

Abstract
Background
Otitis media is endemic in remote Indigenous communities of Australia’s Northern Territory. Alloiococcus otitidis is an outer ear commensal and putative middle ear pathogen that has not previously been described in acute otitis media (AOM) in this population. The aims of this study were to determine the presence, antibiotic susceptibility and bacterial load of A. otitidis in nasopharyngeal and ear discharge swabs collected from Indigenous Australian children with AOM with perforation.
Methods
Paired nasopharyngeal and ear discharge swabs from 27 children with AOM with perforation were tested by A. otitidis quantitative PCR (qPCR). Positive swabs were cultured for 21 days. Total and respiratory pathogen bacterial loads in A. otitidis-positive swabs were determined by qPCR.
Results
A. otitidis was detected by qPCR in 11 ear discharge swabs from 10 of 27 (37%) children, but was not detected in paired nasopharyngeal swabs. A. otitidis was cultured from 5 of 11 qPCR-positive swabs from four children. All A. otitidis isolates had minimum inhibitory concentrations consistent with macrolide resistance. All A. otitidis qPCR-positive swabs were culture-positive for other bacteria. A. otitidis bacterial load ranged from 2.2 × 104-1.1 × 108 cells/swab (median 1.8 × 105 cells/swab). The relative abundance of A. otitidis ranged from 0.01% to 34% of the total bacterial load (median 0.7%). In 6 of 11 qPCR-positive swabs the A. otitidis relative abundance was <1% and in 5 of 11 it was between 2% and 34%. The A. otitidis bacterial load and relative abundance measures were comparable to that of Haemophilus influenzae.
Conclusions
A. otitidis can be a dominant species in the bacterial communities present in the ear discharge of Indigenous children with AOM with perforation. The absence of A. otitidis in nasopharyngeal swabs suggests the ear canal as the likely primary reservoir. The significance of A. otitidis at low relative abundance is unclear; however, at higher relative abundance it may be contributing to the associated inflammation. Further studies to better understand A. otitidis as a secondary otopathogen are warranted, particularly in populations at high-risk of progression to chronic suppurative otitis media and where macrolide therapies are being used.
Keywords: Alloiococcus otitidis, Otitis media, Acute otitis media with perforation, Indigenous Australian children, Bacterial load
Background
Otitis media is endemic in remote Indigenous communities in Australia’s Northern Territory. In this population, middle ear infection begins in the first weeks and months of life [1] and often progresses to perforation and chronic suppurative otitis media (CSOM) [2]. Cross-sectional studies have reported perforation in up to 24% of Indigenous children in the Northern Territory [3], exceeding the rate of 4% recommended by the World Health Organization as requiring urgent public health attention [4]. Standard antibiotic therapies for acute otitis media (AOM) have limited effect in this population. A randomised controlled trial (RCT) of antibiotic treatments for AOM in Indigenous children reported clinical treatment failure in 50% and 54% of children treated with single dose azithromycin or 7 days amoxycillin, respectively (RD, -4%, [95% CI, -15% to 7%]; P = 0.504) [5]. High clinical failure rates following antibiotic treatment are likely due to the dense, polymicrobial nature of otitis media in this population [6].
Alloiococcus otitidis is a slow-growing, strictly aerobic, Gram-positive coccus [7]. Culture-based detection of this species requires prolonged incubation for 5-14 days in an aerobic environment [8-10], and thus, A. otitidis will not be detected by the standard culture conditions used to identify Streptococcus pneumoniae or Haemophilus influenzae.
A. otitidis has not previously been considered in AOM affecting Indigenous Australian children; although one Australian study reported 45% Indigenous children with otitis media with effusion (OME) had A. otitidis-culture positive middle ear specimens [8]. Qualitative PCR-based studies from other populations have reported A. otitidis in MEF collected by tympanocentesis from 20-61% of children with chronic OME [11-14] and 25-50% of children with AOM [13,15-17].
Despite its detection in middle ear fluid (MEF), a primary pathogenic role for A. otitidis remains controversial. Data supporting a pathogenic role for A. otitidis include its detection in MEF from children with OME [14,16,18] and AOM [17] (in the absence of recognised otopathogens), and its capacity to provoke an inflammatory response [18-21]. One study of children with AOM reported IL-8, IL-1-β and IL-6 levels in A. otitidis-positive MEF to be similar to that of S. pneumoniae-positive specimens [22].
The reservoir of A. otitidis associated with otitis media is unclear. A. otitidis has been detected by culture or PCR in 7-12% of nasopharyngeal swabs from paediatric and adult patients with upper respiratory infection or otitis media [9,16,23]. It has also been detected by culture or PCR in 14-83% of ear canal swabs from healthy volunteers [9,24-26], suggesting A. otitidis detection in MEF may reflect specimen contamination by normal canal flora. However, both PCR and culture-based studies have reported A. otitidis in MEF collected by tympanocentesis after careful cleaning and disinfection of the canal and tympanic membrane [8,14,22,27].
Although A. otitidis antibiotic minimum inhibitory concentration (MIC) breakpoints have not been defined [28], MIC levels consistent with macrolide resistance in S. pneumoniae have been reported for 11 of 20 (55%) [8] and 11 of 12 (92%) [29]A. otitidis isolates from two studies.
Azithromycin is an emerging AOM therapy for Indigenous Australian children [5]. Whether A. otitidis is associated with AOM in this population (and the significance of any association) is currently unclear. The aims of this study were: i) to determine the prevalence of A. otitidis in nasopharyngeal and ear discharge swabs from Indigenous Australian children with AOM with perforation; ii) to determine the antibiotic susceptibility of A. otitidis isolates to penicillin and macrolides; and iii) to determine the relative abundance of A. otitidis in polymicrobial specimens.
Methods
Ethical approval
Ethical approval for this study (HREC 07/85) was provided by the Human Research Ethics Committee of the Northern Territory Department of Health and Menzies School of Health Research, which includes an Aboriginal Sub-committee.
Otitis media definitions
Otitis media definitions were as previously described [5]. AOM with perforation was defined as the presence of middle ear discharge for less than six weeks, and perforation covering less than 2% of the pars tensa of the tympanic membrane. Acute otitis media without perforation was defined as a bulging tympanic membrane and a type B tympanogram. OME was defined as an intact and non-bulging tympanic membrane and type B tympanogram.
Specimens
This study retrospectively tested paired nasopharyngeal and ear discharge swabs collected at enrolment into a randomised controlled trial (RCT) of amoxycillin or azithromycin treatment for acute otitis media, conducted between March 2003 and July 2005 [5]. Eligible children were Indigenous, living in a remote community, between 6 months and 6 years of age, and had not received antibiotics in the 7 days preceding specimen collection [5]. Children were only selected for inclusion in the A. otitidis study if parental consent was given for their future use in related studies.
