

Abstract
Ischemic steal syndrome (ISS) is a complication that can occur after the construction of a vascular access for hemodialysis. It is characterized by ischemia of the hand caused by marked reduction or reversal of flow through the arterial segment distal to the arteriovenous fistula (AVF). The diagnosis of hand ischemia is based on physical examination, but imaging studies are very useful for detecting the true cause of ischemia and for selecting an appropriate therapeutic strategy. In this report, we describe an uncommon cause of ISS in a patient on hemodialysis. The ischemia was caused by the presence of undetected flow through an older AVF on the same arm as the AVF used for dialysis. The unsuspected “steal” was disclosed by color Doppler examination of the vascular bed of the patient’s left arm. Dynamic Doppler studies then played a fundamental role in the decision to ligate the distal radio-cephalic AVF. The procedure led to the complete relief of ischemic symptoms.
Keywords: Ischemic steal syndrome, Echo-color-Doppler, Arterio-venous fistula
Sommario
La sindrome ischemica da furto è una possibile conseguenza del confezionamento dell’accesso vascolare per emodialisi. E’ caratterizzata da fenomeni ischemici a carico della mano, causati da un’inversione di flusso o da una sua riduzione marcata nel segmento arterioso distale alla fistola artero-venosa (FAV). La diagnosi di ischemia della mano è basata sull’esame clinico ma è utile ricorrere alle metodiche di imaging per individuarne la reale causa e identificare la strategia terapeutica appropriata. In questo case-report viene descritta una causa poco comune di sindrome ischemica da furto in un paziente in emodialisi cronica conseguente alla coesistenza di due fistole artero-venose sullo stesso braccio. La presenza di una doppia FAV è stata diagnosticata mediante un esame eco-color Doppler dell’arto superiore; in particolare, l’effettuazione di prove emodinamiche ha svolto un ruolo fondamentale nella scelta della procedura chirurgica consentendo la completa risoluzione della sintomatologia ischemica.
Introduction
The distal ischemic steal syndrome (ISS) is a possible complication following the construction of an arteriovenous (AV) access for hemodialysis. It occurs in approximately 1–20 percent of patients with an upper extremity access, and its clinical manifestations can include various signs and symptoms, ranging from coolness, pallor, mild paresthesia, and pain during dialysis to severe symptoms, such as pain at rest, paralysis, ulceration, tissue necrosis, and loss of one or more fingers or the entire hand [1–3]. ISS is caused by a substantial decrease or even reversal of blood flow (“steal”) through the arterial segment distal to the vascular access. These changes are due to the presence of low resistance in the AV access or to hypoperfusion secondary to distal arteriopathy. Both of these factors frequently contribute to symptomatic ischemia [4].
In this report, we describe an unusual case of ISS caused by the presence of two AV fistulas on the left forearm of a hemodialyzed patient. We propose the use of dynamic Doppler studies to select the appropriate intervention for correcting the distal hypoperfusion.
Case report
A 51-year-old Caucasian male with autosomal dominant polycystic kidney disease started hemodialysisin January 1999. His first vascular access was a latero-terminal radio-cephalic AVF on the left forearm. After approximately 1 year, the patient received a kidney transplant from a cadaver donor, but he developed chronic progressive allograft nephropathy and was forced to resume hemodialysis in September 2006. The original vascular access was used. (He had refused to have it ligated during the transplant period.) In April 2008, the original AVF had to be abandoned due to irreversible clotting, and a new AVF was constructed on the same arm, proximal to the former access, using the brachial artery (BA) and median vein (MV) and an L-T configuration.
The new AVF was patent and functioned well, but the patient complained of increasingly severe, sharp pain in the left hand during dialysis. The pain was so severe that the patient was often unable to complete dialysis, and his dry weight increased considerably. For this reason, the AVF was examined with color Doppler sonography. It revealed the presence of an LT anastomosis between the pre-bifurcation segment of the BA and the MV with predominant development of the cephalic venous branch. The AVF displayed a high flow rate (about 2000 mL/min) in the BA. Flow in the radial artery (RA) distal to the anastomosis was initially retrograde. It later became orthodromic although the flow rate was only about 18 mL/min. Ulnar artery (UA) flow had the same directional characteristics, but the flow gradually increased as the transducer was advanced toward the hand, and a rate of around 323 mL/min was recorded at the wrist. It also included a significant diastolic component, which was indicative of low resistance in the distal arterial segment of the hand (Fig. 1). Careful exploration of the site of the patient’s original radio-cephalic fistula revealed the persistence of a small residual anastomosis between the RA and cephalic vein (CV). Flow through this fistula came from the UA (via the palmar arch), and the rate was about 300 mL/min. This finding was confirmed by the presence of an audible thrill over the radio-cephalic AVF. The concomitant presence of two functioning vascular accesses on the same arm – a distal, radio-cephalic fistula with limited flow (about 300 mL/min) and a proximal brachio-median fistula with high flow (about 2000 mL/min) – was thus identified as the cause of symptoms of hypoperfusion.
Fig. 1.
