

Abstract
Background:
It is common clinical practice to assess muscle strength during examination of patients following shoulder injury or surgery. Strength comparisons are often made between the patient’s injured and uninjured shoulders, with the uninjured side used as a reference without regard to upper extremity dominance. Despite the importance of strength measurements, little is known about expected normal baselines of the uninjured shoulder. The purpose of this study was to report normative values for isometric shoulder strength for physically active college-age men and women without history of shoulder injury.
Methods:
University students—546 males (18.8 ± 1.0 years, 75.3 ± 12.2 kg) and 73 females (18.7 ± 0.9 years, 62.6 ± 7.0 kg)—underwent thorough shoulder evaluations by an orthopaedic surgeon and completed bilateral isometric strength measurements with a handheld dynamometer. Variables measured included internal rotation, external rotation, abduction, supine internal rotation and external rotation at 45°, and lower trapezius in prone flexion.
Results:
Significant differences were found between the dominant and nondominant shoulder for internal rotation, internal rotation at 45°, abduction, and prone flexion in males and in internal rotation at 45° and prone flexion for females (P ≤ 0.01).
Keywords: isometric, shoulder, strength, normative data
Strength assessment of the glenohumeral and scapulothoracic muscles is an essential component of the shoulder examination. The rotator cuff muscles function primarily to stabilize and center the head of the humerus on the glenoid during upper extremity movements.30 The lower trapezius serves an equally important role, contributing to shoulder function primarily in scapular upward rotation, external rotation, and posterior tilt.22 When weakness is detected, strengthening exercises serve as a primary component of rehabilitation. Throughout the recovery process, strength assessments are repeated to evaluate progress, to adjust resistance for rehabilitation exercises, and to determine readiness to return to activity or sport. Despite the importance of postinjury strength assessment, little is known about expected baseline isometric strength in the uninjured shoulder in college athletes.
It is generally accepted that optimal shoulder function requires “normal” shoulder strength. A strain or tear of the rotator cuff muscles often leads to abnormal function because of inadequate secondary dynamic stabilization of the glenohumeral joint. Even in the absence of injury, rotator cuff muscle weakness may predict shoulder injury and may contribute to shoulder instability.5,17,31 Because muscle strength is a potential modifiable risk factor for shoulder injury, it is important to implement effective and proper techniques for strengthening the glenohumeral and scapulothoracic musculature. If the goal, however, is to reach “normal” shoulder strength, knowledge of muscle strength normative values may be useful.
While the most commonly performed clinical assessment of strength is the gross manual muscle test, this method lacks objectivity and presents reliability concerns.3,8,26 In contrast, because isokinetic testing provides easily interpreted objective data, it is often recognized as the gold standard for strength testing. Unfortunately, this method is costly and time-consuming, and the equipment is not readily available for many clinicians. Additionally, patients with pathology or those who are postoperative may not be able to tolerate isokinetic testing.21 Isometric strength testing with a handheld dynamometer is a relatively inexpensive and efficient way for clinicians to assess strength, and these devices have been shown to produce reliable objective data.12,15,23,25 The concurrent validity of handheld dynamometry and isokinetic dynamometry has been reported in several studies.7,14,28
Age-related changes in normal isometric shoulder strength indicate that meaningful differences likely exist between subjects in their second decade and those in their third and fourth decades.9 Riemann and colleagues reported normative data for shoulder internal and external rotator musculature on subjects 20 to 40 years old; however, they did not report a comparison between those in their twenties versus those in their thirties.23 Furthermore, their sample was not specifically athletic college students, as it included faculty members as well as other community members.23 Turner and colleagues also reported normative data on subjects 13 to 60 years old, stratified by activity level rather than age.29
When normative strength values are reported for a “healthy” population, it is important to first verify that the population is healthy. Previous research has demonstrated a high prevalence of rotator cuff pathology in asymptomatic individuals, which increases with age.12 A physical examination could identify asymptomatic subjects with shoulder pathology. Previous studies of normative shoulder strength have measured individuals who were asymptomatic solely on the basis of patient-reported screening questionnaires or medical record review and/or interview.9,12,23,29 Turner et al did not report any form of physical evaluation; some subjects in their study were in age ranges that could have asymptomatic rotator cuff pathology.12,29
Baseline strength comparisons between injured and uninjured shoulders are commonly performed following injury under the assumption that the uninjured limb is an appropriate reference regardless of hand dominance. Furthermore, it is common to encounter patients with bilateral shoulder symptoms, which inhibit side-to-side strength comparisons.9 The purpose of this study was to describe isometric shoulder strength values for healthy, physically active university students (17-21 years of age) without a history of shoulder injury. A secondary objective was to evaluate differences in strength measures by arm dominance and sex.
