

Abstract
Background:
Visual analog scales (VAS) and numeric analog scales (NAS) are used to assess post-operative pain, but few studies indicate their usefulness in rural illiterate population in India.
Aims:
This study was designed to 1) Compare the impact of literacy on the ability to indicate pain rating on VAS and NAS in post-operative rural patients. 2) Assess the level of agreement between the pain scales.
Setting and Design:
Cross sectional, hospital based study.
Methods:
Informed consent was obtained from patients prior to undergoing surgical procedures in a teaching hospital. Post surgery, patients who were conscious and coherent, were asked to rate pain on both VAS and NAS. The pain ratings were obtained within 24 hours of surgery and within 5 minutes of each other.
Statistical Methods:
Percentages, chi square test, regression analysis.
Results:
A total of 105 patients participated in the study. 43 (41%) of the sample was illiterate. 82 (78.1%) were able to rate pain on VAS while 81 (77.1%) were able to rate pain on NAS. There was no significant association between pain ratings and type of surgery, duration of surgery and nature of anaesthesia. In multivariate analysis, age, sex and literacy had no significant association with the ability to rate pain on VAS (P value 0.652, 0.967, 0.328 respectively). Similarly, no significant association was obtained between age, sex and literacy and ability to rate pain on NAS (P value 0.713, 0.405, 0.875 respectively). Correlation coefficient between the scales was 0.693.
Conclusion:
VAS and NAS can be used interchangeably in Indian rural population as post-operative pain assessment tools irrespective of literacy status.
Keywords: Illiteracy, numerical analog scale, pain assessment, post-operative, rural, visual analog scale
INTRODUCTION
The international Association for the study of pain has defined pain as unpleasant emotional and sensory experience with actual or potential tissue damage, or described in terms of such damage[1] . Various pain measurement scales have been developed but none have been demonstrated to be easily used in all patients.[2] Daily clinical practice indicates that there is need of at least two equally reliable methods of pain assessment because some patients seem to have difficulty interpreting pain scales and some lack the ability of abstract thinking required to understand pain assessment scales.[2,3] International studies show that 7 to 11% of people are unable to complete the visual analog scale or find it confusing.[4,5] Replication of these studies is needed to evaluate the applicability of these scales in India.
According to data from the government of India, only 74% of the Indian population is literate, while 26% is illiterate. Literacy rate is even lower for females, where illiteracy affects 35% of the Indian population.[6] In effect, almost every fourth patient coming to an Indian hospital is illiterate. Literacy rates are even lower in rural areas such as the area where the present study was conducted.
Even though recommended guidelines for assessment of pain exist, there is still limited data, on the use of pain scales in patient population where illiteracy is prevalent such as in India. A pain assessment scale more appropriate in Indian illiterate population for evaluation of post operative pain will be an effective tool to help in management of post surgical pain. In view of the paucity of data in Indian rural population, we have undertaken this study to evaluate the impact of literacy on the ability to indicate pain on two rating scales.
METHODS
This cross sectional study was performed in post-operative patients admitted in tertiary care hospital in rural India. Patients undergoing surgical procedures in surgery, obstetrics and gynecology, ENT, urology or neurosurgery were included in the study. Clearance from the hospital ethics committee was obtained. Informed consent was obtained from all patients.
Study period
Data was collected during a period of 3 months from April 2011 to June 2011. A total of 140 patients underwent surgery during this period and 105 of them met the inclusion criteria and consented to participate in the study.
Inclusion criteria
All rural post-operative patients, who were conscious enough to cooperate and whose mental status was normal in the immediate post-operative period (24 hours) were enrolled into study.
Exclusion criteria
Urban patients, patients with unstable haemodynamic status and unconscious patients were excluded from the study.
Anaesthetic care
All types of adult surgical cases under different anaesthesia types (general, spinal, epidural, and blocks) who met inclusion criterion were included in the study [Table 1]. Intraoperative anaesthetic care was standardized to the type of the anaesthesia (general, spinal, blocks). Post-operative pain control protocols were standardized for all cases and all patients were provided injection paracetamol 1000mg every 8th hourly and injection tramadol 50 mg every 8th hourly.