The RCT enrolled 320 children and included 49 children with a diagnosis of AOM with perforation. Of these 49 children, paired baseline nasopharyngeal and ear discharge swabs from 27 Indigenous children (median age 1.2 years, range 0.5-4.0 years) with AOM with perforation were available for A. otitidis testing. Four children had bilateral perforation. Thus, the sample set included 27 nasopharyngeal and 31 ear discharge swabs (58 swabs in total). As part of the original RCT, 12 children were treated with amoxycillin (50mg/kg/day in two divided doses for a minimum of 7 days) and 15 received azithromycin (30mg/kg as a single dose). Tympanic membrane perforation had not resolved in 21 of 27 children when reviewed 6-11 days after antibiotic treatment commenced. In the six remaining children, 3 had AOM without perforation (2 azithromycin treated) and 3 had OME (2 azithromycin treated) when reviewed.
Nasopharyngeal swabs were collected as previously described [5,30]. Ear discharge swabs were collected after the ear canal was cleaned to remove any visible debris and pus. The ear discharge was then sampled under direct vision (Welch Allyn Lumiview) by positioning the swab as close to the perforation as possible. Swabs were placed in 1mL skim milk-tryptone-glucose-glycerol broth [31] and frozen immediately at -20°C before being transported to the laboratory in a liquid nitrogen dry shipper [30] for long-term at storage -70°C.
DNA extraction
Total DNA was extracted from the swabs as previously described [6] with some modification. Briefly, cellular material in a 200μL aliquot of each swab was pelleted by centrifugation. Pellets were resuspended with 200μL of enzymatic lysis buffer (containing 36.25mM phosphate buffer, 1mg/mL lysozyme (Sigma®), 0.75mg/mL mutanolysin (Sigma®), and 2mg/mL Proteinase K(QIAGEN)) then incubated at 56°C for 45 min. 10μL of 20% w/v sodium dodecyl sulfate (Amresco) was added, followed by gentle mixing at room temperature for 2 min. If the solution did not become clear, 20μL of 20mg/mL Proteinase K was added and the samples were incubated at 56°C for 10 min. 4μL of 100μg/mL RNase A (QIAGEN) was added and the samples were incubated at 70°C for 10 min. 200μL of 100% ethanol (Merck) was added and the samples were pulse vortexed for 15 s. DNA was then extracted using QIAamp DNA Mini Kit (QIAGEN) as per the manufacturer’s tissue protocol. DNA was eluted with 200μL of Buffer AE (QIAGEN).
For bacterial isolates, up to 100 colonies were harvested from purity plates and suspended in sterile water. Cells were pelleted by centrifugation and DNA was extracted as described above. The DNA concentration was determined using PicoGreen® reagent (Molecular Probes) as per the manufacturer’s instructions with fluorescence measured using a Victor3TM 1420 Multi-label counter (Perkin Elmer) and WorkOut software (Perkin Elmer; version 2.5).
General parameters for bacterial load qPCR assays
All qPCR assays were performed using Rotor-Gene 6000 real-time thermocyclers (Corbett Research). Quantitative standards were prepared by 1:10 serial dilution of reference isolate genomic DNA. qPCR raw data and standard curves were prepared using the Rotor-Gene 6000 software (Corbett Research; version 1.7). All standard curves were linear within the ranges described below. The qPCR efficiency and R2 values were calculated using the “Auto-find threshold” function with default settings. All standards and samples were tested in duplicate. Results were only accepted where duplicates differed by ≤0.5 cycles. Each assay’s limit of detection was defined as the lowest standard concentration at which specific amplification was detected in at least 95% of replicates [32].
A. otitidis qPCR
The A. otitidis qPCR used primers previously described by Hendolin et al.[33] (Table 1) which amplify a 265-bp A. otitidis-specific region of the 16S rRNA gene [GenBank: NR_026088] between positions 437-702, based on E. coli numbering. The qPCR was done using a SensiMixTMNoRef Kit (Bioline). Each 10μL qPCR included 1μM of each primer, 1X SensiMixTMNoRef reagent, 0.5X SYBR® Green I solution (Bioline), and 1μL template DNA. The reaction conditions were 95°C for 10 min followed by 35 cycles of 95°C for 15 s, 66°C for 30 s and 72°C for 15 s; then a final extension at 72°C for 1 min. This was followed by 50°C for 2 min before melt-curve analysis from 80°C-90°C in 1°C steps. Agarose gel electrophoresis was done to confirm amplification of the expected 265-bp product.
Table 1.
Primers and probes usedin qPCR assays
| Assay | Gene | Primer and Probe sequences | Position | Amplicon size (bp) | Reference |
|---|---|---|---|---|---|
| Ao |
16S rRNA |
Forward primer 5'- CTACGCATTTCACCGCTACAC -3' |
437-457 |
265 |
[33] |
| Reverse primer 5'- GGGGAAGAACACGGATAGGA -3' |
702-483 |
||||
| TBL |
16S rRNA |
Forward primer 5'- TCCTACGGGAGGCAGCAGT -3' |
331-349 |
466 |
[6,36] |
| Reverse primer 5'- GGACTACCAGGGTATCTAATCCTGTT -3' |
797-772 |
||||
| Hi |
hpd |
Forward primer 5’- GGTTAAATATGCCGATGGTGTTG -3’ |
822-844 |
151 |
[37,38] |
| Reverse primer 5’- TGCATCTTTACGCACGGTGTA -3’ |
972-953 |
||||
| Probe 5’Hex- TTGTGTACACTCCGT “T” GGTAAAAGAACTTGCAC -SpC6 -3’* |
928-896 |
||||
| Spn |
lytA |
Forward primer 5'- TCTTACGCAATCTAGCAGATGAAGC -3' |
306-326 |
101 |
[6] |
| Reverse primer 5'- GTTGTTTGGTTGGTTATTCGTGC -3' |
406-386 |
||||
| Probe 5'- [6-FAM]-TTTGCCGAAAACGCTTGATACAGGG -[TAMRA] -3' |
354-330 |
||||
| Mc | copB | Forward primer 5'- GTGAGTGCCGCTTTTACAACC -3' |
50-70 |
72 | [6] |
| Reverse primer 5'- TGTATCGCCTGCCAAGACAA -3' | 121-102 |
Ao = A. otitidis. TBL = Total bacterial load. Spn = S. pneumoniae. Hi = H. influenzae. Mc = M. catarrhalis. 16S rRNA gene position numbers are based on E. coli numbering. * Inverted commas in the primer sequence of the hpd probe indicate the position of the Black Hole Quencher.
