

Abstract
Introduction
Hypoplasia of the internal carotid artery (HICA) is a rare congenital anomaly caused by an incomplete development of the organ, and only a few cases are reported in the literature. The prevalence of HICA (including agenesia and aplasia) is estimated to about 0.01%.
Case report
We describe a case of a 66-year-old man with hearing loss on the left side and no other symptoms or signs related to vascular impairment. HICA was discovered incidentally by color duplex sonography of the extracranial cerebral vessel and confirmed by magnetic resonance imaging angiography (angio MRI) and computed tomography (CT) of the head.
Discussion
Compensatory flow allows HICA patients to remain asymptomatic, but complications may occur. The pathways of the collateral circulation in association with aplasia or HICA are described. A differential diagnosis was made on the basis of ultrasonographic (US) detection of diffuse luminal narrowing of the internal carotid artery (ICA). Recognition of this disease has important clinical implications.
Keywords: Arteries, abnormalities; Hypoplasia internal carotid artery; Extracranial duplex sonography; Transcranial duplex sonography
Sommario
Introduzione
L'ipoplasia della carotide interna è una rara anomalia congenita che si verifica per un incompleto sviluppo dell'organo. Soltanto pochi casi sono stati riportati in letteratura. La prevalenza dell'ipoplasia se calcolata insieme alla agenesia e alla aplasia è stimata essere dello 0.01%.
Caso clinico
Descriviamo il caso di un uomo di 66 anni affetto da ipoacusia all'orecchio sinistro e nessun segno di problemi vascolari. L'ipoplasia della carotide interna fu scoperta accidentalmente durante un ecocolordoppler dei tronchi sovraortici e venne confermata da angio risonanza magnetica e tomografia assiale computerizzata del cranio.
Discussione
I flussi di compenso permettono a questi pazienti di rimanere asintomatici per molti anni ma possono essere causa nel tempo di complicazioni. Vengono descritti i pattern di circolazione collaterale associati alla ipoplasia della carotide interna. Vengono messi in evidenza i segni ultrasonografici che permettono la diagnosi differenziale in caso di diffuso restringimento del lume vascolare della arteria carotide interna. Inoltre, sottolineiamo che il riconoscimento di tale condizione ha importanti implicazioni nella pratica clinica.
Introduction
Hypoplasia of the internal carotid artery (HICA) is a rare congenital anomaly caused by an incomplete development of the organ, and only a few cases are reported in the literature [1]. The prevalence of HICA (including agenesia and aplasia) is estimated to about 0.01% [1,2], and recognition of this disease has important clinical implications. Ultrasonography (US) is usually the first examination performed to detect suspected HICA. Characteristic US findings allow the diagnosis, but magnetic resonance imaging angiography (angio MRI) and computed tomography (CT) of the skull base may be necessary to confirm US diagnosis. In our opinion HICA should be suspected in all patients who have a diffuse luminal narrowing of the internal carotid artery.
Case report
A 66-year-old man with hearing loss on the left side and no other symptoms or signs related to vascular impairment underwent examination of the extracranial cerebral vessels. Ethical approval for this study was granted by the Medical Research Ethics Committee of our hospital, and informed consent was obtained from the patient. Extracranial duplex sonography of the cerebral vessel showed kinking and diffuse luminal narrowing of the left ICA with significantly reduced flow velocity (PSV 53.5 cm/s; PEDV 15.0 cm/s; Fig. 1) which contrasted with the contralateral side (PSV 89.7 cm/s; PEDV 45.6 cm/s). The left external carotid artery showed increased diastolic (“internalized”) blood flow (Fig. 2), and the left ophthalmic artery showed inverted flow and a high diastolic component similar to that of a brain supplying artery. No other abnormalities were found. Transcranial duplex sonography revealed a difference in flow velocity between the two sides with reduced flow velocity in the left carotid siphon, in the left M1-MCA segment as well as in the left A1 ACA segment and showed absence of the A1 segment of the right anterior cerebral artery. Assessment of the posterior circulation was unremarkable.
Fig. 1.