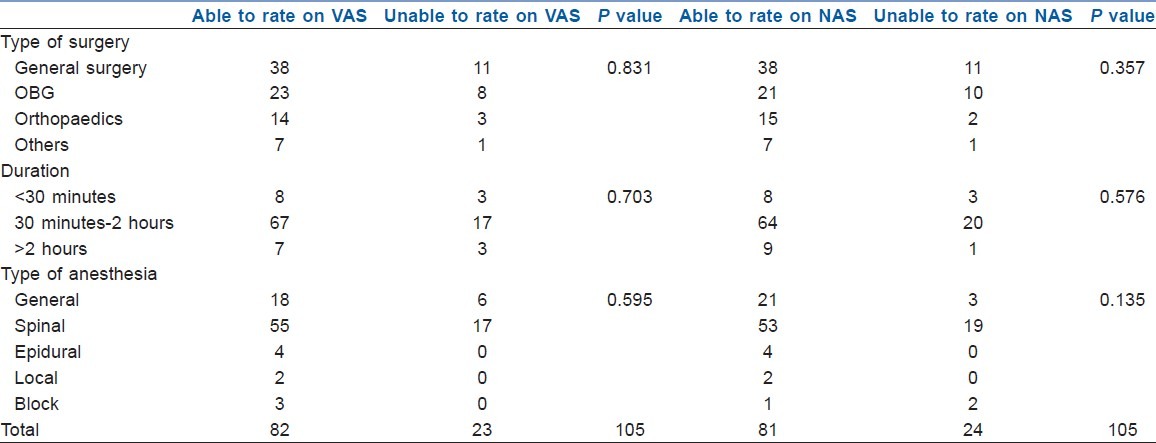
Table 1.
Surgical characteristics and ability to rate pain on VAS and NAS
Study terms
Illiterate
Patients lacking the ability both to read and write in any language were considered to be illiterate as per the census of India definition.[7]
Rural
All places which were not a municipality, corporation or cantonment or notified town area were considered to be rural areas and patients living and working in those areas were considered to be rural patients as per the census of India criteria.[7]
After enrollment, demographic and procedural characteristics were recorded by the principal investigator during a face to face interview in the pre-operative period.
Patients were briefed regarding the evaluation of pain using the VAS and NAS. To evaluate pain on the visual analog scale, patients were given a ruler marked from 0 to 10, where 0 indicated no pain and 10 indicated the worst pain ever. Patients were asked to rate their current pain intensity on this scale. For rating pain on the numeric analog scale, patients were instructed in their local language that 0 corresponded to no pain and 100 corresponded to the worst pain ever and were asked to rate the intensity of their pain using a number between 0 and 100.
Post-operatively, patients meeting the inclusion criteria were asked to rate pain on VAS and NAS. The pain rating was taken exactly 24 hours after completion of surgery. This is one time assessment and rating was taken at rest. Readings on both scales were taken immediately, one after the other with a time gap of no more than five minutes.
Data analysis was done using SPSS software (Version 19). Statistical measures obtained were percentages, proportions tests of significance (Chi square), correlation coefficient and linear regression analysis.
RESULTS
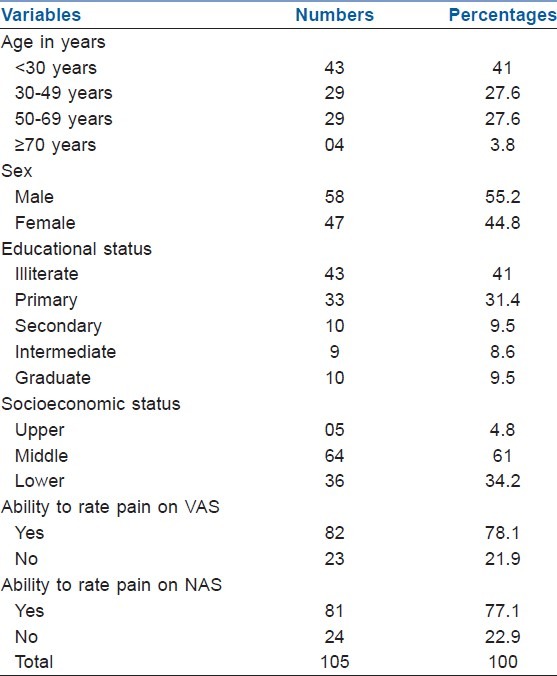
A total of 105 patients were enrolled into the study. Of 105 patients, 58 patients were male (55%) while 47 patients were female (45%). Mean patient age was 37.64±17.4 years. 43 (40%) of the respondents were illiterate. Out of 105 patients enrolled, 82 (78%) patients could rate their pain on visual analog scale; while in spite of probing 23 (22%) could not rate their pain on VAS. The same patients were asked to rate pain on the numeric analog scale within 5 minutes of the first rating. On the numeric analog scale, 81 (77.14%) patients could complete numeric analog scale while 24 (22.8%) patients could not complete numeric analog scale. This is depicted in Table 2.
