

Abstract
Greater understanding of the surgeon's task and skills are required to improve surgical technique and the effectiveness of training. Currently, neither the objective measurement of osteotomy forces during endoscopic sinus surgery (ESS) nor the validity of the properties of cadaver materials, are well documented. Measurement was performed of peak axial osteotomy force during ESS. A comparison was made of results with previously published cadaver data to validate the force properties of cadaver models. A prospective, consecutive cohort of 25 patients was compared with data from 15 cadaver heads. A modified Storz sinus curette measured osteotomy force from uncinate, bulla ethmoidalis, and ground lamella. Independent variables were osteotomy site, age, gender, indication for surgery, and side. Corresponding cadaver data were analyzed for the independent variables of osteotomy site, side, and gender and then compared with the live patient data. Mean osteotomy force in live patients was 9.6 N (95% CI, 8.9–10.4 N). Mean osteotomy force in the cadaver heads was 6.4 N (95% CI, 5.7–7.0 N). Ethmoid osteotomy of live patients required 3.2 N (95% CI, 2.1–4.3 N) more force than the cadaver heads (p = 0.0001). This relationship was statistically significant at the bulla ethmoidalis (p = 0.002) and the ground lamella (p = 0.0001) but not at the uncinate (p = 0.068). Osteotomy in female live subjects required 1.6 N (95% CI, 0.1–3.1 N) more force than male live subjects (p = 0.03). Cadaver tissue may underestimate the mean osteotomy force required in osteotomy of living ethmoid sinus lamellae by a factor of 1.5 times. Caution may be required in extrapolating force estimates from cadaver tissue to those required in living patients.
Keywords: Biomechanics, curette, endoscopic surgical procedures, ergonomics, force, measurement techniques, osteotomy, otolaryngology, paranasal sinuses, surgical therapy
The objective measurement of the forces applied to the sinus lamellae during endoscopic sinus surgery (ESS) is not routinely undertaken in current practice. During every ESS procedure, the operating surgeon repeatedly makes subjective judgements, regarding the appropriate amount of force to use, when breaching sinus lamellae. The criteria on which these decisions are made are not well documented. This has led to attempts to objectively quantify the forces required to fracture paranasal sinus lamella.1–3
A previous study from this center documented the forces required to undertake sinus lamellae osteotomies in 15 cadaver skulls.4 However, the validity of extrapolating cadaver-based data to living tissue has not been previously established.
The current study was designed to be the first to measure the actual forces required to fracture the lamellae of the anterior ethmoid sinus complex during elective surgery on living patients. This data could, in turn, then be used to validate the extrapolation of the previously gathered cadaver-based data to living tissue.
MATERIALS AND METHODS
Subjects
Live Patients.
A prospective, consecutive cohort of 25 patients undergoing ESS, were recruited into the study. Exclusion criteria were age <16 years and history of any previous sinus surgery. Each patient underwent an ESS procedure appropriate to the extent of the clinical disease present.
Cadaver Material.
Fifteen cadaver heads were used in the previous study.4 All of the cadavers had been deceased for <1 year and were preserved in Formalin.
Measures
Live Patients.
During the ESS procedure, the peak axial forces required to undertake puncture osteotomies through the lamellae of the anterior ethmoid sinus complex were recorded. Three discrete areas of the anterior ethmoid complex were categorized for force measurement: uncinate, bulla ethmoidalis, and ground lamella. These measurements were taken independently by three operating surgeons (one consultant and two registrars). Patients' age, gender, indication for surgery, osteotomy site, and side of procedure were recorded.
Cadaver Material.
Cadaver age at death, gender, side of procedure, and osteotomy site were recorded.
Equipment
The puncture osteotomy force recorded from the live patients was measured using a modified sinus curette (model no. 628702; Karl Storz, Tuttlingen, Germany), as shown in Fig. 1.
Figure 1.

Modified Storz sinus curette (below) with standard Storz sinus curette (above) for comparison.