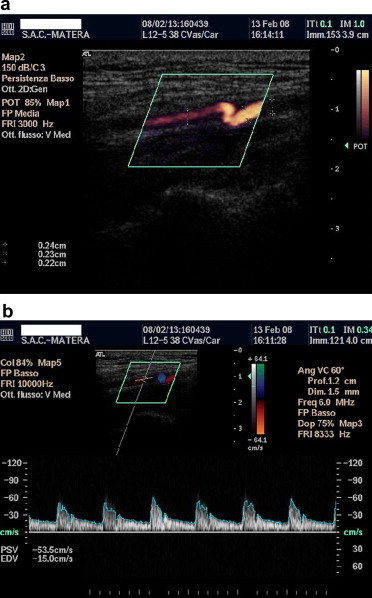
a. Extracranial duplex, longitudinal plane. There is kinking and diffuse luminal narrowing of the left internal carotid artery. b. Extracranial duplex, longitudinal plane. Reduced blood flow in the left internal carotid artery.
Fig. 2.
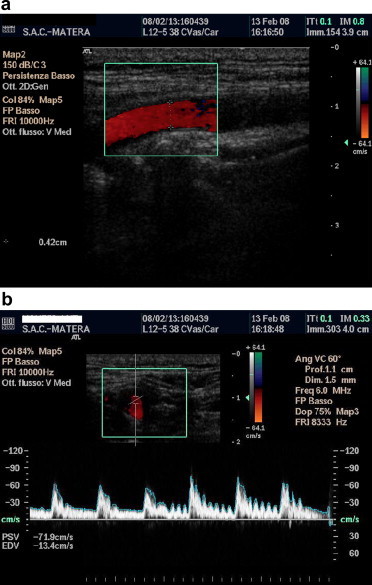
a. Extracranial duplex, longitudinal plane. US appearance of the left external carotid artery. b. Extracranial duplex, axial plane. The left external carotid artery waveform shows diastolic flow and a typical oscillation effect on mild manual oscillation of the temporal artery.
Angio MRI of the cerebral vessels showed reduced signal intensity in the left internal carotid artery (left ICA diameter 1.9 mm; right ICA diameter 5.2 mm) which was in accordance with intracranial and extracranial US findings (Fig. 3, Fig. 4). Axial CT scan of the skull base showed a normally developed right carotid canal and a diminutive left carotid canal, which is a sign of congenital ICA abnormalities.
Fig. 3.
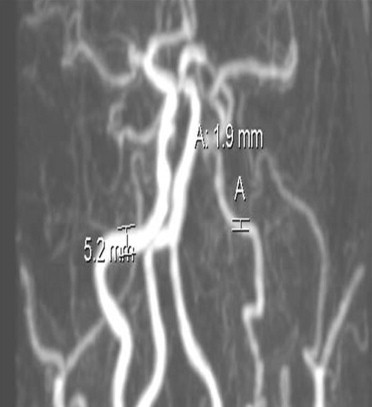
Angio MRI shows reduced signal intensity in the left internal carotid artery (a) in accordance with US findings.
Fig. 4.

Angio MRI shows normal flow in the right intracranial internal carotid artery and no visibility of the left intracranial internal carotid artery.
Discussion
Underdevelopment or absence of the internal carotid artery is an uncommon disease [1]. About 100 cases of absence or underdevelopment of the internal carotid are reported in the literature [2], but the real incidence may be higher because many patients with absence or hypoplasia of the internal carotid probably never come to medical attention.
Six pathways of collateral circulation in association with aplasia or hypoplasia (a/hypoplasia) of the ICA are described [3]. Type 1: a/hypoplasia of the ICA is associated with the anterior communicating artery (ACOM) and posterior communicating artery (PCOM) hypertrophy. The ipsilateral anterior cerebral artery (ACA) is supplied through a patent anterior communicating artery, while the middle cerebral artery (MCA) is supplied through a patent hypertrophied posterior communicating artery. Type 2: a/hypoplasia of the ICA is associated with ACOM hypertrophy, and the MCA and homolateral ACA are supplied through a patent ACOM. Type 3: a/hypoplasia of the ICA is bilateral. The anterior circulation of the brain is permitted through carotid-vertebrobasilar anastomosis. There is often PCOM hypertrophy. Type 4: there is unilateral underdevelopment of the cervical portion of the ICA associated with the transcavernous communication. The transcavernous collateral vessels may be located behind the clivus, or run above, through, or in the floor of the sella turcica [4]. Type 5: there is a bilateral hypoplasia of the ICA. The anterior cerebral arteries are supplied through hypoplastic ICAs while the middle cerebral arteries are supplied through enlarged PCOMs. Type 6: a/hypoplasia of the ICA is associated with anastomosis (rete mirabilis) from the homolateral external carotid artery. Our case showed a type 6 collateral circulation.