Table 2.
Baseline characteristics and ability to rate pain on VAS and NAS scales
Surgical characteristics such as type of surgery, duration of surgery and type of anesthesia were cross-tabulated with the ability to rate pain on both scales and no significant association was obtained for any of the variables. The significance values are depicted in Table 1.
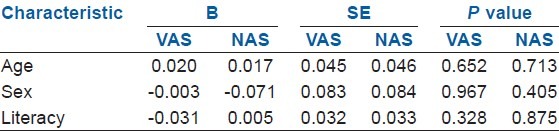
The impact of age, sex and literacy on the ability to rate pain on the NAS and VAS scales was evaluated through multivariate analysis. Ability to rate pain was coded as a binary variable, dichotomized into yes and no and binary logistic regression analysis was performed. The P values for age, sex and literacy versus VAS scale were 0.652, 0.967 and 0.328 respectively whereas the P values for age, sex and literacy versus NAS scale were 0.713, 0.405 and 0.875 respectively. The regression analysis results are depicted in Table 3.
Table 3.
Multivariate logistic regression analysis of baseline characteristics and ability to rate pain on VAS and NAS
Pearson's correlation coefficient was calculated and it revealed moderate positive correlation (0.693) between pain ratings on visual analog scale and numeric analog scale. A correlation was considered statistically significant at a level of P<0.05. A pearson correlation coefficient (r), value of >0.75 was considered to exhibit strong positive correlation, a value between 0.50 to 0.75 was considered as a moderate correlation whereas value less than 0.5 was considered to demonstrate a weak correlation between two variables. The scatter plot for comparison of pain ratings on visual analog scale and numeric analog scale is indicated in Figure 1.
Figure 1.
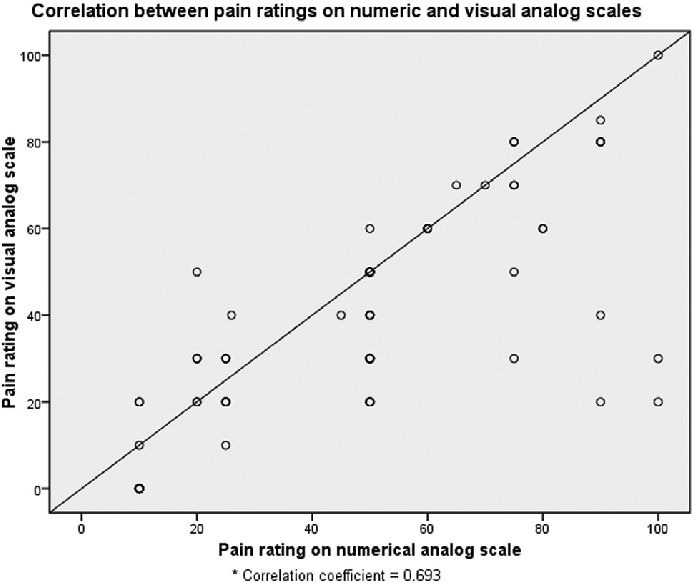
Correlation between pain ratings on numeric and visual analog scales
DISCUSSION
The effective clinical management of pain ultimately depends upon its accurate assessment. This entails a comprehensive evaluation of patient's pain and such assessments rely in part on the use of accurate evaluation tools.