Methods
Design and Setting
Subjects were freshman between the ages of 17 and 21 years entering a 4-year collegiate-level military academy in June 2006. As part of the baseline assessment within this cohort, all subjects completed bilateral strength testing for the muscles of the shoulder and rotator cuff. The Institutional Review Board at Keller Army Community Hospital reviewed and approved this study prior to initiation.
Participants
The majority of students at the United States Military Academy are highly active and participate in athletics and physical activities to a greater extent than their counterparts at civilian universities.16 Exclusion criteria for this study included current shoulder symptoms (pain, weakness, instability), history of shoulder surgery, shoulder instability or trauma, neurological disease, and current cervical or thoracic spine pain or injury.
Of the 1311 potential subjects solicited to participate in the study, 714 provided informed consent and completed all baseline assessments (Figure 1). Of those, 619 met all inclusion/exclusion criteria and were verified as having “normal” shoulders based on physical examination by an orthopaedic surgeon. As a result, the final study population consisted of 546 males (18.8 ± 1.0 years, 75.3 ± 12.2 kg) and 73 females (18.7 ± 0.9 years, 62.6 ± 7.0 kg), which is reflective of the sex distribution of the United States Military Academy at matriculation (85% male, 15% female).
Figure 1.
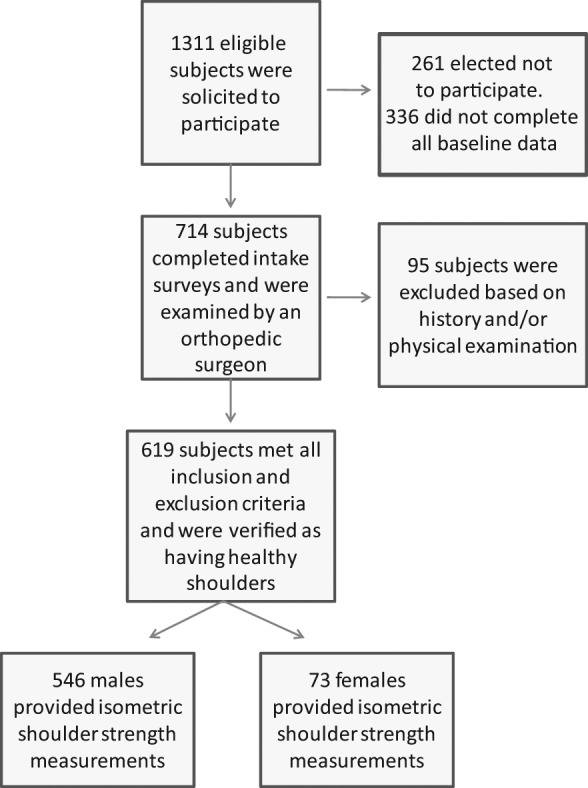
Flow diagram showing subjects available for analysis.
Procedures
Baseline questionnaires established demographics: injury and physical activity. All subjects underwent a standardized shoulder evaluation by an orthopaedic surgeon, including active range of motion, joint stability, and shoulder impingement.19
Handheld Dynamometer Isometric Strength Testing
Bilateral isometric strength was assessed using a handheld dynamometer (model 01163, Lafayette Instrument Company, Lafayette, Indiana).10,12,32 Intraclass correlation coefficients were calculated along with inter- and intrarater reliability for all 3 researchers (Table 1).1
Table 1.
