unskilled and manual work with very low wages, and of those who were "driven out of the house" and forced to participate in the labor market because of the rapidly increased risk of unemployment or wage reductions for their husbands since the economic crisis of 1997 (17, 22, 27, 29-31), may have contributed to the increased risk of adverse birth outcomes. Additionally, the increasing trend in manual work among lesser educated women could increase social inequality in terms of birth outcomes (18). Furthermore, the resulting increase in social polarization may have contributed to the increasing social inequality in adverse birth outcomes. Since Korea experienced an economic crisis at the end of 1997, (32) unemployment (33), absolute poverty (34), and the number of contingent and casual workers has increased. The Gini coefficient increased from 0.283 in 1997 to 0.337 in 2006, indicating aggravated socioeconomic polarization in Korean society (35).
In conclusion, this study shows that social inequalities in adverse birth outcomes in terms of LBW, PTB, PTB-LBW, and IUGR exist in Korea, and that the gap in adverse birth outcomes between educational levels increased over time in Korea from 1995 to 2008. This study indicates that the most vulnerable population in terms of adverse birth outcomes was those doing manual work or in an economically inactive state with a middle school education or lower. Tackling social inequality in terms of education and work should reduce the risk of adverse birth outcomes in Korea.
A major strength of our study is that it used Korean national birth registry data from 1995 to 2008. Thus, our data represent a comprehensive picture of social inequalities in adverse birth outcomes for the entire birth cohort in Korea from 1995 to 2008. Our study has several limitations. First, the national birth registration data might have omitted some cases of neonatal death (i.e., those who were born alive but not registered) because parents might be reluctant to report such cases. Such omitted reports may be related to adverse birth outcomes, which would result in underestimation of the actual rates. Second, misclassification of education due to information bias in national birth registration data might cause non-differential or differential misclassification, which could cause bias in either direction. Third, we were unable to take into account any changes in educational level from 1995 to 2008; the educational status of the participants may have changed during this period. Further investigation of the detailed mechanisms and processes linking class relationships and health is needed, using both detailed longitudinal studies as well as life course studies.
In this study, we demonstrated social inequalities in the rates of LBW, PTB, PTB-LBW, and IUGR between 1995 and 2008 in Korea. Interestingly, the annual changes in LBW, PTB, and PTB-LBW, but not IUGR, increased with widening social inequality. The social inequality in adverse birth outcomes increased as Korea experienced an economic crisis at the end of 1997. Our findings indicate that the most vulnerable population for adverse birth outcomes was engaged in manual work or in an economically inactive state with a less than a middle school education. Maternal manual employment was associated with the highest risk of adverse birth outcomes.
ACKNOWLEDGMENTS
The authors have no conflicts of interest to disclose.
Footnotes
This study was supported by the Korea Research Foundation Grant funded by the Korean Government (MOEHRD) (KRF-2002-015-EP0079).