The standard curve (100pg-100fg) was prepared using genomic DNA from the A. otitidis reference isolate ATCC51267. The limit of detection was 100fg of genomic DNA, which is equivalent to ~50 genome copies based on an A. otitidis genome size of ~1.7-Mb [34]. The A. otitidis qPCR efficiency ranged from 0.87-0.90 and all standard curves had R2 values >0.99. The no template control was negative in all except two instances in which non-specific amplification was detected below the assay’s limit of detection – quantification cycle (Cq) 32-33 which was at least 5 cycles beyond the limit of detection, at a concentration less than one cell, suggesting detection of primer-dimers.
For swabs, positive results were defined as Cq-value less than or equal to that of the 100fg standard with a dissociation temperature (as determined by melt-curve analysis) within 0.5°C of the mean dissociation temperature of the assay’s standards. Negative results were recorded for samples with i) no amplification; or ii) amplification but dissociation temperature >0.5°C different to the mean dissociation temperature of the standards, consistent with primer-dimer or other non-specific amplicons. Results were considered equivocal when i) replicates gave a positive and a negative result; or ii) Cq-values were greater than that of the 100fg control but melt profiles were consistent with A. otitidis, suggesting detection of <50 cells. Equivocal PCRs were repeated with 2μL template DNA. Samples that remained equivocal upon repeat testing were recorded as A. otitidis negative.
Other bacterial load qPCR assays
H. influenzae, S. pneumoniae, M. catarrhalis and total bacterial loads were estimated as previously described [6,35,38] with modification as described in Additional file 1. Primers and probes for all assays are shown in Table 1.
A. otitidis culture and identification
Swabs qPCR-positive for A. otitidis were thawed on ice and vortexed. 10μL was then inoculated onto horse blood agar (Oxoid), and brain-heart-infusion agar (BHI; Oxoid) supplemented with 6.5% NaCl (Crown Scientific). Horse blood agar was selected as it had previously been used to culture A. otitidis from middle ear specimens [8]. As A. otitidis is salt tolerant [7], BHI agar with 6.5% NaCl was included as a potentially selective medium, as previously proposed by Tano et al.[9].
A. otitidis reference strain ATCC51267 was used as a positive control. Plates were incubated at 37°C in an ambient atmosphere and were read after 2, 5, 7, 9, 14 and 21 days of incubation. Small, off-white colonies [8] of similar appearance to the A. otitidis reference isolate were Gram stained and subcultured on horse blood agar with incubation at 37°C for 48 hrs in an ambient atmosphere. Alpha-haemolytic, catalase-positive, oxidase-negative, Gram-positive cocci were considered presumptive A. otitidis[7]. Genomic DNA from presumptive A. otitidis colonies was extracted and identification was confirmed using the qPCR described above.
A. otitidis antibiotic susceptibility testing
Penicillin, erythromycin and azithromycin MICs were determined using E-Tests® as previously described [8]. Briefly, isolates were suspended in sterile saline to no. 3 MacFarland standard then inoculated onto horse blood agar plates. After drying, E-test® strips were applied and the plates incubated at 37°C in an ambient atmosphere for 48 hrs. These conditions are required to support sufficient A. otitidis growth to enable MIC determination [8]. As CLSI MIC breakpoints have not been determined for A. otitidis, the breakpoints of S. pneumoniae[28] were applied (consistent with previous studies [8,29]).
Culture for other bacterial species
Culture data for other bacterial species in A. otitidis qPCR-positive swabs were derived from the original RCT database. Culture had been performed as previously described [5,30] for 18-24 hrs and did not include testing for A. otitidis.
Results
qPCR detection of A. otitidis
A. otitidis was detected by qPCR in ear discharge swabs from 10 of 27 children (37%), including one child with bilateral detection (11 positive ear discharge swabs in total). In the remaining three children with bilateral perforation, two were qPCR-positive for A. otitidis in one ear only; and one was A. otitidis negative. As part of the original RCT, five of the A. otitidis-positive children were treated with azithromycin and five treated with amoxycillin. When reviewed 6-11 days after treatment, 7 of the 10 A. otitidis-positive children continued to have a diagnosis of acute otitis media with perforation (3 azithromycin treated, 4 amoxycillin treated). A. otitidis was not detected by qPCR in nasopharyngeal swabs (0/27). No further testing of nasopharyngeal swabs was performed.
Culture of A. otitidis qPCR-positive swabs
A. otitidis was isolated from 5/11 qPCR-positive ear discharge swabs from 4 children after 2-14 days’ incubation (Table 2). As A. otitidis is salt tolerant [7], BHI agar with 6.5% NaCl was used as a selective medium [9]; however, all cultures grew other bacterial species after two days’ incubation, resulting in substantial overgrowth before day 21.
Table 2.
A. otitidis isolates cultured from eardischarge swabs
| Sample |
Days of culture until
A. otitidis
was isolated |
Penicillin MIC | Erythromycin MIC | Azithromycin MIC | |
|---|---|---|---|---|---|
| HBA agar | BHI agar with 6.5%NaCl | ||||
| Child A (Left ear) |
5 |
7 |
0.19 |
4 |
1.5 |
| Child A (Right ear) |
2 |
5 |
0.125 |
3 |
2 |
| Child B |
14 |
5 |
0.006 |
>256 |
128 |
| Child C |
Not detected* |
9 |
0.19 |
>256 |
>256 |
| Child D | 7 | Not detected | 0.032 | 96 | 64 |
Culture and antibiotic susceptibility data for five isolates from four children (designated child A-D). All cultures were positive for other bacteria after two days’ incubation. MIC values are in μg/mL. In the absence of A. otitidis-specific CLSI breakpoints, the MIC values used to define pneumococcal susceptibility were applied [28]. For oral penicillin V: sensitive ≤0.06μg/mL, intermediate susceptibility 0.12-1μg/mL, resistant ≥2μg/mL. For erythromycin: sensitive ≤0.25μg/mL, intermediate susceptibility 0.5μg/mL, resistant ≥1μg/mL. For azithromycin: sensitive ≤0.5μg/mL, intermediate susceptibility 1μg/mL, resistant ≥2μg/mL. HBA = Horse blood agar. *This plate was overgrown by a Proteus sp.
Susceptibility of A. otitidis isolates
Five A. otitidis isolates were available for antibiotic susceptibility testing (Table 2). Erythromycin MICs ranged from 3 - >256μg/mL. Azithromycin MICs ranged from 1.5 - >256μg/mL. Penicillin MICs ranged from 0.006-0.19μg/mL. If S. pneumoniae Clinical Laboratory Standards Institute (CLSI) MIC breakpoints [28] are applied, as previously described [8,29], all isolates were resistant to erythromycin and 4/5 were resistant to azithromycin. Using S. pneumoniae CLSI breakpoints for oral penicillin V, 3/5 isolates had intermediate penicillin susceptibility.