In our opinion, HICA deserves some important considerations. Patients with HICA may be completely asymptomatic due to collateral blood supply to the affected hemisphere, or they may present symptoms due to cerebrovascular insufficiency or compression by enlarged collateral cerebral vessels.
The increased blood flow through collateral vessels and altered flow dynamics may cause ACOM and PCOM aneurisms [5,6]. In these patients, the prevalence of intracranial aneurysm is estimated to about 24–34% while in the general population it is 2–4% [5,6].
Recognition of HICA is important also in the assessment of cerebral ischemia. Emboli in one cerebral hemisphere may be explained by an atherosclerotic disease of the contralateral carotid system or in the vertebrobasilar system.
Recognition of HICA is very important in the planning of surgical procedures such as transsphenoidal hypophyseal surgery and carotid endarterectomy. A pre-operative diagnosis of this anomaly before carotid endarterectomy is essential because both hemispheres depend on a single carotid artery. Before transsphenoidal hypophyseal surgery, the surgeon should foresee the possibility of finding an intracavernous vessel in any patient with no identifiable ICA [7].
HICA represents a diagnostic challenge for the sonographer. Diffuse luminal narrowing of the internal carotid can be caused by carotid dissection, high grade stenosis, arteritis, fibromuscular dysplasia and radiation-induced angiopathy. The hemodynamic findings in these diseases do not allow a differential diagnosis, but some signs may help to avoid US misdiagnosis.
Carotid dissection is an important cause of stroke in young patients. Although diagnostic confirmation using neuroradiological diagnostics is mandatory, US may be helpful, particularly in the initial investigation and in the follow-up. Detection of direct signs of carotid dissection is often possible: a tapering occlusion, a pseudoaneurysm resulting from the rupture of the artery and subsequent encapsulation of the paravascular hematoma, a double lumen with an intimal flap, a flat, hyperechoic structure floating in the lumen or dividing the true and the false lumen. Hypoechoic thickness of the wall, which is a sign of hematoma and intraluminal thrombus, is not pathognomonic of carotid dissection, as it could also be a sign of anechoic plaques or mural thrombus. Also indirect US signs, essentially hemodynamic changes due to high grade stenosis are not pathognomonic of carotid dissection.
Fibromuscular dysplasia is a nonatherosclerotic, noninflammatory segmental vascular disease of unknown origin. The extracranial cerebral vessels are frequently affected, particularly the distal internal carotid artery. US diagnostic findings are a segmental string-of-beads pattern with alternating regions of luminal narrowing and vessel dilatation [8].
The patient's anamnesis may cause suspicion of radiation-induced carotid angiopathy. Irradiation leads to fibrosis of the tunica media and tunica adventitia. US shows plaques, which are usually midechoic and non-calcified.
Patients with high grade arteriosclerotic lesions usually present vascular risk factors. Atherosclerotic vessel wall changes are found in several arteries. The atherosclerotic plaques are irregular and with inhomogeneous echogenicity because the lesions are often calcified.
Particularly in the Takayasu disease, arteritis may be confounding, but some aspects have to be considered. Takayasu disease occurs mainly in young women and is characterized by progressive stenoses and occlusions of the arteries arising from the aortic arch. US findings are very typical. A severe, diffuse wall thickening is observed especially in the internal and common carotid arteries. The wall deposit is typically homogeneous, midechoic, circumferential and has been described as the “macaroni sign” by Maeda et al. [9].