The curette design was altered to contain a load cell (model F380-Z; Novatech, East Sussex, U.K.) at the interface between the main shaft and the handle of the curette. The modification to the curette increased length from 191 to 214 mm (12%) and overall mass from 20.9 to 43.7 g (109%). The shaft and head of the curette were fitted to the handle via a screw thread and tightened in position with a custom made spanner. During surgery the handle of the curette and wiring were encased in a disposable plastic cover of the same design routinely used to protect the endoscopic camera. The curette shaft and head were detached from the handle after each procedure and sent for sterilization.
The previous cadaver-based study4 used a modified set of Blakesley forceps to measure axial forces. A detailed description of the design of the modified Blakesley forceps and the method of data collection have been published.2–4 The modified Blakesley forceps incorporated strain gauges for load sensing into the handle. These were found to become unreliable after repeated sterilization. The new curette design avoided the sensitive load cells having to undergo the sterilization process.
The load cell in the modified curette was sensitive to force in the direction of the long axis of the instrument only (axial force). Its output was measured and recorded on a Microsoft Windows XP Professional–based Hewlett Packard Workstation, programmed in LabView (National Instruments, Austin, TX). The load cell was calibrated by applying compressive loads, representing the direction of loading in use, from 50 mN to 30 N. The calibration graph relating force to output voltage was incorporated into the software used in the measurement system.
The computer simultaneously recorded data as a file in a Microsoft Excel (Microsoft Corp., Redmond, WA) spreadsheet and presented a graph of force (newtons) versus time (seconds) in real time on the computer's monitor, superimposed on a live feed from the endoscope, which was also recorded. The computer monitor displaying the graphic “force versus time” output was placed adjacent to the stack monitor, as shown in Fig. 2, such that it did not interfere with the primary view of the operating surgeon.
Figure 2.

Graphic output of force versus time displayed on parallel computer monitor in real time. Also shown on the second monitor are two alternative prototype displays representing the applied force.
Data from all of the live patients were stored on the computer and backup hard disk. Once data collection had been completed, all data sources (intraoperative endoscopic video, tabulated force measurements, and graphical output) were simultaneously reviewed to identify the peak force used during each osteotomy.
Statistical Analysis
Live Patients.
The independent variables of osteotomy site, age, gender, side, and operative indication (polyp disease versus nonpolyp disease) were assessed using an independent ANOVA (SAS 9.1; SAS Institute, Inc., Cary, NC).
Cadaver Material.
The data from the previous study were reanalyzed with an independent ANOVA for the independent variables of side, anatomic site, and gender (SAS 9.1).
Comparison of data from the current study with corresponding data from the previous cadaver study for each of the anatomic sites was undertaken using independent t-tests (SAS 9.1).
Ethical Considerations
Full ethical approval for the study was granted by the National Health Service Tayside Ethics Committee and written consent was obtained from the patients, before enrollment into the study.
RESULTS
Live Patient Data
Twenty-five patients completed the study. Male/female ratio was 13:12. Mean age was 48.8 years (range, 25–77 years). The indications for surgery are detailed in Table 1.
Table 1.
Indication for FESS in the patients enrolled into the study
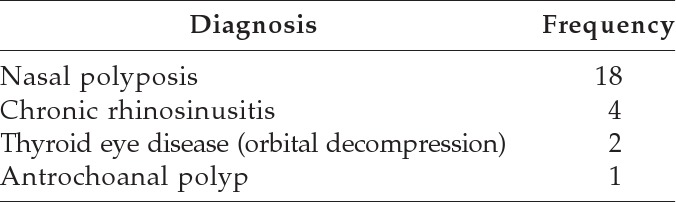
FESS = functional endoscopic sinus surgery.
Twenty-two patients underwent a bilateral procedure. Three patients underwent a unilateral procedure. The indications in the unilateral procedures were nasal polyposis, chronic rhinosinusitis, and antrochoanal polyp.
The osteotomy and debridement of the individual sinus bony lamella in each live patient was dictated by clinical need. As a result, a full data set was not recorded for all of the three anatomic sites in each patient. The mean peak axial force and the total number of data points recorded for each of the three anterior ethmoid sites are shown in Table 2.