Other bacteria cultured from A. otitidis-positive ear discharge swabs
Previously recorded culture data for the 11 A. otitidis qPCR-positive swabs were reviewed to determine if other species were present. All A. otitidis-qPCR positive swabs were polymicrobial with at least 2-5 other species cultured (Table 3). In one child (Child G), A. otitidis, S. pneumoniae, H. influenzae, M. catarrhalis, Staphylococcus sp. and other unidentified bacteria were all detected. Overall, Staphylococcus sp. were cultured from 10 of the 11 A. otitidis qPCR-positive swabs.
Table 3.
Other bacteria previously cultured from A. otitidis qPCR-positive ear discharge specimens
| Swab | S. pneumoniae | H. influenzae | M. catarrhalis | β-haemolytic streptococci | Staphylococcus sp. | P. aeruginosa | Proteus sp. | Other |
|---|---|---|---|---|---|---|---|---|
| Child A (Left ear) |
- |
+ |
- |
- |
- |
- |
- |
+ |
| Child A (Right ear) |
- |
+ |
- |
- |
+ |
- |
- |
- |
| Child B |
- |
- |
n/a |
- |
+ |
n/a |
+ |
+ |
| Child C |
- |
- |
n/a |
- |
+ |
- |
+ |
+ |
| Child D |
- |
- |
- |
+ |
+ |
- |
- |
+ |
| Child E |
+ |
+ |
- |
- |
+ |
- |
- |
- |
| Child F |
- |
- |
n/a |
- |
+ |
n/a |
+ |
+ |
| Child G |
+ |
+ |
+ |
- |
+ |
- |
- |
+ |
| Child H |
- |
- |
- |
- |
+ |
- |
- |
+ |
| Child I |
- |
- |
- |
- |
+ |
+ |
- |
+ |
| Child J | - | - | - | - | + | + | - | + |
These data were derived from the original RCT database. Culture data for M. catarrhalis and P. aeruginosa were not available for some swabs due to overgrowth by Proteus species (n/a = not available).
A. otitidis bacterial load and relative abundance in polymicrobial ear discharge specimens
As all A. otitidis-qPCR positive swabs were culture-positive for at least two other species, bacterial load measures were used to determine if A. otitidis was a minor or dominant constituent of the bacterial communities (Table 4). A. otitidis bacterial load in the 11 qPCR-positive swabs ranged from 2.2 × 104-1.1 × 108 cells/swab (median 1.8 × 105 cells/swab), while the total bacterial load estimates ranged from 1.5 × 107-8.1 × 108 cells/swab (median 9.4 × 107 cells/swab; Figure 1).
Table 4.
H. influenzae , S. pneumoniae , and M. catarrhalis bacterial loads in A. otitidis -positive ear discharge swabs
| A. otitidis | H. influenzae | S. pneumoniae | M. catarrhalis | |
|---|---|---|---|---|
| In A. otitidis-positive ED swabs (n = 11#) |
|
|
|
|
| qPCR-positive swabs |
11 |
10 |
3 |
4 |
| Culture-positive swabs |
5 |
4 |
2 |
1 |
| Bacterial load range (cells/swab) |
2.2 × 104-1.1 ×108 |
4.3 ×104-1.2 ×107 |
3.5 ×104-1.8 ×105 |
4.3 ×104-5.9 ×105 |
| Number of swabs with bacterial load >1x106 cells/swab |
5 |
5 |
0 |
0 |
| Number of swabs culture-positive and bacterial load >1x106 cells/swab |
4 |
3 |
0 |
0 |
| Number of swabs with relative abundance <1% |
6 |
5 |
3 |
4 |
| Relative abundance range (%) |
0.01-0.70 |
0.02-0.79 |
0.01-0.68 |
0.01-0.89 |
| Number of swabs with relative abundance >1% |
5 |
5 |
0 |
0 |
| Relative abundance range (%) | 2-34 | 4-27 | 0 | 0 |
#One child with bilateral. *A. otitidis culture was only performed for qPCR-positive swabs.
Figure 1.
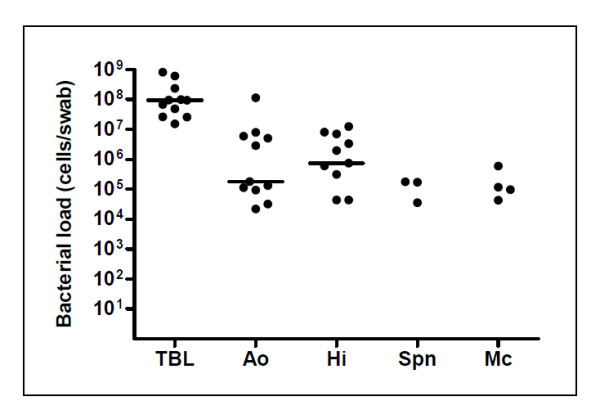
Total and species-specific bacterial loads in 11 A. otitidis -positive ear discharge swabs. Species-specific data points are only shown for qPCR-positive specimens. A. otitidis, H. influenzae and total bacterial load median values are indicated with a bar. TBL = Total bacterial load. Ao = A. otitidis. Hi = H. influenzae. Spn = S. pneumoniae. Mc = M. catarrhalis.
A. otitidis relative abundance was then determined by expressing its bacterial load as a percentage of the total bacterial load (Table 4). The relative abundance of A. otitidis ranged from 0.01-34% of the total bacterial load (median 0.7%). In 6 of 11 qPCR-positive swabs the A. otitidis relative abundance was <1% (median 0.2%). The A. otitidis bacterial load in these swabs ranged from 2.2 × 104-1.8 × 105 cells/swab and only one swab was positive by culture. In the remaining five swabs the relative abundance ranged from 2-34% of the total bacterial load (median 9%). These samples had the highest A. otitidis bacterial loads (2.9 × 106-1.1 × 108 cells/swab) and 4 of 5 were A. otitidis-positive by culture.
Bacterial load and relative abundance of A. otitidis compared to recognised otopathogens
H. influenzae, S. pneumoniae and M. catarrhalis bacterial loads were determined for the 11 A. otitidis-positive ear discharge swabs (Table 4 and Figure 1). Ten A. otitidis-positive swabs were also qPCR-positive for H. influenzae. Overall, H. influenzae and A. otitidis bacterial loads and relative abundances were similar (Table 4): the bacterial load ranged from 4.3 × 104-1.2 × 107 cells/swab for H. influenzae (median 7.4 × 105 cells/swab) and 2.2 × 104-1.1 × 108 cells/swab for A. otitidis (median 1.8 × 105 cells/swab). Maximum relative abundance was 27% for H. influenzae versus 34% for A. otitidis. The relative abundance of H. influenzae was <1% in 5/10 H. influenzae qPCR-positive swabs. In 5/10 H. influenzae qPCR-positive swabs the A. otitidis bacterial load was higher than that of H. influenzae.
