

Abstract
Background:
It is difficult to visualise the larynx using conventional laryngoscopy in the presence of cervical spine immobilisation. Airtraq® provides for easy and successful intubation in the neutral neck position.
Objective:
To evaluate the effectiveness of Airtraq in comparison with the Mc Coy laryngoscope, when performing tracheal intubation in patients with neck immobilisation using hard cervical collar and manual in-line axial cervical spine stabilisation.
Methods:
A randomised, cross-over, open-labelled study was undertaken in 60 ASA I and II patients aged between 20 and 50 years, belonging to either gender, scheduled to undergo elective surgical procedures. Following induction and adequate muscle relaxation, they were intubated using either of the techniques first, followed by the other. Intubation time and Intubation Difficulty Score (IDS) were noted using Mc Coy laryngoscope and Airtraq. The anaesthesiologist was asked to grade the ease of intubation on a Visual Analogue Scale (VAS) of 1–10. Chi-square test was used for comparison of categorical data between the groups and paired sample t-test for comparison of continuous data. IDS score and VAS were compared using Wilcoxon Signed ranked test.
Results:
The mean intubation time was 33.27 sec (13.25) for laryngoscopy and 28.95 sec (18.53) for Airtraq (P=0.32). The median IDS values were 4 (interquartile range (IQR) 1–6) and 0 (IQR 0–1) for laryngoscopy and Airtraq, respectively (P=0.007). The median Cormack Lehane glottic view grade was 3 (IQR 2–4) and 1 (IQR 1–1) for laryngoscopy and Airtraq, respectively (P=0.003). The ease of intubation on VAS was graded as 4 (IQR 3–5) for laryngoscopy and 2 (IQR 2–2) for Airtraq (P=0.033). There were two failures to intubate with the Airtraq.
Conclusion:
Airtraq improves the ease of intubation significantly when compared to Mc Coy blade in patients immobilised with cervical collar and manual in-line stabilisation simulating cervical spine injury.
Keywords: Airtraq®, Mc Coy laryngoscope, immobilization, cervical spine injury
INTRODUCTION
It is a significant challenge even to the most experienced anaesthesiologist to intubate patients in whom the movement of the cervical spine is not desirable or restricted. In cases of cervical spine immobility or instability, the use of direct laryngoscopy is reserved: it requires flexion of the cervical spine and atlanto-occipital extension for alignment of the oral, pharyngeal and laryngeal axis to create a direct line of vision from the mouth to the vocal cords. Tracheal intubation in patients with suspected neck injuries should achieve two contradicting goals: sufficient laryngeal exposure and the least cervical spine movement. As the former involves movement of the cervical vertebrae, intubation has to be performed using cervical spine immobilisation to prevent exacerbation of spinal cord injuries. Protective measures to avoid deleterious compression forces on the spinal column include application of rigid collar, a forehead tape and manual-in-line stabilisation (MILS). Application of cervical collars may reduce cervical spine movements, but it hinders tracheal intubation with the standard laryngoscope. The cervical collar also significantly reduces the mouth opening, rendering laryngoscopy difficult.[1] Besides, the neck collar lifts up the chin and tips the larynx anteriorly.[2] Removing the anterior portion of the collar can facilitate tracheal intubation. However, this jeopardises the safety of the cervical spine. MILS that is recommended for cervical spine immobilisation further impairs glottic visualisation.[3]
Fibreoptic intubation is the most reliable method in patients with cervical trauma, but it may be difficult in patients with restricted neck movement.[4] The other drawbacks of fiberoptic intubation are lack of availability of equipment, requires lack of expertise in its use and difficulty in using it if the patient is not co-operative or if there is blood or secretions in the airway.
The unique curving blade of the Airtraq® is designed to fit the oropharyngeal anatomy. It possesses considerable advantages in the setting of cervical spine immobilisation[5] when direct laryngoscopy is difficult or not recommended.[6] It provides a full view of the glottis without requiring to align the airway axis. In addition, the Airtraq® laryngoscope also appears to cause less cervical spine movements during tracheal intubation when compared with the Macintosh or Mc Coy® laryngoscopes.[7] The Airtraq facilitates tracheal intubation with the neck in neutral position, which is similar to the neck position maintained by a rigid cervical collar.[8] However, a rigid cervical collar in combination with forehead strapping and MILS virtually obliteratess even the small neck movements which normally facilitate airway insertion. The efficacy of the Airtraq has not been determined in this setting.
