

Abstract
Calcified amorphous tumour is a rare, non-neoplastic, endocardially based, intracavitary cardiac mass. This report describes a 59-year old man in whom a mobile mass was found incidentally in the heart by routine echocardiography after he had been on haemodialysis for 3 years. Transoesophageal echocardiography revealed a high-echoic swinging tumour that originated from the annulus of the anterior commissure of the mitral valve. Surgical resection was performed to prevent embolization, and his clinical course was excellent.
Keywords: Calcified amorphous tumour, Mitral annulus calcification, End-stage renal disease, Haemodialysis
INTRODUCTION
Calcified amorphous tumour, a non-neoplastic cardiac mass composed of nodules of calcium on a background of amorphous fibrous material, was first described in 1997 [1]. Since then, few cases have been reported in the English literature. Because the size, origination and configuration of this tumour are variable, it is difficult to distinguish between this tumour and vegetation or other cardiac tumours preoperatively. Here, we describe a patient with a unique calcified amorphous tumour that wavered in the heart.
PATIENT
A 59-year old man, who had been on haemodialysis for 3 years because of diabetic nephropathy, was seen in our hospital, because routine echocardiography showed an intracardiac mobile mass. Routine echocardiography at 1 year before did not show any evidence of this mass. He was asymptomatic and his general condition was normal. Transthoracic and transoesophageal echocardiography revealed a cudgel-shaped, homogeneous, high-echoic mobile tumour (6 mm × 28 mm) with an acoustic shadow that originated from the annulus of the anterior commissure of the mitral valve near the left fibrous trigone (Fig. 1A and B). Slight mitral annulus calcification (MAC) was also recognized in the same location. The tumour originated from the ventricular aspect of mitral annulus, and therefore, it wavered widely and protruded through the aortic valve into the ascending aorta during systole. Because of this condition, he required urgent admission to our hospital.
Figure 1:

(A) Transthoracic echocardiogram. The long-axis view shows high-echoic mass (arrow) adhering to the mitral annulus of the anterior leaflet. (B) Transoesophageal echocardiogram. The short-axis view shows a cudgel-shaped, homogenous, high-echoic mass (arrow) that originated from the annulus of the anterior commissure of the mitral valve near the left fibrous trigone. Mitral annulus calcification was also recognized in the same area. LA: left atrium; LV: left ventricle; LAA: left atrial appendage.
Upon admission, his body temperature was 36.2°C, and there were no abnormal general physical characteristics except for inner shunt at the left antebrachium. Blood chemistry analysis showed renal dysfunction (blood urea nitrogen, 23.6 mmol/l; creatinine, 963.6 µmol/l), increased phosphorous (1.8 mmol/l) and intact parathyroid hormone level (23.2 pmol/l). His serum calcium concentration was 1.8 mmol/l. No remarkable inflammatory changes suggesting infective endocarditis were detected (white blood cells, 4.7 × 109/l; C-reactive protein, 0.0 nmol/l), and a blood culture was negative. Differential diagnosis of papillary fibroelastoma was made at this time. Computed tomography was performed to assess the coronary arteries, and no significant stenoses were observed. Because the tumour was large and very mobile, he underwent urgent surgical tumour resection to prevent embolization. The floating caseous white tumour (8 mm × 26 mm) was resected easily from the anterior commissure of the mitral valve (Fig. 2A). The operation was finished without mitral valve repair, and his clinical course was uneventful.
Figure 2:
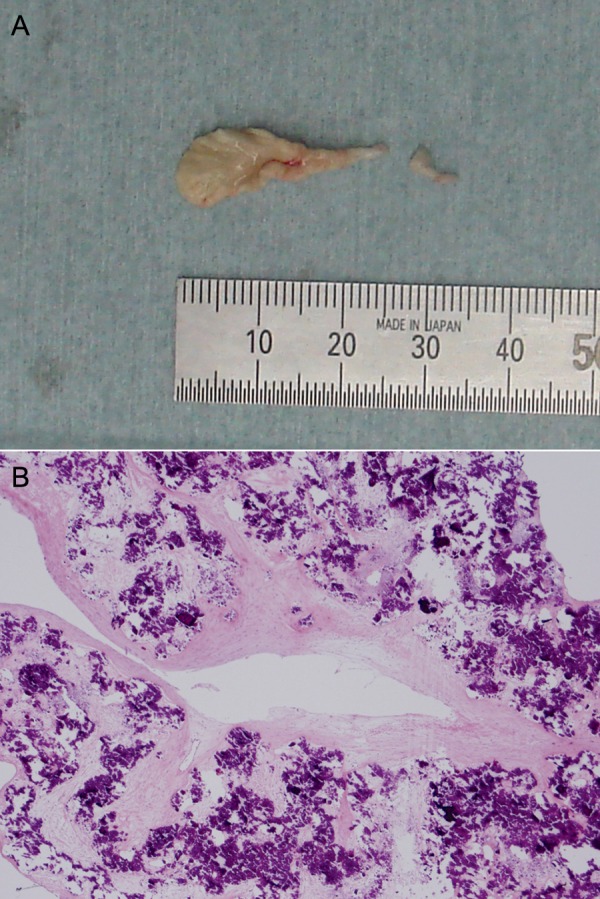
(A) Gross appearance of the resected tumour. (B) Histopathological appearance of the tumour. Fine deposits of calcium surrounded by amorphous fibrin and collagenous fibres, and chronic inflammation are seen (haematoxylin and eosin staining, ×40).