Many scales have been devised to provide quantifiable measure of pain. Measures of pain are primarily classified into behavioral and subjective. Other measure includes biological and non subjective measures. The accuracy of the assessment depends upon the efforts of the health care provider and of the person experiencing pain.[8]
These measures of pain include visual analog scale, numeric analog scale and McGill pain questionnaire. Visual analog scale is the most common simple scale used in pain research.[9] It represents intensity of pain on a 10 cm plain line with two anchor points of “no pain ”and “worst pain I ever felt ”. The patient is requested to draw a line at the point that best describes his or her pain level. It is the most widely used scale for assessment of pain in clinical setting and has been reported to be sensitive and reliable.[10] Numeric analog scale is also a simple form of pain assessment where respondents are asked to rate their current level of pain on a scale between 0 to 100 where 0 represents no pain and 100 represents the worst pain ever. Studies have compared the agreement between the numerical and visual analog scale and have found good correlation between the scales.[11,12]
Visual analog scales and numeric analog scales are single dimension pain assessment tools. These tools are reasonable for use in acute pain evaluation where etiology is single and clear (in our case, the etiology is postoperative status). Visual analog scale can be administered visually and has been validated in chronic pain, rheumatoid arthritis and also in children less than 5 years of age. However, there are also some inherent problems with this scale. If the patient has cognitive dysfunction, reproducibility of the scale is questionable. Additionally, reproducibility is problematic in with dementia.[13]
The numeric analog scale can be administered either in verbal form or visual form and has been validated for use in rheumatic disease, chronic pain trauma cancer and also in illiterate patients. There are some inherent problems associated with this scale which include decreased reliability at extremes of ages, visual auditory and cognitive dysfunction.[14]
Since visual analog scale and numeric analog scales are simple to assess they can possibly be used accurately in illiterate patients. Hence, these can be particularly useful in a country like India where illiteracy is dominant (24%).[6] In the current study, there was no significant association between literacy status and the ability to rate pain on either the visual analog or numerical scales indicating the utility of these scales in the illiterate population. There was also no significant difference between other demographic characteristics such as age, sex and socioeconomic status and the ability to rate pain. Similar findings were obtained in studies by Holgate et al., Chung et al. and Fadaizadeh L.[15–17]
A moderate correlation was obtained between the pain scores on the two scales in the current study. International studies evaluating post-operative pain intensity showed good correlation among the two scales with coefficients ranging from 0.71-0.99. These differences can be explained by the differences in socio-demographic characteristic of the studied sample.[18–20] Similarly, a study conducted by Jayant et al. in India found a correlation of 0.892 between the two scales. The difference can be explained by the fact that Jayant et al. studied burn patients, while our study was conducted in post-operative patients. Post-operative patients may rate pain differently due to residual anaesthesia. In addition, our sample was predominantly rural in nature whereas the study by Jayant et al. was conducted in an urban population.[21]
The strength of the study lies in the fact that it is first of its kind, done in Indian population, that assesses the impact of literacy on pain rating by VAS and NAS. Education thus must not be hindrance in assessment and management of pain.
Limitation of the study includes the perception of pain among patients evaluated may have subjective as well as interpersonal variation which could influence the ability to rate the pain.
CONCLUSION
Visual analog scale and numeric analog scales are simple to perform tools for assessment of pain in Indian rural population, even illiterate patients can easily rate their pain on these scales, while correlation between these two scales is moderate, indicating that both scales can be used interchangeably irrespective of the literacy status of the patients.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.International Association for the Study of Pain. Pain terms: A list with definitions and notes on usage. Recommended by the IASP Subcommittee on Taxonomy. Pain. 1979;6:249. [PubMed] [Google Scholar]