The present study evaluates the efficacy of Airtraq in patients undergoing cervical spine immobilisation with rigid cervical collar and MILS, simulating the situation of cervical trauma, and compares it with the Mc Coy laryngoscope.
METHODS
The study was designed as an open-labelled, randomised, cross-over trial. Following Institutional Ethics Committee's (IEC) approval, informed consent was obtained from 60 ASA I and II patients, aged between 18 and 50 years, belonging to either gender and undergoing elective surgery requiring general anaesthesia with oral endotracheal intubation. Patients with anticipated difficult airway (Mallampatti grade IV, mentohyoid distance (MHD) <3 cm, thyromental distance (TMD) <5 cm, sternomental distance (SMD) <10 cm, neck circumference >42 cm), obese (body mass index (BMI) >30) patients, patients with risk of pulmonary aspiration of gastric contents, pregnant patients, and patients with cervical spine pathology, airway distortion or trauma were excluded from the study.
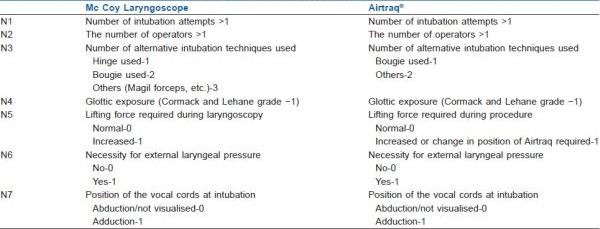
An appropriate-sized rigid cervical collar (Ambulance Collar, MGRM Medicare Limited, hyderabad, India) was placed as per manufacturer's instructions. Mouth opening was measured before and after its application. All the patients received a standardised general anaesthetic. Standard monitoring included ECG, non-invasive arterial pressure, SpO2, and measurement of end-tidal carbon dioxide. Before induction of anaesthesia, all patients were given fentanyl 1–1.5 μg/kg and glycopyrrolate 5 μg/kg i.v. MILS was applied by the neurosurgeon not involved in the study. Patients were induced with pentothal sodium 5 mg/kg. After induction of anaesthesia, all patients were manually ventilated with sevoflurane 2.0–2.5% in oxygen, and vecuronium 0.1 mg/kg was administered. Difficulty in mask ventilation was noted. Intubation was attempted after 5 min to obtain optimal intubating conditions. Each patient was intubated twice, once using Airtraq and the other time with Mc Coy laryngoscope. Patients were randomised using online randomisation (http: //www.randomization.com) to undergo Airtraq intubation first or intubation with Mc Coy first to reduce the influence of one intubation on the other. Anaesthesiologists with adequate experience (>40 intubations) in both techniques performed all intubations. The trachea was intubated with a 7.5-mm tracheal tube in females and an 8.0-mm tracheal tube in males. In case of Mc Coy, if Cormack Lehane Grade 1 or 2, intubation proceeded without using hinge of the laryngoscope. If Cormack Lehane Grade >2, then hinge of Mc Coy was used to improve laryngeal visualisation. If glottic view did not improve even with hinge, an intubating bougie was used. The ease of introduction of Mc Coy blade or Airtraq in the presence of collar was graded for both techniques on a Likert scale[9] from –2 to +2. A modification Intubation Difficulty Score (IDS) described by Adnet and colleagues[10] to suit Mc Coy and Airtraq aided intubation as given in Appendix 1 was noted. All the manoeuvres and devices used for intubation were included in the modified IDS. The intubation time (time from removal of face mask for intubation to successful intubation and connection of circuit to the endotracheal tube) was noted for both techniques. The intubating anaesthesiologist graded the ease of intubation for both techniques on a visual analogue scale from 1 to 10, 10 being most difficult or failed intubation and 1 being very easy intubation. If introduction of the intubating device was not possible or there were more than three attempts for intubation or intubation time was more than 120 sec, it was considered to be a failure. The IDS before abandoning the technique was noted. Intubation was then performed with the second technique. In case of failure with the second technique also, cervical collar was removed and intubation proceeded. Failure to intubate (>3 attempts or >120 sec), episodes of desaturation (SpO2 < 90%) and airway trauma (blood seen on lips teeth or oral mucosa or the device) during intubation were noted.