Supplementary Material
References
- 1.Kramer MS, Seguin L, Lydon J, Goulet L. Socio-economic disparities in pregnancy outcome: why do the poor fare so poorly? Paediatr Perinat Epidemiol. 2000;14:194–210. doi: 10.1046/j.1365-3016.2000.00266.x. [DOI] [PubMed] [Google Scholar]
- 2.Sanjose S, Roman E, Beral V. Low birthweight and preterm delivery, Scotland, 1981-84: effect of parents' occupation. Lancet. 1991;338:428–431. doi: 10.1016/0140-6736(91)91045-v. [DOI] [PubMed] [Google Scholar]
- 3.Rodriguez C, Regidor E, Gutierrez-Fisac JL. Low birth weight in Spain associated with sociodemographic factors. J Epidemiol Community Health. 1995;49:38–42. doi: 10.1136/jech.49.1.38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Olsen P, Laara E, Rantakallio P, Jarvelin MR, Sarpola A, Hartikainen AL. Epidemiology of preterm delivery in two birth cohorts with an interval of 20 years. Am J Epidemiol. 1995;142:1184–1193. doi: 10.1093/oxfordjournals.aje.a117577. [DOI] [PubMed] [Google Scholar]
- 5.Gruenwald P, Funakawa H, Mitani S, Nishimura T, Takeuchi S. Influence of environmental factors on foetal growth in man. Lancet. 1967;1:1026–1028. doi: 10.1016/s0140-6736(67)91541-3. [DOI] [PubMed] [Google Scholar]
- 6.Butler NR, Alberman ED. Perinatal problems: the second report of the 1958 British perinatal mortality survey under the auspices of the national birthday trust fund. Edinburgh: Livingstone; 1969. [Google Scholar]
- 7.Eastman NJ, Jackson E. Weight relationships in pregnancy. I. The bearing of maternal weight gain and pre-pregnancy weight on birth weight in full term pregnancies. Obstet Gynecol Surv. 1968;23:1003–1025. [PubMed] [Google Scholar]
- 8.Mengert WF. Fetal and neonatal mortality cause and prevention. Am J Obstet Gynecol. 1948;55:660–668. doi: 10.1016/0002-9378(48)90121-5. [DOI] [PubMed] [Google Scholar]
- 9.Anderson NA, Brown EW, Lyon RA. Cause of prematurity. Am J Dis Child. 1941;61:72. doi: 10.1001/archpedi.1946.02020310055004. [DOI] [PubMed] [Google Scholar]
- 10.Shwartz S. Prenatal care, prematurity, and neonatal mortality. A critical analysis of prenatal care statistics and associations. Am J Obstet Gynecol. 1962;83:591–598. doi: 10.1016/s0002-9378(16)35888-4. [DOI] [PubMed] [Google Scholar]
- 11.Robinson JS, Moore VM, Owens JA, McMillen IC. Origins of fetal growth restriction. Eur J Obstet Gynecol Reprod Biol. 2000;92:13–19. doi: 10.1016/s0301-2115(00)00421-8. [DOI] [PubMed] [Google Scholar]
- 12.Rogers LK, Velten M. Maternal inflammation, growth retardation, and preterm birth: insights into adult cardiovascular disease. Life Sci. 2011;89:417–421. doi: 10.1016/j.lfs.2011.07.017. [DOI] [PubMed] [Google Scholar]
- 13.Ancel PY, Saurel-Cubizolles MJ, Di Renzo GC, Papiernik E, Breart G Europop Group. Social differences of very preterm birth in Europe: interaction with obstetric history. Am J Epidemiol. 1999;149:908–915. doi: 10.1093/oxfordjournals.aje.a009734. [DOI] [PubMed] [Google Scholar]
- 14.Lee SY, Hong SC. Difference in incidence rate of low birth weight among the parental social strata in Korea. Health Soc Sci. 2003;13:61–79. [Google Scholar]
- 15.Park JH, Lee BE, Park HS, Ha EH, Lee SW, Kim YJ. Association between pre-pregnancy body mass index and socioeconomic status and impact on pregnancy outcomes in Korea. J Obstet Gynaecol Res. 2011;37:138–145. doi: 10.1111/j.1447-0756.2010.01332.x. [DOI] [PubMed] [Google Scholar]
- 16.Son M. The effects of the parents' social class on low birthweight among the birth, 1995-2001. Korean J Health Policy Adm. 2004;14:148–168. [Google Scholar]
- 17.Hwang S, Jang J. The relationship between the supply and policy change in women's labour. Seoul, Korea: Korea Labour Institute; 2003. [Google Scholar]
