

Abstract
Knee osteoarthritis commonly occurs in the medial compartment of the knee and has been linked to overloading of the medial articular cartilage. Gait modification represents a non-invasive treatment strategy for reducing medial compartment knee force. The purpose of this study was to evaluate the effectiveness of a variety of gait modifications that were expected to alter medial contact force. A single subject implanted with a force-measuring knee replacement walked using nine modified gait patterns, four of which involved different hiking pole configurations. Medial and lateral contact force at 25%, 50%, and 75% of stance phase, and the average value over all of stance phase (0-100%), were determined for each gait pattern. Changes in medial and lateral contact force values relative to the subject’s normal gait pattern were determined by a Kruskal-Wallis test. Apart from early stance (25% of stance), medial contact force was most effectively reduced by walking with long hiking poles and wide pole placement, which significantly reduced medial and lateral contact force during stance phase by up to 34% (at 75% of stance) and 26% (at 50% of stance), respectively. Although this study is based on data from a single subject, the results provide important insight into changes in medial and lateral contact forces through gait modification. The results of this study suggest that an optimal configuration of bilateral hiking poles may significantly reduce both medial and lateral compartment knee forces in individuals with medial knee osteoarthritis.
Keywords: Knee osteoarthritis, In vivo knee loads, Gait retraining, Walking, Biomechanics
INTRODUCTION
Knee osteoarthritis (OA) affects a large segment of the population1 and occurs frequently in the medial compartment of the knee.2 The development of medial compartment knee OA has been attributed to overloading of the medial compartment articular cartilage.3 Therefore, treatment strategies (e.g., high tibial osteotomy, gait modification) are often focused on reducing medial compartment knee loads.
Gait modification represents a non-invasive method for reducing medial knee compartment loads. Previous studies have evaluated a variety of gait modifications for their ability to reduce the external knee adduction moment. Gait modifications that reduce this moment include walking while pointing the toes outward,4,5 walking at a reduced speed,6,7 walking with increased medial-lateral trunk sway,8-10 walking with medialized knees (i.e., medial thrust gait),11-13 and walking with hiking poles.12 The external knee adduction moment is often used as a surrogate measure for medial compartment force and has been shown to be highly correlated with medial contact force.14 However, a recent study showed that reductions in the external knee adduction moment can be achieved without corresponding reductions in medial compartment force.12 Therefore, changes in external knee adduction moment may not accurately reflect changes in medial compartment loading. Direct measurements of changes in medial contact force are important for determining the effectiveness of gait modifications at reducing medial compartment loading.
Assessment of gait modifications through direct measurement of contact forces is difficult because in vivo knee contact forces cannot be easily measured. However, force-measuring knee implants allow for in vivo measurement of knee contact forces15-17 and provide the ability to evaluate the effectiveness of different gait modifications at reducing medial contact force. A previous study found that medial thrust gait and walking with bilateral hiking poles reduced the in vivo medial contact force peak in late stance significantly in a subject implanted with a force-measuring tibial prosthesis.11 A related study performed with the same subject reported that increased knee flexion produced by a crouched gait pattern may increase knee contact force.12 Apart from these studies, in vivo data that quantify how knee contact forces change in response to gait modification remain scarce. Furthermore, other gait patterns that could positively or negatively impact medial contact force, such as walking so that the forefoot strikes the ground before the heel (forefoot strike gait), walking in a bouncy fashion, or walking with hiking poles in different configurations, have not been investigated. Although not a typical gait modification for reducing medial contact force, we expected forefoot strike gait to reduce knee joint loading in early stance by avoiding the high impact forces at heel strike in a typical gait pattern where the heel strikes the ground first. We also chose to investigate bouncy gait to investigate the effects of superior-inferior pelvis translation on knee joint loading.
This study expands on previous studies by investigating how a broad spectrum of gait modifications (medial thrust, mild crouch, moderate crouch, forefoot strike, and bouncy gait) and four hiking pole configurations change the magnitude of medial and lateral contact forces in the knee. A single subject implanted with a force-measuring knee replacement performed each modified gait pattern. Direct measurement of contact forces will provide insight into changes in knee joint loading through gait modification, which is commonly accepted as a contributing factor to the development and progression of knee OA3. By analyzing in vivo measurements of knee contact force, this study provides unique insight into the effectiveness of a variety of gait modifications that could be adopted by individuals suffering from medial compartment knee OA. In addition, the results have implications for designing successful non-invasive treatments for individuals with knee OA.
METHODS
Experimental data were collected from a single subject implanted with a cruciate-retaining force-measuring knee replacement (male, right knee, seven years post-implantation, age: 88 years, mass: 64.8 kg).18 The subject’s custom knee replacement was instrumented with four uniaxial force transducers that measured compressive force at the four corners of the tibial tray.15 Institutional review board approval and subject informed consent were obtained prior to testing.