S. pneumoniae and M. catarrhalis were detected by qPCR in fewer A. otitidis-positive swabs (3/11 and 4/11, respectively) and were only present at <1% relative abundance (Table 4). S. pneumoniae bacterial load ranged from 3.5 × 104-1.8 × 105 cells/swab. M. catarrhalis bacterial load ranged from 4.3 × 104-5.9 × 105 cells/swab.
Discussion
A. otitidis is present in the ear discharge of Indigenous children with AOM with perforation
In this study, A. otitidis was detected by qPCR in ear discharge swabs from 10 of 27 children (37%). This rate is consistent with PCR-based AOM studies from Finland, the USA and Japan (25%, 32% and 50%, respectively) [13,15,16], and a culture-based study of chronic OME in Indigenous and non-Indigenous Australian children (45% and 36%, respectively) [8] which tested MEF from children referred for myringotomy.
A. otitidis isolation from ear discharge swabs
Published incubation times for A. otitidis culture vary from 5-14 days [9,22]. Data from this study support culture for 14 days. It is important to note that unless extended incubation times are used, culture-based otitis media studies may not detect A. otitidis.
Using an extended culture procedure, we isolated A. otitidis from 5 of 11 qPCR-positive ear discharge swabs. Several factors may have contributed to the low A. otitidis isolation rate. Firstly, PCR-positive but culture-negative results may indicate detection of non-viable bacteria; however, it is generally accepted that DNA is quickly cleared from the middle ear [39-41] suggesting that a positive PCR is indicative of viable cells. Secondly, A. otitidis viability may have been affected by storage at -70°C for up to five years; however, viability of S. pneumoniae and H. influenzae has been demonstrated in swabs stored for up to 12 years at -70°C [42] suggesting good overall bacterial survival despite the prolonged storage.
Overgrowth by other bacterial species likely affected A. otitidis isolation. All cultures grew other species after two days’ incubation, which potentially obscured the small A. otitidis colonies. Use of BHI agar with 6.5% NaCl as a selective medium was unsuccessful due to heavy overgrowth by other species after two days’ incubation, despite the high salt concentration. Interestingly, successful A. otitidis culture was associated with higher bacterial loads (4 of 5 culture-positive swabs with bacterial load ≥1 × 106cells/swab versus 1/6 culture-positive with bacterial load <1 × 106cells/swab). The small study size limits further interpretation of this finding. Overall, our findings are consistent with the lower sensitivity of culture compared to PCR that has been documented for several bacteria in middle ear samples [43] and highlights the difficulties associated with A. otitidis culture, even when prolonged culture conditions are used.
Macrolide resistance in A. otitidis isolates
The five A. otitidis isolates had MIC values suggestive of macrolide resistance (erythromycin MICs 3 to >256μg/mL; azithromycin MICs 1.5 to >256μg/mL). If S. pneumoniae CLSI breakpoints are applied [8,29], 3 of 5 A. otitidis isolates also had intermediate level penicillin resistance. The validity of applying S. pneumoniae breakpoints to interpret A. otitidis MIC data remains to be determined, especially as atypical culture conditions are required to achieve sufficient growth [8]. Specific CLSI breakpoints are required to confirm macrolide resistance and reduced-penicillin susceptibility in A. otitidis isolates. Overall, our findings are consistent with previous studies describing macrolide resistance in A. otitidis[8,29].
Is A. otitidis contributing to middle ear pathology?
The clinical significance of A. otitidis in the ear discharge swabs is unclear. Several studies have found A. otitidis in the ear canal of healthy volunteers indicating that it is part of the normal canal flora [9,24-26]. Other studies using culture or species-specific PCRs have detected A. otitidis (in the absence of recognised pathogens) in MEF from children with otitis media collected after careful disinfection of the canal and tympanic membrane suggesting infection of the middle ear [8,27].
In this study, A. otitidis was not detected by PCR in any nasopharyngeal swabs. Previous PCR and culture-based studies from other populations have reported A. otitidis in 7-12% of nasopharyngeal swabs [9,16,23]. As our study was limited to 27 children, it is possible that A. otitidis nasopharyngeal carriage may be detected if a larger cohort were tested. However, failure to detect A. otitidis in nasopharyngeal swabs from any of the children with positive ear discharge swabs suggests it is unlikely to be a primary otopathogen in this population.
This prompts further consideration of A. otitidis in the canal flora. Staphylococcal sp. were cultured from 10 of the 11 A. otitidis qPCR-positive ear discharge swabs. This may indicate detection of canal flora; however, it was not possible to confirm this as paired canal swabs were not available. Furthermore, as the study children may have had a perforation for up to 6 weeks, secondary middle ear infection by these species cannot be excluded.
Bacterial load and relative abundance measures were used to better understand the significance of A. otitidis in the polymicrobial ear discharge swabs. A. otitidis bacterial load and relative abundance measures were similar to that of the otopathogen H. influenzae (in A. otitidis-positive swabs). For both species, relative abundance <1% was associated with bacterial load <106 cells/swab and most of these samples were qPCR-positive and culture-negative. This suggests a minor role for these species in these specimens, and may be indicative of canal flora (H. influenzae has also been reported in normal canal flora from healthy volunteers [26]). For the remaining specimens, relative abundance ranged from 2-34% and 4-27% for A. otitidis and H. influenzae, respectively. The significance of this finding is unclear as there are no data describing relative abundance thresholds, and the small size of this study limits further interpretation. However, a relative abundance of 34% is clearly suggestive of a dominant species. Furthermore, A. otitidis was present at a relative abundance greater than that of H. influenzae in 5/10 swabs positive for both species. These data suggest that, in these children, A. otitidis may have secondarily infected the middle ear following tympanic membrane perforation. This interpretation is consistent with the hypothesis previously proposed by De Baere et al.[26] who reported substantially higher rates of A. otitidis in ear canal rather than nasopharyngeal swabs (83% versus 8%) and concluded that A. otitidis in MEF from children with OME most likely reflected either secondary infection following perforation or specimen contamination by canal flora. As Indigenous Australian children are at high-risk of progressing to CSOM [44], further research is warranted to better understand A. otitidis in secondary middle ear infection, particularly where macrolide antibiotics, such as azithromycin, are used to treat AOM with perforation [5].