Intrarater and interrater reliability.
| Position | Rater 1a | Rater 2a | Rater 3a | Interraterb |
|---|---|---|---|---|
| External rotation | 0.725 | 0.631 | 0.808 | 0.792 |
| Internal rotation | 0.896 | 0.862 | 0.935 | 0.897 |
| Abduction | 0.905 | 0.887 | 0.662 | 0.827 |
| External rotation, 45° | 0.894 | 0.924 | 0.776 | 0.850 |
| Internal rotation, 45° | 0.985 | 0.969 | 0.957 | 0.905 |
| Prone lower trapezius | 0.948 | 0.885 | 0.860 | 0.829 |
n = 12.
Intraclass correlation coefficient.
The strength measures included internal and external rotation and abduction in the neutral position, supine internal rotation and external rotation at 45° abduction, and flexion in the prone position. The dynamometer was placed just proximal to the elbow for the abduction measurement and just proximal to the styloid process of the wrist joint for all other measurements. Subjects were asked to produce a 5-second maximal contraction rather than a “break test.”23,29 Two trials were completed for each side in each position; the greatest force produced was used as a measure of muscular strength.4
Internal rotation at 45° and external rotation at 45° were measured with subjects in the supine and seated position with the shoulder abducted to 45° with 0° of flexion/extension. A bolster was used to maintain neutral flexion/extension. The supine internal rotation at 45° and external rotation at 45° positions have been described as optimal positions associated with reduced coefficient of variation and were selected to stabilize the scapulothoracic joint with the shoulder abducted to the scapular plane.6,11
Prone flexion measurements were obtained for the lower trapezius with the arm extended overhead (full flexion up to 180) and abducted 135° with the elbow fully extended and thumb directed upward.11,13,20
Statistical Analysis
Strength means and standard deviations were normalized by body mass (strength/body mass) and analyzed by sex and hand dominance. Paired t tests were performed to identify significant differences between dominant and nondominant sides. Independent t tests were performed to identify differences between sex. Gender-based percentile cut points were calculated for all strength measures. All statistical analyses were performed using SPSS 11.5.
Results
All strength measures were normally distributed (Table 2). The dominant shoulder was significantly stronger than the nondominant shoulder (P ≤ 0.01) for internal rotation, internal rotation at 45°, abduction, and prone flexion in males and in internal rotation at 45° and prone flexion in females (Table 3). Males were significantly stronger (P ≤ 0.01) than females in all measures (Table 4).
Table 2.
Participant demographics.
| Men (n = 546) | Women (n = 73) | |
|---|---|---|
| Age, y | 18.8 ± 1.0 | 18.7 ± 0.9 |
| Mass, kga | 75.3 ± 12.2 | 62.6 ± 7.0 |
| Height, cma | 178.5 ± 7.5 | 165.4 ± 7.0 |
a
Table 3.
Isometric shoulder strength normative data computed relative to body weight for healthy male and female subjects (mean ± SD).a
| Dominant | Nondominant | ||
|---|---|---|---|
| External rotation | Males | 0.20 ± 0.04 | 0.19 ± 0.05 |
| Females | 0.16 ± 0.04 | 0.15 ± 0.04 | |
| Internal rotation | Males | 0.27 ± 0.06 | 0.27 ± 0.06 |
| Females | 0.21 ± 0.05 | 0.21 ± 0.06 | |
| Abduction | Males | 0.35 ± 0.08 | 0.35 ± 0.08 |
| Females | 0.29 ± 0.10 | 0.29 ± 0.10 | |
| External rotation, 45° abduction | Males | 0.22 ± 0.05 | 0.22 ± 0.05 |
| Females | 0.18 ± 0.04 | 0.18 ± 0.04 | |
| Internal rotation, 45° abduction | Males | 0.26 ± 0.05b | 0.25 ± 0.05 |
| Females | 0.21 ± 0.05 | 0.20 ± 0.05 | |
| Prone flexion | Males | 0.12 ± 0.03b | 0.11 ± 0.03 |
| Females | 0.10 ± 0.03 | 0.10 ± 0.03 |
Each difference between males and females significant at P < 0.001.