Internal knee contact force15 and external ground reaction data were collected simultaneously while the subject performed a minimum of five trials of ten different overground gait patterns: normal, mild crouch, moderate crouch, medial thrust, forefoot strike, bouncy, and four hiking pole conditions (combinations of short and long hiking poles with normal and wide pole placement). Walking speed was controlled for all trials to allow for comparison of contact forces across conditions at similar walking speeds. Descriptions of the gait patterns are provided in Table 1 and Figure 1. For each gait trial, internal knee contact force data were recorded from the instrumented tibial prosthesis15 and external ground reaction data were recorded from three force plates (Bertec Corporation, Columbus, OH, USA).
Table 1.
Descriptions of each gait modification.
| Gait modification | Verbal Instructions |
|---|---|
| Mild Crouch | Crouched position with a mild increase in knee flexion angle. |
| Moderate Crouch | Crouched position with a moderate increase in knee flexion angle. |
| Medial Thrust | Internally rotated hip of the stance leg so that the knees were medialized during stance. The subject was instructed not to increase knee flexion during stance. |
| Forefoot Strike | Striking the ground with the forefoot rather than the heel at initial contact. |
| Bouncy | Increased superior-inferior translation of the pelvis during the gait cycle. |
| Walking pole conditions | Walking with hiking poles. The subject was instructed to place the tip of the ipsilateral pole on the ground opposite the contralateral heel at the instant of heel strike. |
| Short hiking poles, normal pole placement | Hiking pole length was 10% shorter than the manufacturer’s recommendations. Hiking poles were placed with the tip on the ground at approximately shoulder width on the ipsilateral side. |
| Long hiking poles, normal pole placement | Hiking pole length corresponded to the length recommended by the manufacturer, where in a standing position the elbow is at a 90° angle when the pole is vertical with the tip on the ground. Hiking poles were placed with the tip on the ground at approximately shoulder width on the ipsilateral side. |
| Short hiking poles, wide pole placement | Hiking pole length was 10% shorter than the manufacturer’s recommendations. Hiking poles were placed at a wide width achieved by externally rotating the shoulder as far as comfortable. |
| Long hiking poles, wide pole placement | Hiking pole length corresponded to the length recommended by the manufacturer, where in a standing position the elbow is at a 90° angle when the pole is vertical with the tip on the ground. Hiking poles were placed at a wide width achieved by externally rotating the shoulder as far as comfortable. |
Figure 1.
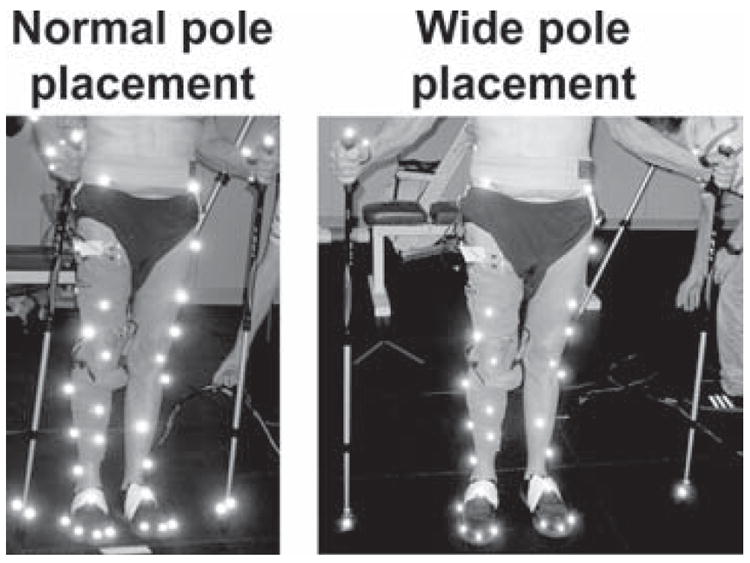
Photos of hiking pole placement during the normal (left) and wide (right) conditions.
The subject was given verbal instructions and allowed time to learn each gait pattern. For medial thrust gait, the subject was instructed to internally rotate the hip of the stance leg so that the knee was medialized during stance.12 The subject was also instructed not to increase knee flexion during stance as recommended by a previous study.12 For the four hiking pole conditions, the subject used two Leki Makalu Tour trekking poles (Leki Lenhart GmbH, Kirchheim/Teck, Germany) and was instructed to place the tip of the ipsilateral pole on the ground opposite the contralateral heel at the instant of heel strike. The long pole length corresponded to the length recommended by the manufacturer, where in a standing position the elbow is at a 90° angle when the pole is vertical with the tip on the ground. The short pole length was 10% shorter. The normal pole placement involved placing the pole tip on the ground at approximately shoulder width on the ipsilateral side, which is the most natural tip placement width (Fig. 1, left image). The wide pole placement involved a lateralized tip placement on the ground, achieved by externally rotating the shoulder as far as comfortable (Fig. 1, right image).
Medial and lateral contact forces were calculated from the implant’s force transducer data using previously validated regression equations (Equations 1 and 2) developed for the subject’s implant.14 The regression equations are
| (1) |
| (2) |
where FM and FL are the medial and lateral contact force, respectively, C1 (0.9871), C2 (0.9683), C3 (0.0387), and C4 (0.0211) are the regression coefficients and the subscripts A, M, P, and L represent the anterior, medial, posterior, and lateral force transducers in the instrumented implant, respectively14.