Study limitations
This study retrospectively considered A. otitidis in polymicrobial ear discharge swabs collected from Indigenous Australian children with AOM with perforation. The study specimens had been stored for up to five years. While it is unclear if prolonged storage may have adversely affected qPCR detection of A. otitidis, culture-based studies have reported continued bacterial viability in upper respiratory swabs after up to 12 years storage at -70°C [42].
The study focused on Indigenous Australian children who are at high-risk of progression to CSOM, and thus the findings may not be generalisable to other populations. The small study size (27 children) also limits generalisation of the findings. Despite these limitations, it appears that A. otitidis is often present in the ear discharge of young Indigenous children with AOM with perforation (37% of our cohort).
The study was also potentially limited by the ear discharge sampling technique. Ear discharge swabs in this study were all collected from children with AOM with perforation affecting <2% of the pars tensa of the tympanic membrane for up to six weeks. Paired canal swabs were not collected. Canals were cleaned prior to sampling, but disinfection was not done. As the small size of the perforations prevented middle ear sampling, it is likely that some degree of contamination from canal flora will be present in the swabs. This limitation prevents definitive differentiation of canal flora from middle ear pathogens.
The qPCR described in this study is a modification of a previously published qualitative A. otitidis PCR [33]. The qPCR had efficiency of 0.87-0.90, slightly below the ideal range of 0.9-1.10 [45]. This may reflect the amplicon size which is approximately twice that recommended for qPCR [45]. This limitation was accepted as there are few data describing alternative A. otitidis-specific PCR targets and a qPCR efficiency of 0.8-0.9 is common to other bacterial load assays [46].
Conclusions
This study used qPCR to show that A. otitidis is present in ear discharge swabs from Indigenous Australian children with AOM with perforation. In a subset of ear discharge swabs we found high A. otitidis load and relative abundance. The absence of A. otitidis in nasopharyngeal swabs suggests A. otitidis may only have a role in secondary middle ear infection following tympanic membrane perforation. Larger longitudinal studies and treatment trials should include paired ear discharge, canal and nasopharyngeal swabs to further test this hypothesis. Such studies should be PCR-based and include culture to assess antibiotic susceptibility. Bacterial load and relative abundance estimates should be considered when investigating the significance of A. otitidis in polymicrobial contexts, particularly in children with existing perforations. In light of the co-detection of Staphylococcus sp. in 10 of the 11 A. otitidis qPCR-positive specimens, future studies should also consider the potential for polymicrobial secondary middle ear infection by these and other species. Where collection of MEF by tympanocentesis is not feasible, paired ear discharge and canal swabs may be helpful in distinguishing bacteria from the outer and middle ear. Additional studies investigating a role for A. otitidis as a secondary pathogen in CSOM are also warranted in populations with a high prevalence of spontaneous tympanic membrane perforation.
Abbreviations
AOM: Acute otitis media; BHI: Brain heart infusion agar; CLSI: Clinical Laboratory Standards Institute; Cq: Quantification cycle; CSOM: Chronic suppurative otitis media; RCT: Randomised controlled trial; MEF: Middle ear fluid; MIC: Minimum inhibitory concentration; OME: Otitis media with effusion; qPCR: Quantitative PCR.
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
RLM conceived the study, coordinated laboratory testing and prepared the manuscript. MJB participated in the study design, qPCR development, data analyses and manuscript preparation. JB and PC carried out the qPCR and assisted with data analyses. PSM and AJL participated in the study design and provided critical review of the manuscript. HSV participated in the study design, co-ordination and manuscript preparation. All authors read and approved the final manuscript.
Pre-publication history
The pre-publication history for this paper can be accessed here:
Supplementary Material
Other bacterial load qPCR assays. qPCR methods used to quantify H. influenzae, S. pneumoniae, M. catarrhalis and total bacterial loads.
Contributor Information
Robyn L Marsh, Email: robyn.marsh@menzies.edu.au.
Michael J Binks, Email: michael.binks@menzies.edu.au.
Jemima Beissbarth, Email: jemima.beissbarth@menzies.edu.au.
Peter Christensen, Email: peter.christensen@menzies.edu.au.
Peter S Morris, Email: peter.morris@menzies.edu.au.
Amanda J Leach, Email: amanda.leach@menzies.edu.au.
Heidi C Smith-Vaughan, Email: heidi.smith-vaughan@menzies.edu.au.
Acknowledgements
We wish to acknowledge Kim Hare who assisted with MIC measurements and Allen Cheng for commenting on the manuscript draft. We also wish to acknowledge the families, health centres and schools from communities across the Northern Territory and South Australia that have participated in our studies. Financial support for this study was provided by the Channel 7 Children’s Research Foundation; The Trust Foundation; and the National Health and Medical Research Council (Australia).
References
- Leach AJ, Boswell JB, Asche V, Nienhuys TG, Mathews JD. Bacterial colonization of the nasopharynx predicts very early onset and persistence of otitis media in Australian aboriginal infants. Pediatr Infect Dis J. 1994;13:983–989. doi: 10.1097/00006454-199411000-00009. [DOI] [PubMed] [Google Scholar]
- Leach A, Wood Y, Gadil E, Stubbs E, Morris P. Topical ciprofloxin versus topical framycetin-gramicidin-dexamethasone in Australian aboriginal children with recently treated chronic suppurative otitis media: a randomized controlled trial. Pediatr Infect Dis J. 2008;27:692–698. doi: 10.1097/INF.0b013e31816fca9d. [DOI] [PubMed] [Google Scholar]