Statistical analysis
We based our sample size estimation on the IDS score. An IDS score of 0–1 represents ideal intubating conditions. Based on initial pilot studies, we projected an IDS score of 2 or greater in 73% patients with the Mc Coy laryngoscope. A clinically important reduction in the number of patients with an IDS score greater than 2 in these low-risk patients would be a 50% reduction. Based on these figures, using α=0.05 and β=0.2, we estimated that 54 patients would be required. We therefore aimed to enrol 60 patients per group.
Statistical analysis was performed using SPSS version 13. Continuous data are presented as mean±SD, ordinal data as median with interquartile range (IQR), and categorical data are presented as frequency and proportions. Categorical data were compared between Airtraq and Mc Coy laryngoscope using Chi-square test. Ordered categorical data like IDS score were compared using Wilcoxon Signed ranked test and continuous data compared using paired sample t-test. The significance level for all analyses was set as P<0.05.
RESULTS
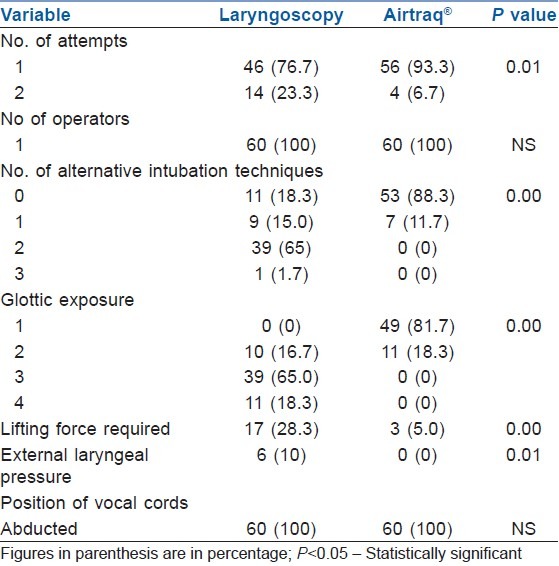
A total of 60 patients were enrolled in the study. There were no exclusions after recruitment. The demographic and baseline airway parameters are shown in Table 1. There was a significant reduction in mouth opening following placement of rigid cervical collar. Difficulty in mask ventilation was experienced in 11 (18.3%). There was no significant difference in the difficulty in insertion of laryngoscope or Airtraq [Table 2]. There were two failures to intubate in the Airtraq group, which were not related to poor view of vocal cords but to an inability to advance the tracheal tube within 120 sec despite using the manoeuvres described. Fourteen (23.3%) patients required a second attempt with laryngoscopy, whereas only 4 (6.7%) required a second attempt (P=0.01) with Airtraq. The Airtraq significantly reduced median IDS score [Table 2] and improved Cormack and Lehane glottic view [Table 3], compared to laryngoscopy. Only six patients had an IDS score of 1 or less with laryngoscopy using Mc Coy blade, compared to 52 with the Airtraq. Using Mc Coy blade, 14 patients had an IDS score of 5 or greater, indicating moderate to severe intubation difficulty, whereas none with Airtraq had an IDS >5. There was no significant difference in the duration of intubation attempts between the techniques. Fewer manoeuvres were required with Airtraq to improve the glottic exposure, compared to laryngoscopy [Table 3]. There was no difference in the incidence of complications in the two groups [Table 2]. Removal of cervical collar was not required in any of the patients with both the techniques.
Table 1.
Demographic data and airway characteristics of patients in the study
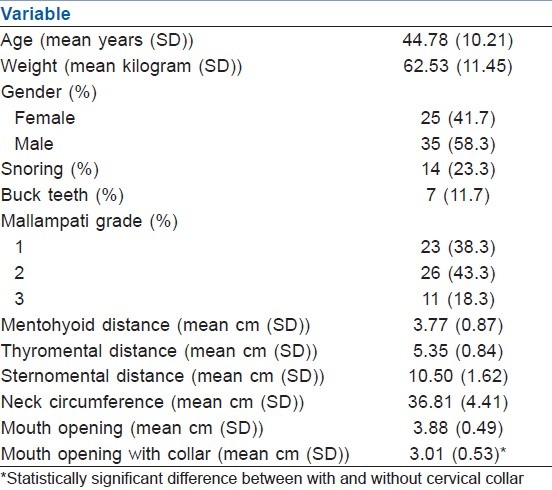
Table 2.