Histological examination (Fig. 2B) showed that the tumour contained multiple calcified nodules surrounded by collagenous fibres, amorphous fibrin and inflammatory cells, which confirmed the diagnosis of calcified amorphous tumour [1].
COMMENT
Calcified amorphous tumour is a non-neoplastic cardiac mass that can mimic neoplasms and cause symptoms due to the obstruction or embolization of calcified fragments. The rarity of this lesion is supported by the fact that a 29-year review at the Mayo clinic yielded only 11 such cases in 1997 [1]. From this previous report, this tumour can originate in any of the four cardiac chambers. The distribution of age and underlying disease, the tumour size and configuration are also variable. Although most of the sites of the tumour were intracavity and motionless [2, 3], MAC-related mobile calcified amorphous tumours that can mimic vegetation have been reported [4, 5]. Notably, compared with intracavity tumour, patients with MAC-related calcified amorphous tumour suffered from end-stage renal failure and received haemodialysis, including our case. Although MAC was mild in our case, the lesion was considered a MAC-related calcified amorphous tumour. Mitral annulus involvement in end-stage renal disease patients is most commonly manifested as MAC. A MAC-related calcified amorphous tumour may develop from MAC, and it may be a subtype or atypical variant of MAC [4, 5]. Therefore, this tumour located in a mitral annulus may be noted to end-stage renal disease patients. Because abnormalities of calcium–phosphorus metabolism due to renal dysfunction may contribute to rapid growth of this tumour, calcified amorphous tumour should be considered in cases of haemodialysis, particularly in cases with MAC. Moreover, the adequacy of calcium–phosphorus metabolism may be important for the prevention of MAC and MAC-related calcified amorphous tumour in haemodialysis patients.
FUNDING
Conflict of interest: none declared.
REFERENCES
- 1.Reynolds C, Tazelaar HD, Edwards WD. Calcified amorphous tumor of the heart (cardiac CAT) Hum Pathol. 1997;28:601–6. doi: 10.1016/s0046-8177(97)90083-6. [DOI] [PubMed] [Google Scholar]
- 2.Habib A, Friedman PA, Cooper LT, Suleiman L, Asirvatham SJ. Cardiac calcified amorphous tumor in a patient presenting for ventricular tachycardia ablation: intracardiac echocardiogram diagnosis and management. J Interv Card Electrophysiol. 2010;29:175–8. doi: 10.1007/s10840-009-9418-3. [DOI] [PubMed] [Google Scholar]
- 3.Ho HH, Min JK, Lin F, Wong SC, Bergman G. Calcified amorphous tumor of the heart. Circulation. 2008;117:e171–2. doi: 10.1161/CIRCULATIONAHA.107.730838. [DOI] [PubMed] [Google Scholar]
- 4.Kubota H, Fujioka Y, Yoshino H, Koji H, Yoshihara K, Tonari K, et al. Cardiac swinging calcified amorphous tumors in end-stage renal failure patients. Ann Thorac Surg. 2010;90:1692–4. doi: 10.1016/j.athoracsur.2010.04.097. [DOI] [PubMed] [Google Scholar]
- 5.Fujiwara M, Watanabe H, Iino T, Kobukai Y, Ishibashi K, Yamamoto H, et al. Two case of calcified amorphous tumor mimicking mitral valve vegetation. Circulation. 2012;125:e432–4. doi: 10.1161/CIRCULATIONAHA.111.072793. [DOI] [PubMed] [Google Scholar]