- Morris PS, Leach AJ, Silberberg P, Mellon G, Wilson C, Hamilton E, Beissbarth J. Otitis media in young Aboriginal children from remote communities in Northern and Central Australia: a cross-sectional survey. BMC Pediatr. 2005;5:27. doi: 10.1186/1471-2431-5-27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization and the CIBA foundation. Prevention of hearing impairment from chronic otitis media. London, UK: Report of a WHO/CIBA Foundation workshop; 1996. [Google Scholar]
- Morris PS, Gadil G, McCallum GB, Wilson CA, Smith-Vaughan HC, Torzillo P, Leach AJ. Single-dose azithromycin versus seven days of amoxycillin in the treatment of acute otitis media in Aboriginal children (AATAAC): a double blind, randomised controlled trial. Med J Aust. 2010;192:24–29. doi: 10.5694/j.1326-5377.2010.tb03396.x. [DOI] [PubMed] [Google Scholar]
- Smith-Vaughan H, Byun R, Nadkarni M, Jacques NA, Hunter N, Halpin S, Morris PS, Leach AJ. Measuring nasal bacterial load and its association with otitis media. BMC Ear Nose and Throat Disord. 2006;10:10. doi: 10.1186/1472-6815-6-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aguirre M, Collins MD. Phylogenetic analysis of Alloiococcus otitis gen. nov., sp. nov., an organism from human middle ear fluid. Int J Syst Evol Microbiol. 1992;42:79–83. doi: 10.1099/00207713-42-1-79. [DOI] [PubMed] [Google Scholar]
- Ashhurst-Smith C, Hall ST, Walker P, Stuart J, Hansbro PM, Blackwell CC. Isolation of Alloiococcus otitidis from Indigenous and non-Indigenous Australian children with chronic otitis media with effusion. FEMS Immunol Med Microbiol. 2007;51:163–170. doi: 10.1111/j.1574-695X.2007.00297.x. [DOI] [PubMed] [Google Scholar]
- Tano K, von ER, Eriksson PO, Sjostedt A. Alloiococcus otitidis-otitis media pathogen or normal bacterial flora? APMIS. 2008;116:785–790. doi: 10.1111/j.1600-0463.2008.01003.x. [DOI] [PubMed] [Google Scholar]
- Harimaya A, Takada R, Somekawa Y, Fujii N, Himi T. High frequency of Alloiococcus otitidis in the nasopharynx and in the middle ear cavity of otitis-prone children. International Journal of Pediatric Otorhinolaryngology. 2006;70:1009–1014. doi: 10.1016/j.ijporl.2005.10.012. [DOI] [PubMed] [Google Scholar]
- Hendolin PH, Karkkainen U, Himi T, Markkanen A, Ylikoski J. High incidence of Alloiococcus otitis in otitis media with effusion. Pediatr Infect Dis J. 1999;18:860–865. doi: 10.1097/00006454-199910000-00005. [DOI] [PubMed] [Google Scholar]
- Leskinen K, Hendolin P, Virolainen-Julkunen A, Ylikoski J, Jero J. The clinical role of Alloiococcus otitidis in otitis media with effusion. Int J Pediatr Otorhi. 2002;66:41–48. doi: 10.1016/S0165-5876(02)00186-6. [DOI] [PubMed] [Google Scholar]
- Harimaya A, Takada R, Hendolin PH, Fujii N, Ylikoski J, Himi T. High incidence of Alloiococcus otitidis in children with otitis media, despite treatment with antibiotics. J Clin Microbiol. 2006;44:946–949. doi: 10.1128/JCM.44.3.946-949.2006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guvenc MG, Midilli K, Inci E, Kuskucu M, Tahamiler R, Ozergil E, Ergin S, Ada M, Altas K. Lack of Chlamydophila pneumoniae and predominance of Alloiococcus otitidis in middle ear fluids of children with otitis media with effusion. Auris Nasus Larynx. 2010;37:269–273. doi: 10.1016/j.anl.2009.09.002. [DOI] [PubMed] [Google Scholar]
- Leskinen K, Hendolin P, Virolainen-Julkunen A, Ylikoski J, Jero J. Alloiococcus otitidis in acute otitis media. Int J Pediatr Otorhi. 2004;68:51–56. doi: 10.1016/j.ijporl.2003.09.005. [DOI] [PubMed] [Google Scholar]
- Kaur R, Adlowitz DG, Casey JR, Zeng M, Pichichero ME. Simultaneous assay for four bacterial species including Alloiococcus otitidis using multiplex-PCR in children with culture negative acute otitis media. Pediatr Infect Dis J. 2010;29:741–745. doi: 10.1097/INF.0b013e3181d9e639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neumark T, Ekblom M, Brudin L, Groth A, Eliasson I, Molstad S, Petersson AC, Torngren A. Spontaneously draining acute otitis media in children: An observational study of clinical findings, microbiology and clinical course. Scand J Infect Dis. 2011;43:891–898. doi: 10.3109/00365548.2011.591820. [DOI] [PubMed] [Google Scholar]
- Faden H, Dryja D. Recovery of a unique bacterial organism in human middle ear fluid and its possible role in chronic otitis media. J Clin Microbiol. 1989;27:2488–2491. doi: 10.1128/jcm.27.11.2488-2491.1989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kita H, Himi T, Fujii N, Ylikoski J. Interleukin-8 secretion of human epithelial and monocytic cell lines induced by middle ear pathogens. Microbiol Immunol. 2000;44:511–517. doi: 10.1111/j.1348-0421.2000.tb02526.x. [DOI] [PubMed] [Google Scholar]
- Himi T, Kita H, Mitsuzawa H, Harimaya A, Tarkkanen J, Hendolin P, Ylikoski J, Fujii N. Effect of Alloiococcus otitidis and three pathogens of otitis media in production of interleukin-12 by human monocyte cell line. FEMS Immunol Med Microbiol. 2000;29:101–106. doi: 10.1111/j.1574-695X.2000.tb01511.x. [DOI] [PubMed] [Google Scholar]
- Harimaya A, Takada R, Himi T, Yokota S, Fujii N. Evidence of local antibody response against Alloiococcus otitidis in the middle ear cavity of children with otitis media. FEMS Immunol Med Microbiol. 2007;49:41–45. doi: 10.1111/j.1574-695X.2006.00166.x. [DOI] [PubMed] [Google Scholar]
- Harimaya A, Fujii N, Himi T. Preliminary study of proinflammatory cytokines and chemokines in the middle ear of acute otitis media due to Alloiococcus otitidis. Int J Pediatr Otorhi. 2009;73:677–680. doi: 10.1016/j.ijporl.2008.12.033. [DOI] [PubMed] [Google Scholar]
- Takada R, Harimaya A, Yamazaki N, Himi T. Detection of Alloiococcus otitidis and three middle ear pathogens in the nasopharynx and the middle ear effusion of otitis-prone children. International Congress Series. 2003;1257:213–215. [Google Scholar]
- Stroman DW, Roland PS, Dohar J, Burt W. Microbiology of normal external auditory canal. Laryngoscope. 2001;111:2054–2059. doi: 10.1097/00005537-200111000-00035. [DOI] [PubMed] [Google Scholar]
- Frank DN, Spiegelman GB, Davis W, Wagner E, Lyons E, Pace NR. Culture-independent molecular analysis of microbial constituents of the healthy human outer ear. J Clin Microbiol. 2003;41:295–303. doi: 10.1128/JCM.41.1.295-303.2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Baere T, Vaneechoutte M, Deschaght P, Huyghe J, Dhooge I. The prevalence of middle ear pathogens in the outer ear canal and the nasopharyngeal cavity of healthy young adults. Clin Microbiol Infect. 2010;16:1031–1035. doi: 10.1111/j.1469-0691.2009.02928.x. [DOI] [PubMed] [Google Scholar]