Large-vessel giant cell arteritis may appear in several vessels other than the temporal arteries, so we recommend considering the possibility of carotid artery involvement. US sign of giant cell arteritis is a dark halo around the artery lumen which may be due to edema of the artery wall. In clinical practice it is important to keep also this in mind, as the hypoechoic circumferential halo typical of large-vessel giant cell arteritis like the midechoic homogeneous wall thickening of the Takayasu arteritis, may disappear with corticosteroid therapy [9,10].
In our opinion, color duplex US allows diagnosis of underdevelopment of the ICA although it is sometimes difficult to distinguish between underdevelopment of the ICA and other diseases causing diffuse luminal narrowing of the vessel. However, some US signs may help to avoid diagnostic errors. In unclear cases and in cases in which US outcome is considered unreliable, angio MRI or CT of the skull base may show absence of the carotid canal as a sign of congenital ICA abnormalities. Angio MRI or CT should therefore be performed to confirm the diagnosis. Recognition of HICA may be important in the assessment of cerebrovascular diseases and in the planning of carotid and transsphenoidal hypophyseal surgery, and it should prompt further evaluation to rule out the presence of a potentially life-threatening intracranial aneurysm, even in asymptomatic patients.
Conflict of interest statement
The authors have no conflict of interest.
References
- 1.Claros P., Bandos R., Gilea I. Case report: major congenital anomalies of the internal carotid artery-agenesis, aplasia and hypoplasia. Int J Pediatr Otorhinolaryngol. 1999;49:69–76. doi: 10.1016/s0165-5876(99)00012-9. [DOI] [PubMed] [Google Scholar]
- 2.Chen Cj, Chen S.T., Hsieh F.Y., Wang L.J., Wong Y.C. Hypoplasia of the internal carotid artery with intercavernous anastomosis. Neuroradiology. 1998;40:252–254. doi: 10.1007/s002340050578. [DOI] [PubMed] [Google Scholar]
- 3.Lie T.A. Excerpta Medica; Amsterdam: 1968. Congenital anomalies of the carotid arteries. p. 35–41. [Google Scholar]
- 4.Janicki P.C., Limbacher J.P., Guinto F.C., Jr. Agenesis of the internal carotid artery with a primitive transsellar communicating artery. AJR Am J Roentgenol. 1979;132:130–132. doi: 10.2214/ajr.132.1.130. [DOI] [PubMed] [Google Scholar]
- 5.Afifi A.K., Godersky J.C., Menezes A., Smoker W.R., Bell W.E., Jacoby C.G. Cerebral hemiatrophy, hypoplasia of internal carotid artery and intracranial aneurysm: a rare association occurring in an infant. Arch Neurol. 1987;44:232–235. doi: 10.1001/archneur.1987.00520140090024. [DOI] [PubMed] [Google Scholar]
- 6.Quint D.J., Boulos R.S., Spera T.D. Congenital absence of the cervical and petrous internal carotid artery with intercavernous anastomosis. AJNR Am J Neuroradiol. 1989;10:435–442. [PMC free article] [PubMed] [Google Scholar]
- 7.Kishore P.R., Kaufman A.B., Melichar F.A. Intrasellar carotid anastomosis simulating pituitary microadenoma. Radiology. 1979;132:381–383. doi: 10.1148/132.2.381. [DOI] [PubMed] [Google Scholar]
- 8.Arning C., Grzyska U. Color Doppler imaging of cervicocephalic fibromuscular dysplasia. Cardiovasc Ultrasound. 2004;20(2):7. doi: 10.1186/1476-7120-2-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Maeda H., Handa N., Matsumoto M. Carotid lesions detected by B-mode ultrasonography in Takayasu's arteritis: “macaroni sign” as an indicator of the disease. Ultrasound Med Biol. 1991;17:695–701. doi: 10.1016/0301-5629(91)90101-2. [DOI] [PubMed] [Google Scholar]
- 10.Nicoletti G., Ciancio G., Tardi S., Olivieri I. Colour duplex ultrasonography in the management of giant cell arteritis. Clin Rheumatol. 2003;22:508–509. doi: 10.1007/s10067-003-0813-3. [DOI] [PubMed] [Google Scholar]