- 18.Son M. Occupational class and health: the differentials in mortality, morbidity and workplace injury rates by occupation, education, income and working conditions in Korea. London School of Hygiene & Tropical Medicine, University of London; 2001. pp. 244–268. PhD thesis. [Google Scholar]
- 19.Mamelle N, Laumon B, Lazar P. Prematurity and occupational activity during pregnancy. Am J Epidemiol. 1984;119:309–322. doi: 10.1093/oxfordjournals.aje.a113750. [DOI] [PubMed] [Google Scholar]
- 20.Saurel-Cubizolles MJ, Kaminski M. Pregnant women's working conditions and their changes during pregnancy: a national study in France. Br J Ind Med. 1987;44:236–243. doi: 10.1136/oem.44.4.236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.McDonald AD, McDonald JC, Armstrong B, Cherry NM, Nolin AD, Robert D. Prematurity and work in pregnancy. Br J Ind Med. 1988;45:56–62. doi: 10.1136/oem.45.1.56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Homer CJ, Beresford SA, James SA, Siegel E, Wilcox S. Work-related physical exertion and risk of preterm, low birthweight delivery. Paediatr Perinat Epidemiol. 1990;4:161–174. doi: 10.1111/j.1365-3016.1990.tb00634.x. [DOI] [PubMed] [Google Scholar]
- 23.Henriksen TB, Hedegaard M, Secher NJ. Standing and walking at work and birthweight. Acta Obstet Gynecol Scand. 1995;74:509–516. doi: 10.3109/00016349509024380. [DOI] [PubMed] [Google Scholar]
- 24.Hickey CA, Cliver SP, Mulvihill FX, McNeal SF, Hoffman HJ, Goldenberg RL. Employment-related stress and preterm delivery: a contextual examination. Public Health Rep. 1995;110:410–418. [PMC free article] [PubMed] [Google Scholar]
- 25.Kim YA, Park JH. Impact of changes in maternal age and parity distribution on low birth weight incidence rate. Korean J Prev Med. 1989;22:276–282. [Google Scholar]
- 26.Park MS, Park SH, Han JH, Kim EI. A study on factors affecting on low birth weight infants. J Reprod Med Popul. 1996;9:5–14. [Google Scholar]
- 27.Park SH, Han JH, Kim SM, Ku SY, Kim SH. Risk factors of preterm delivery in pregnant women aged 35 years or older: analysis of birth certificate data in 1996. Korean J Obstet Gynecol. 1999;42:1416–1421. [Google Scholar]
- 28.Romo A, Carceller R, Tobajas J. Intrauterine growth retardation (IUGR): epidemiology and etiology. Pediatr Endocrinol Rev. 2009;6(Suppl 3):332–336. [PubMed] [Google Scholar]
- 29.Launer LJ, Villar J, Kestler E, de Onis M. The effect of maternal work on fetal growth and duration of pregnancy: a prospective study. Br J Obstet Gynaecol. 1990;97:62–70. doi: 10.1111/j.1471-0528.1990.tb01718.x. [DOI] [PubMed] [Google Scholar]
- 30.Teitelman AM, Welch LS, Hellenbrand KG, Bracken MB. Effect of maternal work activity on preterm birth and low birth weight. Am J Epidemiol. 1990;131:104–113. doi: 10.1093/oxfordjournals.aje.a115463. [DOI] [PubMed] [Google Scholar]
- 31.Klebanoff MA, Shiono PH, Carey JC. The effect of physical activity during pregnancy on preterm delivery and birth weight. Am J Obstet Gynecol. 1990;163:1450–1456. doi: 10.1016/0002-9378(90)90604-6. [DOI] [PubMed] [Google Scholar]
- 32.Oh EJ, Min HJ, Kim JH. Career choice and labor market transition of the married women by level of education. J Vocat Educ Train. 2009;12:141–162. [Google Scholar]
- 33.Kim MR. The change of people's life during 6 years of neoliberalism. 95, Situation and Labor, Korean Institute of Labor Study and Policy. Seoul, Korea: 2004. pp. 1–59. [Google Scholar]
- 34.Kim AE. The social perils of the Korean financial crisis. J Contemp Asia. 2004;34:221–237. [Google Scholar]
- 35.Shin KY. Inequalities in social class in Korea. Econ Soc. 2003;59:32–54. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.