- Khoramrooz SS, Mirsalehian A, Emaneini M, Jabalameli F, Aligholi M, Saedi B, Bazargani A, Taherikalani M, Borghaei P, Razmpa E. Frequency of Alloiococcus otitidis, Streptococcus pneumoniae, Moraxella catarrhalis and Haemophilus influenzae in children with otitis media with effusion (OME) in Iranian patients. Auris Nasus Larynx. 2012;39:369–373. doi: 10.1016/j.anl.2011.07.002. [DOI] [PubMed] [Google Scholar]
- Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing; eighteenth informational supplement, M100-S19 edn. Wayne, PA, USA: Clinical and Laboratory Standards Institute; 2009. [Google Scholar]
- Bosley GS, Whitney AM, Pruckler JM, Moss CW, Daneshvar M, Sih T, Talkington DF. Characterization of ear fluid isolates of Alloiococcus otitidis from patients with recurrent otitis media. J Clin Microbiol. 1995;33:2876–2880. doi: 10.1128/jcm.33.11.2876-2880.1995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stubbs E, Hare K, Wilson C, Morris P, Leach AJ. Streptococcus pneumoniae and noncapsular Haemophilus influenzae nasal carriage and hand contamination in children: a comparison of two populations at risk of otitis media. Pediatr Infect Dis J. 2005;24:423–428. doi: 10.1097/01.inf.0000160945.87356.ca. [DOI] [PubMed] [Google Scholar]
- Gibson L, Khoury J. Storage and survival of bacteria by ultra-freeze. Lett Appl Microbiol. 1986;3:127–129. doi: 10.1111/j.1472-765X.1986.tb01565.x. [DOI] [Google Scholar]
- Bustin SA, Benes V, Garson JA, Hellemans J, Huggett J, Kubista M, Mueller R, Nolan T, Pfaffl MW, Shipley GL, Vandesompele J, Wittwer CT. The MIQE guidelines: minimum information for publication of quantitative real-time PCR experiments. Clin Chem. 2009;55:611–622. doi: 10.1373/clinchem.2008.112797. [DOI] [PubMed] [Google Scholar]
- Hendolin PH, Markkanen A, Ylikoski J, Wahlfors JJ. Use of multiplex PCR for simultaneous detection of four bacterial species in middle ear effusions. J Clin Microbiol. 1997;35:2854–2858. doi: 10.1128/jcm.35.11.2854-2858.1997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mcmichael JC, Zagursky RJ, Fletcher LD. Alloiococcus otitidis open reading frames (orfs) encoding polypeptide antigens, immunogenic compositions and uses thereof. [20050203280] Ref Type: Patent, USA; 2005. [Google Scholar]
- Binks M, Cheng A, Smith-Vaughan H, Sloots T, Nissen M, Whiley D, McDonnell J, Leach A. Viral-bacterial co-infection in Australian Indigenous children with acute otitis media. BMC Infectious Diseases. 2011;11:161. doi: 10.1186/1471-2334-11-161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nadkarni MA, Martin FE, Jacques NA, Hunter N. Determination of bacterial load by real-time PCR using a broad-range (universal) probe and primers set. Microbiology. 2002;148:257–266. doi: 10.1099/00221287-148-1-257. [DOI] [PubMed] [Google Scholar]
- Wang X, Mair R, Hatcher C, Theodore MJ, Edmond K, Wu HM, Harcourt BH, Carvalho M, Pimenta F, Nymadawa P, Altantsetseg D, Kirsch M, Satola SW, Cohn A, Messonnier NE, Mayer LW. Detection of bacterial pathogens in Mongolia meningitis surveillance with a new real-time PCR assay to detect Haemophilus influenzae. Int J Med Microbiol. 2011;301:303–309. doi: 10.1016/j.ijmm.2010.11.004. [DOI] [PubMed] [Google Scholar]
- Binks MJ, Temple B, Kirkham LA, Wiertsema SP, Dunne EM, Richmond PC, Leach AJ, Smith-Vaughan H. Molecular surveillance of true nontypeable Haemophilus influenzae: an evaluation of PCR screening assays. PLoS ONE. 2011;7:e34083. doi: 10.1371/journal.pone.0034083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aul JJ, Anderson KW, Wadowsky RM, Doyle WJ, Kingsley LA, Post JC, Ehrlich GD. Comparative evaluation of culture and PCR for the detection and determination of persistence of bacterial strains and DNAs in the Chinchilla laniger model of otitis media. Ann Otol Rhinol Laryngol. 1998;107:508–513. doi: 10.1177/000348949810700609. [DOI] [PubMed] [Google Scholar]
- Post JC, Aul JJ, White GJ, Wadowsky RM, Zavoral T, Tabari R, Kerber B, Doyle WJ, Ehrlich GD. PCR-based detection of bacterial DNA after antimicrobial treatment is indicative of persistent, viable bacteria in the chinchilla model of otitis media. Am J Otolaryngol. 1996;17:106–111. doi: 10.1016/S0196-0709(96)90005-8. [DOI] [PubMed] [Google Scholar]
- Bakaletz LO. Chinchilla as a robust, reproducible and polymicrobial model of otitis media and its prevention. Expert Rev Vaccines. 2009;8:1063–1082. doi: 10.1586/erv.09.63. [DOI] [PubMed] [Google Scholar]
- Hare KM, Smith-Vaughan HC, Leach AJ. Viability of respiratory pathogens cultured from nasopharyngeal swabs stored for up to 12 years at −70 degrees in skim milk tryptone glucose glycerol broth. J Microbiol Meth. 2011;86:364–367. doi: 10.1016/j.mimet.2011.06.016. [DOI] [PubMed] [Google Scholar]
- Hall-Stoodley L, Hu FZ, Gieseke A, Nistico L, Nguyen D, Hayes J, Forbes M, Greenberg DP, Dice B, Burrows A, Wackym PA, Stoodley P, Post JC, Ehrlich GD, Kerschner JE. Direct detection of bacterial biofilms on the middle-ear mucosa of children with chronic otitis media. JAMA. 2006;296:202–211. doi: 10.1001/jama.296.2.202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization. Chronic suppurative otitis media. Burden of Illness and Management Options. Geneva. Switzerland: World Health Organization; 2004. [Google Scholar]
- D'haene B, Vandesompele J, Hellemans J. Accurate and objective copy number profiling using real-time quantitative PCR. Methods. 2010;50:262–270. doi: 10.1016/j.ymeth.2009.12.007. [DOI] [PubMed] [Google Scholar]
- Kais M, Spindler C, Kalin M, Ortqvist A, Giske CG. Quantitative detection of Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis in lower respiratory tract samples by real-time PCR. Diagn Micr Infec Dis. 2006;55:169–178. doi: 10.1016/j.diagmicrobio.2006.01.007. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Other bacterial load qPCR assays. qPCR methods used to quantify H. influenzae, S. pneumoniae, M. catarrhalis and total bacterial loads.