Statistically significant side-to-side difference at P ≤ 0.01.
Table 4.
Isometric shoulder strength percentiles computed relative to body weight by hand dominance for male and female subjects.
| Dominant | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| External Rotation | Internal Rotation | Abduction | External Rotation 45° | Internal Rotation 45° | Prone Flexion | |||||||
| Male | Female | Male | Female | Male | Female | Male | Female | Male | Female | Male | Female | |
| 5th | 0.14 | 0.11 | 0.18 | 0.13 | 0.23 | 0.18 | 0.15 | 0.11 | 0.17 | 0.15 | 0.07 | 0.05 |
| 25th | 0.17 | 0.14 | 0.24 | 0.18 | 0.30 | 0.23 | 0.19 | 0.15 | 0.22 | 0.18 | 0.10 | 0.08 |
| 50th | 0.19 | 0.16 | 0.27 | 0.21 | 0.35 | 0.29 | 0.22 | 0.17 | 0.26 | 0.21 | 0.11 | 0.10 |
| 75th | 0.22 | 0.18 | 0.32 | 0.24 | 0.40 | 0.34 | 0.24 | 0.20 | 0.29 | 0.23 | 0.14 | 0.12 |
| 95th | 0.26 | 0.23 | 0.37 | 0.31 | 0.49 | 0.44 | 0.30 | 0.25 | 0.35 | 0.31 | 0.18 | 0.17 |
| Nondominant | ||||||||||||
| 5th | 0.13 | 0.10 | 0.18 | 0.13 | 0.23 | 0.17 | 0.15 | 0.12 | 0.17 | 0.13 | 0.06 | 0.06 |
| 25th | 0.16 | 0.13 | 0.23 | 0.18 | 0.29 | 0.21 | 0.19 | 0.15 | 0.22 | 0.17 | 0.09 | 0.08 |
| 50th | 0.19 | 0.15 | 0.27 | 0.20 | 0.34 | 0.28 | 0.21 | 0.17 | 0.25 | 0.20 | 0.11 | 0.09 |
| 75th | 0.22 | 0.18 | 0.30 | 0.24 | 0.40 | 0.34 | 0.24 | 0.20 | 0.29 | 0.22 | 0.13 | 0.11 |
| 95th | 0.27 | 0.20 | 0.36 | 0.33 | 0.47 | 0.47 | 0.29 | 0.26 | 0.34 | 0.30 | 0.17 | 0.16 |
Discussion
Isometric testing offers a practical, reliable,8,23,25 and cost-effective alternative to more costly and time-consuming isokinetic testing when evaluating strength. Handheld dynamometry strength measures have demonstrated high concurrent validity when compared with the established standard, isokinetic measurements.14 Clinicians frequently gauge strength by deficiency in the affected side.9,10,32 These data indicate that there may be an underlying difference in side-to-side strength measures in some positions with the dominant side being stronger than the nondominant side. Riemann et al reported dominant internal rotation is stronger in healthy subjects aged 20 to 40 years.23 The differences in the current study were small (0.01%-0.02% body weight). Work and leisure activities can contribute to unilateral strength discrepancies.2,23
Shoulder strength assessments are a valuable component of the physical examination. In adolescent female volleyball athletes, shoulder dysfunction was related to strength ratio deficits, suggesting that preventive shoulder eccentric strengthening programs focused on correcting imbalances between medial and lateral rotators may be warranted.27 Similar conclusions are seen in young tennis players18,24 and in female athletes in general.17 The relationship between strength and the risk of shoulder injury is unknown.5 Prospective studies are needed to determine if shoulder strength measures are associated with the subsequent risk of shoulder instability.
An important limitation in the current investigation is the generalizability of the relatively homogeneous male dominance in the study population. The study has several strengths, including strength measurements bilaterally on 619 physically active, healthy university students. Nearly 75% participated in high school athletics, and all met the baseline medical and physical fitness standards for military service. As a result, the findings of the current study are probably most comparable with young athletic high school or college-age populations.
Footnotes
The views and opinions expressed in this manuscript are those of the author(s) and do not reflect the official policy of the Department of the Army, the Department of Defense, or the U.S. Government.