Comparison of intubation between laryngoscopy and Airtraq®
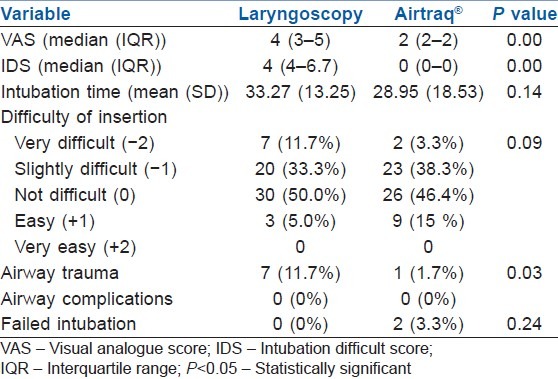
Table 3.
Comparison of intubation difficulty score between laryngoscopy and Airtraq®
DISCUSSION
Spinal cord injury has been reported in association with the airway management of patients with cervical spine instability in whom cervical spine immobilisation was not performed. Unfortunately, cervical spine immobilisation reduces the quality of glottic exposure.[11] MILS prevents head extension and neck flexion, which are necessary for optimal alignment of the three airway axes and exposure of the vocal cords using direct laryngoscopic techniques. The use of a rigid collar, tape and sandbags may result in an increased incidence of Grade 3 and 4 laryngoscopic views (up to 64%) with conventional laryngoscopy owing to the combination of decreased inter-incisor distance and cervical spine immobility.[3] Consequently, manoeuvres to stabilise the neck in patients at risk of cervical spinal injury may result in failure to secure the airway, which may result in substantial morbidity and even mortality in this patient group. These issues have prompted, in part, the development of a number of alternative approaches to securing the airway in patients at risk of cervical spine injury. Airtraq that was recently introduced into the Indian market is one of them. We evaluated the relative efficacies of this intubation technique when used by experienced anaesthesiologist in the clinical setting of cervical spine immobilisation using rigid cervical collar and MILS and compared it with the commonly used Mc Coy laryngoscope. Airtraq has an exaggerated curvature of the blade and an internal arrangement of optical components, which provide a high-quality view of the glottis without the need for alignment of the oral, pharyngeal and tracheal axes, and therefore requiring application of less force during laryngoscopy, less external neck pressure and less manoeuvres to facilitate intubation, as seen in this study. There are published reports that Airtraq intubating device is superior to laryngoscopy in patients with normal airways[12] and difficult airway scenarios simulated in manikins.[6,13] Airtraq has also been shown to produce less haemodynamic stimulation,[14] a potentially important advantage in certain clinical situations. In a study of morbidly obese patients where tracheal intubation was compared using the Airtraq and Macintosh laryngoscopes, the mean time taken for tracheal intubation was found to be shorter in the Airtraq group. There was no statistically significant difference in the duration of intubation compared to that with Mc Coy blade. However, it should be noted that the authors were more familiar with the latter technique. The presence of cervical collar could have also resulted in slightly longer intubation times with Airtraq as compared to earlier studies. Turkstra et al.[7] reported 66% lesser movement at occiput–C1, C2–C5 and C5–thoracic segments with Airtraq than that during Macintosh laryngoscopy. Studies have demonstrated that the Airtraq reduces the difficulty of tracheal intubation in patients undergoing cervical spine immobilisation with MILS when compared with the Macintosh laryngoscope.[5] Koh et al. reported higher success rate of intubation with Airtraq in patients with cervical immobilisation with collar.[15] Arslan et al. evaluated the effectiveness of the Airtraq and CTrach™ in lean patients with simulated cervical spine injury after application of a rigid cervical collar.[8] Our study confirms and extends these findings to application of cervical immobilisation as recommended in Advanced Trauma Life Support (ATLS) guidelines using rigid cervical collar along with MILS and head taped to the table. This study demonstrated that the Airtraq reduced the IDS, improved the Cormack and Lehane grade and reduced the number of optimisation manoeuvres compared with the laryngoscopy. The reduced interdental distance due to rigid cervical collar did not hamper the intubation quality with Airtraq. The authors did experience some difficulties advancing the tracheal tube towards the glottis. This was the principal reason for the increased duration of tracheal intubation in some of these patients. There were two failures to intubate in the Airtraq group, which were not related to poor view of vocal cords but to an inability to advance the tracheal tube within 120 sec despite using the manoeuvres described.[16] These patients were intubated using Mc Coy laryngoscope and bougie. However, the IDS was high. Another problem with Airtraq was fogging on the distal lens which reduced the image quality.