Table 2.
Mean peak axial osteotomy forces in the live patient group
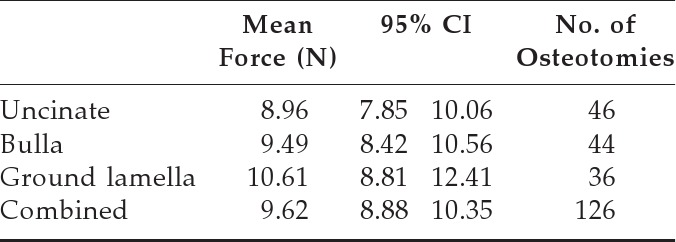
There was a statistically significant difference between the two gender groups in the live patients (p = 0.03). Osteotomy in female subjects required 1.6 N (95% CI, 0.1–3.1) more force than those in male subjects.
Analysis of the data from the live patients for the independent variables of osteotomy site, age, operative side, and preoperative indication showed no statistically significant differences.
There was a nonsignificant trend to increasing mean force requirement from the anterior to the posterior ethmoid sites.
Cadaver Data4
Fifteen cadaver heads were used in the study. Male/female ratio was 10:5. Mean age at death was 82 years (range, 48–94 years). Because of previously undertaken anatomic dissections, it was not possible to sample all of the anterior ethmoid areas in every cadaver head. The mean peak axial forces required and the total number of osteotomies recorded for each of the three anterior ethmoid sites are shown in Table 3.
Table 3.
Mean peak axial osteotomy forces in the cadaver tissue
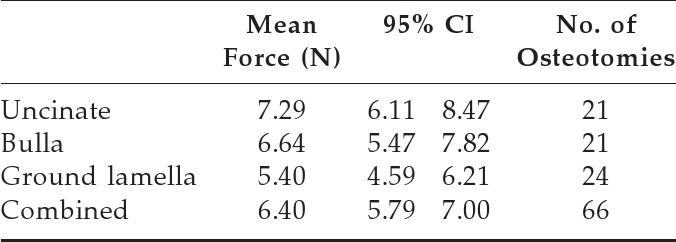
A greater mean force of 1.9 N (95% CI, 0.2–3.5 N) was required to produce an osteotomy in the uncinate than the ground lamella (p = 0.025). In contrast to the live patient data, there was a trend to a decreasing force requirement from the anterior to the posterior ethmoid sites. There were no significant differences between the independent variables of side or gender. The mean force required was greater in female than male subjects (mean difference, 0.8 N; 95% CI, −0.2–1.9 N) but the difference was not significant (p = 0.12).
Comparison of Live Patient and Cadaver Data
The results of the comparison of the live patient with cadaver data are shown in Table 4.
Table 4.
Comparison of live patient and cadaver data

At each of the anatomic sites, greater force was required to perform osteotomies in live patients than in cadaver tissue. This difference was statistically significant at the bulla ethmoidalis (p = 0.002) and the ground lamella (p = 0.0001) but not at the uncinate (p = 0.068). Combining the data for all sites, a greater mean force of 3.2 N (95% CI, 2.1–4.3 N) was required to perform an osteotomy in the anterior ethmoid complex of the live patient group than in the cadaver group (p = 0.0001). As a ratio, the force required to perform an osteotomy in live patient tissue is 1.5 greater than in cadaver tissue.
DISCUSSION
This study provides the first data set of the forces required to fracture the ethmoid sinus lamellae in live patients, using modified, routinely used, ESS instruments.
The mean peak axial forces required to undertake punch osteotomy were greater in live patients than in cadaver specimens and this difference was statistically significant in the combined data as well as for the individual sites of the bulla ethmoidalis and ground lamella. Data for the uncinate also showed a trend for greater force requirement in live patients but the difference was not statistically significant. The results suggest that the cadaver model tends to underestimate the strength of live tissue.