One or more of the authors has declared a potential conflct of interest: This project was aided by a grant from the Orthopaedic Research and Education Foundation.
References
- 1.Andrews AW, Thomas MW, Bohannon RW. Normative values for isometric muscle force measurements obtained with hand-held dynamometers. Phys Ther. 1996;76(3):248-259 [DOI] [PubMed] [Google Scholar]
- 2.Bohannon RW. Reference values for extremity muscle strength obtained by hand-held dynamometry from adults aged 20 to 79 years. Arch Phys Med Rehabil. 1997;78(1):26-32 [DOI] [PubMed] [Google Scholar]
- 3.Bohannon RW, Andrews AW. Interrater reliability of hand-held dynamometry. Phys Ther. 1987;67(6):931-933 [DOI] [PubMed] [Google Scholar]
- 4.Bohannon RW, Saunders N. Hand-held dynamometry: a single trial may be adequate for measuring muscle strength in healthy individuals. Physiother Can. 1990;42(1):6-9 [Google Scholar]
- 5.Edouard P, Degache F, Beguin L, et al. Rotator cuff strength in recurrent anterior shoulder instability. J Bone Joint Surg Am. 2011;93(8):759-765 [DOI] [PubMed] [Google Scholar]
- 6.Forthomme B, Dvir Z, Crielaard JM, Croisier JL. Isokinetic assessment of the shoulder rotators: a study of optimal test position. Clin Physiol Funct Imaging. 2011;31(3):227-232 [DOI] [PubMed] [Google Scholar]
- 7.Harbo T, Brincks J, Andersen H. Maximal isokinetic and isometric muscle strength of major muscle groups related to age, body mass, height, and sex in 178 healthy subjects. Eur J Appl Physiol. 2012;112(1):267-275 [DOI] [PubMed] [Google Scholar]
- 8.Hayes K, Walton JR, Szomor ZL, Murrell GA. Reliability of 3 methods for assessing shoulder strength. J Shoulder Elbow Surg. 2002;11(1):33-39 [DOI] [PubMed] [Google Scholar]
- 9.Hughes RE, Johnson ME, O’Driscoll SW, An KN. Age-related changes in normal isometric shoulder strength. Am J Sports Med. 1999;27(5): 651-657 [DOI] [PubMed] [Google Scholar]
- 10.Katolik LI, Romeo AA, Cole BJ, Verma NN, Hayden JK, Bach BR. Normalization of the Constant score. J Shoulder Elbow Surg. 2005;14(3):279-285 [DOI] [PubMed] [Google Scholar]
- 11.Kendall F, McCreary E, Provance P, Rogers M. Muscles: Testing and Function With Posture and Pain. New York, NY: Lippincott Williams & Wilkins; 2005 [Google Scholar]
- 12.Kim HM, Teefey SA, Zelig A, Galatz LM, Keener JD, Yamaguchi K. Shoulder strength in asymptomatic individuals with intact compared with torn rotator cuffs. J Bone Joint Surg Am. 2009;91(2):289-296 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kolber MJ, Beekhuizen KS, Cheng MS, Hellman MA. Shoulder joint and muscle characteristics in the recreational weight training population. J Strength Cond Res. 2009;23(1):148-157 [DOI] [PubMed] [Google Scholar]
- 14.Kolber MJ, Cleland JA. Strength testing using hand-held dynamometry. Phys Ther Rev. 2005;10:99-112 [Google Scholar]
- 15.MacDermid JC, Ramos J, Drosdowech D, Faber K, Patterson S. The impact of rotator cuff pathology on isometric and isokinetic strength, function, and quality of life. J Shoulder Elbow Surg. 2004;13(6):593-598 [DOI] [PubMed] [Google Scholar]
- 16.Mountcastle SB, Posner M, Kragh JF, Jr, Taylor DC. Gender differences in anterior cruciate ligament injury vary with activity: epidemiology of anterior cruciate ligament injuries in a young, athletic population. Am J Sports Med. 2007;35(10):1635-1642 [DOI] [PubMed] [Google Scholar]