Difficulty in intubation despite good glottic visualisation is a problem reported with most video laryngoscopes. Most video laryngoscopes can achieve a better view of the glottis and have a similar success rate. Overall, the time to tracheal intubation was not different between the video laryngoscopes and direct laryngoscopy.[17] Different video laryngoscopes such as Glidescope Ranger, Storz C-MAC, Ambu Pentax AWS, Airtraq and McGrath Series 5 were compared with Macintosh blade for ease and time of intubation in a cervical spine immobilised manikin.[18] The time to first effective ventilation was fastest when using Macintosh laryngoscope (21.0±7.6 sec). It was 33.2±23.9 sec with Airtraq, 32.4±14.9 sec with Pentax Airway Scope, and 34.1±23.9 sec, 101.7±108.3 sec and 46.3±59.1 sec with Storz C-MAC, McGrath Series 5 and Glidescope Ranger, respectively. The investment cost is lower with Airtraq when compared to other video laryngoscopes.
There are certain limitations in this study. We acknowledge that it is impossible to blind the anaesthesiologist to the device being used, thus there is a potential bias. Furthermore, some subjectivity is involved with certain measurements used in this study, such as laryngoscopic grading. Though Cormack and Lehane classification has an advantage of being used widely in clinical practice, the appropriateness of using this classification with indirect laryngoscopes is open to question. Arsaln et al.[8] have considered only the Cormack and Lehane grading of glottis visualisation in their study using Airtraq. In addition to Cormack and Lehane glottic view classification, we have also used IDS which is more objective and found to have a good agreement between subjective indices of difficulty of intubation. Secondly, this study was carried out by experienced users of each device. The results seen may differ in the hands of less experienced users. Finally, the relative efficacy of these devices in comparison to other promising devices has not been determined.
CONCLUSION
Airtraq improves the ease of intubation when compared to laryngoscopy with Mc Coy blade in patients immobilised with cervical collar and MILS simulating cervical spine injury with the same rapidity as Mc Coy laryngoscope and can aid intubation without the need to remove the cervical collar.
Appendix 1: Modified intubation difficulty score
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Goutcher CM, Lochhead V. Reduction in mouth opening with semi-rigid cervical collars. Br J Anaesth. 2005;95:344–8. doi: 10.1093/bja/aei190. [DOI] [PubMed] [Google Scholar]
- 2.Wakeling HG, Nightingale J. The intubating laryngeal mask airway does not facilitate tracheal intubation in the presence of a neck collar in simulated trauma. Br J Anaesth. 2000;84:254–6. doi: 10.1093/oxfordjournals.bja.a013414. [DOI] [PubMed] [Google Scholar]
- 3.Heath KJ. The effect of laryngoscopy of different cervical spine immobilisation techniques. Anaesthesia. 1994;49:843–5. doi: 10.1111/j.1365-2044.1994.tb04254.x. [DOI] [PubMed] [Google Scholar]
- 4.Fuchs G, Schwarz G, Baumgartner A, Kaltenbock F, Voit-Augustin H, Planinz W. Fiberoptic intubation in 327 neurosurgical patients with lesions of the cervical spine. J Neurosurg Anesthesiol. 1999;11:11–6. doi: 10.1097/00008506-199901000-00003. [DOI] [PubMed] [Google Scholar]
- 5.Maharaj CH, Buckley E, Harte BH, Laffey JG. Endotracheal intubation in patients with cervical spine immobilization: A comparison of macintosh and airtraq laryngoscopes. Anesthesiology. 2007;107:53–9. doi: 10.1097/01.anes.0000267529.71756.f0. [DOI] [PubMed] [Google Scholar]