Wagner3 published cadaver osteotomy force data from the anterior ethmoid complex. The study design used an endoscope to apply and measure mean osteotomy forces. The study results estimated mean osteotomy forces for the bulla ethmoidalis of 8.1 N. These forces are greater than those found in our previous cadaver study,4 (6.64 N) but they were less that those recorded in the current live patient study (9.49 N) and would support the view that live tissue requires greater osteotomy force than cadaver tissue. The cause of the weaker bone found in the cadaver material is not clear. It could be the result of the fixation process or might reflect the greater age at death of the cadaver material compared with the live patient group.
The previous cadaver study was able to assess safety critical areas of the skull base. This showed that the force required to breach the skull base, optic crest, and internal carotid artery ranged from 13.1 to 17.8 N.4 It is not clear if the increased relative strength recorded in the live patient data in the current study can be extrapolated to these safety critical areas, but does suggest that these safety critical areas still require greater force to fracture than that required in ethmoid osteotomy.
Osteotomy forces were higher in female live patients than the corresponding male data. In contrast, previous radiological studies have shown higher paranasal sinus bone density in male plastinated cadaver material compared with female plastinated cadaver material.5
Ethmoid lamellae are not load bearing and therefore are unlikely to show the typically increased bone mass found in the load-bearing skeleton of male patients compared with female patients. However, the ethmoid bone would be exposed to the hormonal environment, which predisposes to reduced bone density in female subjects. It would therefore have been expected that the strength of the ethmoid lamellae would be greater in male patients than in female patients.
The difference between male and female subjects although significant is small, representing a 16% increase in overall force. The perception of differences in force application by surgeons is currently being assessed, to determine the clinical relevance of the differences in forces recorded in the study.
Limitations of the Study
Different force measurement equipment was used in each of the studies. However, each of the measurement tools was objectively calibrated and the force being measured was a noncomplex, axial measurement. Any difference between the two devices should therefore be negligible.
The exact position on the surface of each of the sinus lamellae that the curette was placed and the subsequent position that the osteotomy force measurements were taken was dictated by the judgment of the operating surgeon. Although the surgeons attempted to identify the most perpendicular position to the lamina, the variability of sinus anatomy and the possibility for bias due to subjective surgical judgment is recognized.
The current study and the previous cadaver study represent the largest published series, but the numbers in both studies are small. The small data set makes it impossible to draw any meaningful conclusions regarding the effect of underlying diagnosis and indication for surgery on the strength of the sinus lamina. A reduction in bone density with extended systemic steroid use in the treatment of nasal polyposis and the osteopenia resulting from the disease itself is well recognized. It might be expected that patients suffering from nasal polyposis and subsequently treated with nasal steroids may form a discrete group with significantly weaker sinus lamellae. This was not identified in the study results but might become apparent in a larger study.
Previous studies have also identified that chronic rhinosinusitis may result in osteitis and subsequent thickening of the sinus lamella.6 An increased bone thickness could result in a requirement for greater force during osteotomy and the live patient group may have therefore been predisposed to thicker sinus lamella. Review of the preoperative CT scans for all live patients, however, showed no evidence of bone thickening and all sinus lamella, which underwent osteotomy, were <3 mm thick.
All cadaver specimens used in the study were preserved with formalin. It may be that the use of fresh frozen cadavers would provide data closer to that found in living patients.
Clinical Applicability
Documentation of the basic properties of the paranasal sinuses will allow more prescriptive guidance in surgical training by objectively describing the force required to undertake ESS. This will lead to improvements in training effectiveness and subsequent surgical performance. The results from this study already highlight that surgeons currently training with formalin-preserved cadaver heads should note the potential differences in osteotomy forces required, compared with those that might be expected in live patient surgery.
The current study only reports on the basic data collected by the force measurement system. The measurement system is currently being developed to provide an effective, real-time, force feedback that can be used routinely in theater, to provide a training tool and augment patient safety.
Data on the expected strength of the sinus lamina could also be combined with the output of imaging techniques, such as high-resolution CT. It may soon be possible to be able to provide an accurate estimate of the strength of specific sinus anatomy based on radiological estimates of density alone. This is an area also currently under investigation.