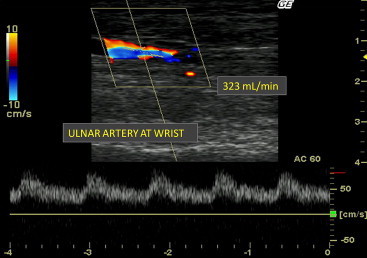
Color Doppler ultrasound: characteristics of the ulnar artery at first evaluation.
Dynamic Doppler studies were performed to determine whether surgical ligation of one of the fistulas could be performed to improve the patient’s clinical symptoms. Each of the AVFs was manually compressed, and the hemodynamic effects of this maneuver were assessed. Compression of the proximal AVF did not produce any substantial changes in arterial or venous flow in the left forearm. In particular, it did not increase the flow through the distal AVF to values suitable for use in dialysis (Fig. 2). In contrast, compression of the distal AVF caused a marked change in the Doppler trace of the UA, which became triphasic (high-resistance), and a reduction of the UA flow rate from 333 to 133 mL/min (Figs. 3 and 4). The patient was therefore scheduled for surgical ligation of the distal radio-cephalic AVF.
Fig. 2.
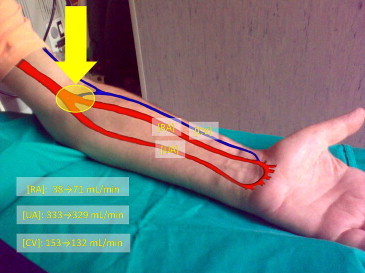
Doppler dynamic test: manual compression of the proximal AVF [UA]: ulnar artery; [RA]: radial artery; [CV]: cephalic vein.
Fig. 3.
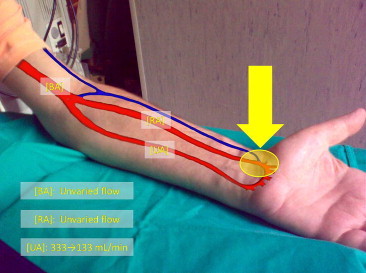
Doppler dynamic test: manual compression of the distal AVF [UA]: ulnar artery; [RA]: radial artery; [BA]: brachial artery.
Fig. 4.

Color Doppler ultrasound: characteristics of the ulnar artery after compression of the distal AVF.
Ten days after surgery, color Doppler sonography was repeated. The study confirmed the closure of distal anastomosis and the presence of high flow through the proximal AVF (2221 mL/min). RA flow remained low (17 mL/min), while the UA continued to display triphasic, high-resistance flow regularly directed toward the hand. These ultrasound findings were associated with an improvement in clinical manifestations of the ISS, and within a few days all ischemic symptoms had disappeared.
Informed consent was obtained from the patient.
Discussion
ISS is a serious clinical condition. Not only does the pain reduce the patient’s ability to tolerate hemodialysis, the ischemia can lead to tissue necrosis and eventual loss of fingers and even the entire hand. Retrograde flow can be demonstrated in the vast majority of vascular accesses, but only a few patients have clinical signs of ISS. Factors other than retrograde flow often play an important role in the development of ischemic symptoms. The most common are diabetes, smoking, and peripheral vascular disease. Therefore, peripheral ischemia can be caused by any one or a combination of different mechanisms (retrograde flow, stenotic lesions and distal arteriopathy). For this reason, the cause of ischemic symptoms should be investigated by means of a detailed medical history, physical examination, and careful evaluation of the arterial circulation of the extremity.
In conclusion, this case illustrates the importance of Doppler ultrasonography in the evaluation of ISS. This non-invasive technique provides important information about vascular anatomy and hemodynamics. In the case reported here, it played a decisive role in the detection of an uncommon cause of ISS (co-presence of two AVFs) and in the selection of appropriate surgical treatment. Doppler hemodynamic testing was also used to evaluate the functional effects of manual compression of each AVF. The results of these studies led to the surgical ligation of the distal radio-cephalic AVF, which was followed by marked improvement in the patient’s hand pain.
Conflict of interest statement
The authors have no conflict of interest.
References
- 1.Papasavas P.K., Reifsnyder T., Birdas T.J., Caushaj P.F., Leers S. Prediction of arteriovenous access steal syndrome utilizing digital pressure measurements. Vasc Endovascular Surg. 2003;37(3):179–184. doi: 10.1177/153857440303700304. [DOI] [PubMed] [Google Scholar]
- 2.Tordoir J.H., Dammers R., van der Sande F.M. Upper extremity ischemia and hemodialysis vascular access. Eur J Vasc Endovasc Surg. 2004;27:1–5. doi: 10.1016/j.ejvs.2003.10.007. [DOI] [PubMed] [Google Scholar]
- 3.Suding P.N., Wilson S.E. Strategies for management of ischemic steal syndrome. Semin Vasc Surg. 2007;20:184–188. doi: 10.1053/j.semvascsurg.2007.07.009. [DOI] [PubMed] [Google Scholar]
- 4.Leon C., Asif A. Arteriovenous access and hand pain: the distal hypoperfusion ischemic syndrome. Clin J Am Soc Nephrol. 2007;2(1):175–183. doi: 10.2215/CJN.02230606. [DOI] [PubMed] [Google Scholar]