- 2.Ferrell BA, Ferrell BR, Rivera L. Pain in cognitively impaired nursing home patients. J Pain Symptom Manage. 1995;10:591–8. doi: 10.1016/0885-3924(95)00121-2. [DOI] [PubMed] [Google Scholar]
- 3.Bergeron DA, Leduc G, Marchand S, Bourgault P. Descriptive study of the post-operative pain assessment and documentation process in a university hospital. Pain Res Manag. 2011;16:81–6. doi: 10.1155/2011/480479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kremer E, Atkinson JH, Ignelzi RJ. Measurement of pain. Pain. 1981;10:241–8. doi: 10.1016/0304-3959(81)90199-8. [DOI] [PubMed] [Google Scholar]
- 5.Revill SI, Robinson JO, Rosen M, Hogg MI. The reliability of a linear analogue for evaluating pain. Anaesthesia. 1976;31:1191–8. doi: 10.1111/j.1365-2044.1976.tb11971.x. [DOI] [PubMed] [Google Scholar]
- 6.New Delhi: Government of India, Ministry of home affairs, office of registrar general and census commissioner, India; 2011. [Cited 2011 Oct 3]. Census of India [Internet] Available from: http://www.censusindia.gov.in/2011-prov-results/data_files/india/Final%20PPT%202011_chapter6.pdf . [Google Scholar]
- 7.New Delhi: Government of India, Ministry of home affairs, office of registrar general and census commissioner, India; 2011. [Cited 2011 Oct 3]. Census of India - Census Terms [Internet] Available from: http://censusindia.gov.in/Data_Products/Library/Indian_perceptive_link/Census_Terms_link/censusterms.html . [Google Scholar]
- 8.Price DD, Bush FM, Long S, Harkins SW. A comparison of pain measurement characteristics of mechanical visual analogue and simple numerical rating scales. Pain. 1994;56:217–26. doi: 10.1016/0304-3959(94)90097-3. [DOI] [PubMed] [Google Scholar]
- 9.UK: Assessment of acute and chronic pain; [Cited 2011 Oct 3]. Frca.co.uk [Internet] [updated 2009 Jan 12]. Available from: www.frca.co.uk/article.aspx?articleid=100549 . [Google Scholar]
- 10.Scott J, Huskisson EC. Graphic representation of pain. Pain. 1976;2:175–84. [PubMed] [Google Scholar]
- 11.Price DD, McGrath PA, Rafii A, Buckingham B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain. 1983;17:45–56. doi: 10.1016/0304-3959(83)90126-4. [DOI] [PubMed] [Google Scholar]
- 12.Sloman R, Rosen G, Rom M, Shir Y. Nurses’ assessment of pain in surgical patients. J Adv Nurs. 2005;52:125–32. doi: 10.1111/j.1365-2648.2005.03573.x. [DOI] [PubMed] [Google Scholar]
- 13.Assessment and management of acute pain. Bloomington,MN: Institute of clinical system improvement (ICSI); 2008. [Cited 2011 Oct 3]. Icsi.org [Internet] Available from: http://www.icsi.org/pain_acute/pain_acute_assessment_and_management_of_3.html . [Google Scholar]
- 14.Gagliese L, Weizblit N, Ellis W, Chan VW. The measurement of postoperative pain: A comparison of intensity scales in younger and older surgical patients. Pain. 2005;117:412–20. doi: 10.1016/j.pain.2005.07.004. [DOI] [PubMed] [Google Scholar]
- 15.Holdgate A, Asha S, Craig J, Thompson J. Comparison of a verbal numeric rating scale with the visual analogue scale for the measurement of acute pain. Emerg Med (Fremantle) 2003;15:441–6. doi: 10.1046/j.1442-2026.2003.00499.x. [DOI] [PubMed] [Google Scholar]
- 16.Chung SM, Masaki KH, Somogyi-Zalud E, Sumida KN, Wen A, Blanchette PL. Assessment of pain in older Asian Americans with cancer. Hawaii Med J. 2009;68:62–5. [PubMed] [Google Scholar]
- 17.Fadaizadeh L, Emami H, Samii K. Comparison of visual analogue scale and faces rating scale in measuring acute post-operative pain. Arch Iran Med. 2009;12:73–5. [PubMed] [Google Scholar]
- 18.DeLoach LJ, Higgins MS, Caplan AB, Stiff JL. The visual analog scale in the immediate post-operative period: Intrasubject variability and correlation with a numeric scale. Anesth Analg. 1998;86:102–6. doi: 10.1097/00000539-199801000-00020. [DOI] [PubMed] [Google Scholar]
- 19.Li L, Liu X, Herr K. Post-operative pain intensity assessment: A comparison of four scales in Chinese adults. Pain Med. 2007;8:223–34. doi: 10.1111/j.1526-4637.2007.00296.x. [DOI] [PubMed] [Google Scholar]
- 20.Hartrick CT, Kovan JP, Shapiro S. The numeric rating scale for clinical pain measurement: A ratio measure? Pain Pract. 2003;3:310–6. doi: 10.1111/j.1530-7085.2003.03034.x. [DOI] [PubMed] [Google Scholar]
- 21.Jaywant SS, Pai AV. A comparison study of pain measurement scales in acute burn Patients. Indian J Occup Ther. 2003;35:13–17. [Google Scholar]