- 6.Maharaj CH, Higgins BD, Harte BH, Laffey JG. Evaluation of intubation using the Airtraq or Macintosh laryngoscope by anaesthetists in easy and simulated difficult laryngoscopy–a manikin study. Anaesthesia. 2006;61:469–77. doi: 10.1111/j.1365-2044.2006.04547.x. [DOI] [PubMed] [Google Scholar]
- 7.Turkstra TP, Pelz DM, Jones PM. Cervical spine motion: A fluoroscopic comparison of the AirTraq Laryngoscope versus the Macintosh laryngoscope. Anesthesiology. 2009;111:97–101. doi: 10.1097/ALN.0b013e3181a8649f. [DOI] [PubMed] [Google Scholar]
- 8.Arslan ZI, Yildiz T, Baykara ZN, Solak M, Toker K. Tracheal intubation in patients with rigid collar immobilisation of the cervical spine: A comparison of Airtraq and LMA CTrach devices. Anaesthesia. 2009;64:1332–6. doi: 10.1111/j.1365-2044.2009.06053.x. [DOI] [PubMed] [Google Scholar]
- 9.Norman G. Likert scales, levels of measurement and the “laws” of statistics. Adv Health Sci Educ Theory Pract. 2010;15:625–32. doi: 10.1007/s10459-010-9222-y. [DOI] [PubMed] [Google Scholar]
- 10.Adnet F, Borron SW, Racine SX, Clemessy JL, Fournier JL, Plaisance P, et al. The intubation difficulty scale (IDS): Proposal and evaluation of a new score characterizing the complexity of endotracheal intubation. Anesthesiology. 1997;87:1290–7. doi: 10.1097/00000542-199712000-00005. [DOI] [PubMed] [Google Scholar]
- 11.Smith CE, Pinchak AB, Sidhu TS, Radesic BP, Pinchak AC, Hagen JF. Evaluation of tracheal intubation difficulty in patients with cervical spine immobilization: Fiberoptic(WuScope) versus conventional laryngoscopy. Anesthesiology. 1999;91:1253–9. doi: 10.1097/00000542-199911000-00015. [DOI] [PubMed] [Google Scholar]
- 12.Maharaj CH, O’Croinin D, Curley G, Harte BH, Laffey JG. A comparison of tracheal intubation using the Airtraq or the Macintosh laryngoscope in routine airway management: A randomised, controlled clinical trial. Anaesthesia. 2006;61:1093–9. doi: 10.1111/j.1365-2044.2006.04819.x. [DOI] [PubMed] [Google Scholar]
- 13.Maharaj CH, Costello JF, Harte BH, Laffey JG. Evaluation of the Airtraq and Macintosh laryngoscopes in patients at increased risk for difficult tracheal intubation. Anaesthesia. 2008;63:182–8. doi: 10.1111/j.1365-2044.2007.05316.x. [DOI] [PubMed] [Google Scholar]
- 14.Schalte G, Scheid U, Rex S, Coburn M, Fiedler B, Rossaint R, et al. The use of the Airtraq(R) optical laryngoscope for routine tracheal intubation in high-risk cardio-surgical patients. BMC Res Notes. 2011;4:425. doi: 10.1186/1756-0500-4-425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Koh JC, Lee JS, Lee YW, Chang CH. Comparison of the laryngeal view during intubation using Airtraq and Macintosh laryngoscopes in patients with cervical spine immobilization and mouth opening limitation. Korean J Anesthesiol. 2010;59:314–8. doi: 10.4097/kjae.2010.59.5.314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Dhonneur G, Abdi W, Amathieu R, Ndoko S, Tual L. Optimising tracheal intubation success rate using the Airtraq laryngoscope. Anaesthesia. 2009;64:315–9. doi: 10.1111/j.1365-2044.2008.05757.x. [DOI] [PubMed] [Google Scholar]
- 17.Su YC, Chen CC, Lee YK, Lee JY, Lin KJ. Comparison of video laryngoscopes with direct laryngoscopy for tracheal intubation: A meta-analysis of randomised trials. Eur J Anaesthesiol. 2011;28:788–95. doi: 10.1097/EJA.0b013e32834a34f3. [DOI] [PubMed] [Google Scholar]
- 18.Wetsch WA, Spelten O, Hellmich M, Carlitscheck M, Padosch SA, Lier H, et al. Comparison of different video laryngoscopes for emergency intubation in a standardized airway manikin with immobilized cervical spine by experienced anaesthetists. A randomized, controlled crossover trial. Resuscitation. 2012;83:740–5. doi: 10.1016/j.resuscitation.2011.11.024. [DOI] [PubMed] [Google Scholar]