- 17.Niederbracht Y, Shim AL, Sloniger MA, Paternostro-Bayles M, Short TH. Effects of a shoulder injury prevention strength training program on eccentric external rotator muscle strength and glenohumeral joint imbalance in female overhead activity athletes. J Strength Cond Res. 2008;22(1):140-145 [DOI] [PubMed] [Google Scholar]
- 18.Owens BD, Agel J, Mountcastle SB, Cameron KL, Nelson BJ. Incidence of glenohumeral instability in collegiate athletics. Am J Sports Med. 2009;37(9):1750-1754 [DOI] [PubMed] [Google Scholar]
- 19.Owens BD, Duffey ML, Deberardino TM, Cameron KL. Physical examination findings in young athletes correlate with history of shoulder instability. Orthopedics. 2011;34(6):460. [DOI] [PubMed] [Google Scholar]
- 20.Petersen SM, Wyatt SN. Lower trapezius muscle strength in individuals with unilateral neck pain. J Orthop Sports Phys Ther. 2011;41(4):260-265 [DOI] [PubMed] [Google Scholar]
- 21.Rabin SI, Post M. A comparative study of clinical muscle testing and Cybex evaluation after shoulder operations. Clin Orthop. 1990(258):147-156 [PubMed] [Google Scholar]
- 22.Reinold M, Escamilla R, Wilk K. Current concepts in the scientific and clinical rationale behind exercises for glenohumeral and scapulothoracic musculature. J Orthop Sports Phys Ther. 2009;39(2):105-117 [DOI] [PubMed] [Google Scholar]
- 23.Riemann BL, Davies GJ, Ludwig L, Gardenhour H. Hand-held dynamometer testing of the internal and external rotator musculature based on selected positions to establish normative data and unilateral ratios. J Shoulder Elbow Surg. 2010;19(8):1175-1183 [DOI] [PubMed] [Google Scholar]
- 24.Roetert EP, Ellenbecker TS, Chu DA, Bugg BS. Tennis-specific shoulder and trunk strength training. Strength Cond. 1997;19(3):31-43 [Google Scholar]
- 25.Roy JS, MacDermid JC, Orton B, et al. The concurrent validity of a hand-held versus a stationary dynamometer in testing isometric shoulder strength. J Hand Ther. 2009;22(4):320-326 [DOI] [PubMed] [Google Scholar]
- 26.Schwartz S, Cohen ME, Herbison GJ, Shah A. Relationship between two measures of upper extremity strength: manual muscle test compared to hand-held myometry. Arch Phys Med Rehabil. 1992;73(11):1063-1068 [PubMed] [Google Scholar]
- 27.Stickley CD, Hetzler RK, Freemyer BG, Kimura IF. Isokinetic peak torque ratios and shoulder injury history in adolescent female volleyball athletes. J Athl Train. 2008;43(6):571-577 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Sullivan SJ, Chesley A, Hebert G, McFaull S, Scullion D. The validity and reliability of hand-held dynamometry in assessing isometric external rotator performance. J Orthop Sports Phys Ther. 1988;10(6):213-217 [DOI] [PubMed] [Google Scholar]
- 29.Turner N, Ferguson K, Mobley BW, Riemann B, Davies G. Establishing normative data on scapulothoracic musculature using handheld dynamometry. J Sport Rehabil. 2009;18(4):502-520 [DOI] [PubMed] [Google Scholar]
- 30.Veeger HEJ, van der Helm FCT. Shoulder function: The perfect compromise between mobility and stability. J Biomech. 2007;40(10):2119-2129 [DOI] [PubMed] [Google Scholar]
- 31.Wang HK, Cochrane T. Mobility impairment, muscle imbalance, muscle weakness, scapular asymmetry and shoulder injury in elite volleyball athletes. J Sports Med Phys Fitness. 2001;41(3):403-410 [PubMed] [Google Scholar]
- 32.Yian EH, Ramappa AJ, Arneberg O, Gerber C. The constant score in normal shoulders. J Shoulder Elbow Surg. 2005;14(2):128-133 [DOI] [PubMed] [Google Scholar]