As robotic technology matures, the automation of endoscopic sinus procedures1,7 and other otorhinolaryngological surgical procedures8 can already be envisioned. To design a control system for a robotic application to undertake sinus surgery, our knowledge of the anatomy and material properties of the paranasal sinus system has to be formalized. Central to this will be knowledge of the magnitude of the forces that can be safely exerted within the paranasal sinuses. Only by creating a set of rules describing the physical actions that can be performed, and the anatomic locations that they can be safely undertaken in, will it be possible to develop an automated sinus surgery system. Data from this study provide a starting point for the formal understanding of force generation in ESS and, consequently, could be used to inform the creation of computer programming rules.
CONCLUSIONS
A mean force of 9.62 N is required to fracture the ethmoid sinus lamellae in living patients. This value does not vary significantly across the anterior ethmoid complex. When compared with forces documented from a previous cadaver study,4 osteotomy in live ethmoid tissue requires a mean force 1.5 times greater than that required for formalin-fixed cadaver tissue. Ethmoid lamellae in live female subjects require significantly more force to fracture than male subjects. Additional work is required to conclude on the underlying causes and specific effects of gender, disease, and cadaver fixation methods on ethmoid lamellae strength.
ACKNOWLEDGMENTS
The authors thank Ben Pattinson of Karl Storz Endoscopy (United Kingdom), Ltd., for the provision of the sinus curettes. The authors also thank the Epidemiology Research Unit, Scottish Agricultural College, Inverness, for support with statistical analyses.
Footnotes
Presented previously at the summer meeting of the Scottish Otolaryngology Society, Pitlochry, Perthshire, United Kingdom, May 7–8, 2009, and the Australian Society of Otolaryngology Head and Neck Surgery Sydney, NSW, Australia, March 27–31, 2010
Funded by The Anonymous Trust, University of Dundee
The authors have no conflicts of interest to declare pertaining to this article
REFERENCES
- 1. Waridel F, Monnier P, Agrifoglio A. Evaluation of the bone resistance of the sphenoid and ethmoid sinuses. Laryngoscope 107:1667–1670, 1997 [DOI] [PubMed] [Google Scholar]
- 2. White P, Nassif RG, Saleh H, Drew T. Pilot study of a device for measuring Instrument forces during endoscopic sinus surgery. Acta Otolaryngol 124:176–178, 2004 [DOI] [PubMed] [Google Scholar]
- 3. Wagner I, Tingelhoff K, Westphal R, et al. Ex-vivo evaluation of force data and tissue elasticity for robot-assisted FESS. Eur Arch Otorhinol (DOI: 10.1007/s00405-008-0644-6, 2008.) [DOI] [PubMed] [Google Scholar]
- 4. Ross P, Joice P, Nassif R, White PS. Surgical instrument force measurement in endoscopic sinus surgery: What is the difference between parts of the ethmoid sinus complex? Am J Rhinol Allergy 24:76–80, 2010 [DOI] [PubMed] [Google Scholar]
- 5. Sprinzl GM, Menzler A, Eckel HE, et al. Bone density measurements of the paranasal sinuses on plastinated whole organ sections: Anatomic data to prevent complications in endoscopic sinus surgery. Laryngoscope 109:400–406, 1999 [DOI] [PubMed] [Google Scholar]
- 6. Lee JT, Kennedy DW, Palmer JN, et al. The incidence of concurrent osteitis in patients with chronic rhinosinusitis: A clinicopathological study. Am J Rhinol 20:278–282, 2006 [DOI] [PubMed] [Google Scholar]
- 7. Wurm J, Steinhart H, Bumm K, et al. A novel robot system for fully automated paranasal sinus surgery. International Congress Series 1256:633–638, 2003. (DOI: 10.1016/s0531(03)00284-X.) [Google Scholar]
- 8. Coulson CJ, Taylor RP, Reid AP, et al. An autonomous surgical robot for drilling a cochleostomy: Preliminary porcine trial. Clin Otolaryngol 33:343–347, 2008 [DOI] [PubMed] [Google Scholar]