All medial and lateral contact force data were normalized to the subject’s body weight and then time normalized to 100% of stance phase by identifying gait cycle events from the vertical ground reaction force data. Medial and lateral contact force at 25%, 50%, and 75% of stance phase, and the average value over all of stance phase (0-100%), were determined for ten stance phases (five trials with two stance phases per trial) of each gait pattern. Contact forces at discrete values in stance phase were chosen for comparison to previous studies that evaluated similar changes in contact forces11,12 and changes in peak external knee adduction moments4-10,13. Changes in walking speed and medial and lateral contact force for the modified gait patterns relative to the subject’s normal gait pattern were determined using a Kruskal-Wallis test. When significant (p < 0.05) differences were found, pairwise comparisons using a Tukey’s Honestly Significant Difference correction were performed to determine which conditions were significantly different from the normal condition. All data analysis was completed using MATLAB (The Mathworks, Natick, MA, USA).
RESULTS
Average walking speed for all conditions was 1.22 ± 0.08 m/s and no statistically significant differences were found between walking speed during any gait modification relative to the normal condition (p = 0.5). Relative to normal gait, hiking pole gaits with wide pole placement were the only gait modifications to produce statistically significant changes in medial contact force (Fig. 2, Table 2). No hiking pole configuration produced statistically significant changes at 25% of stance phase relative to the normal condition (p > 0.05), while only long hiking poles with wide pole placement produced significant changes at all remaining time points (p < 0.001, 95% Confidence Intervals (CI) at 50%: [5.9, 87.1], 75%: [22.6, 103.8], 0-100%: [9.1, 90.3]). These reductions ranged from 18% over all of stance phase (i.e., 0-100%) to 34% at 75% of stance phase. In addition, short hiking poles with wide pole placement produced a significant reduction of 21% at 75% of stance phase (p < 0.001, 95% CI [5.1, 86.3]).
Figure 2.
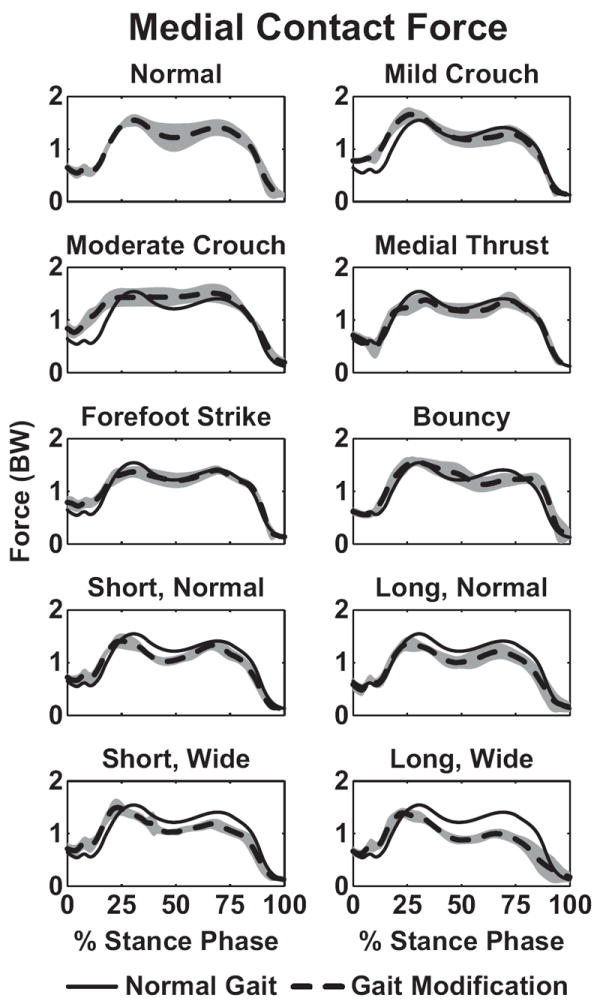
Average curves for medial knee contact force during the stance phase of gait from five trials of each gait modification. For each gait modification the average data (dashed line) and standard deviation (gray shaded area) are shown. The average curve for normal gait (solid line) is also shown for comparison.
Table 2.
Medial knee contact force at 25%, 50% and 75% of the stance phase and the average value over the stance phase (0-100%).
| 25% | 50% | 75% | 0-100% | |||||
|---|---|---|---|---|---|---|---|---|
| Avg (SD) | % Diff. | Avg (SD) | % Diff. | Avg (SD) | % Diff. | Avg (SD) | % Diff. | |
| Normal | 1.44 (0.07) | - | 1.22 (0.27) | - | 1.35 (0.15) | - | 1.06 (0.08) | - |
| Mild Crouch | 1.64 (0.15) | 14 | 1.18 (0.15) | -2 | 1.27 (0.15) | -6 | 1.10 (0.08) | 4 |
| Moderate Crouch | 1.43 (0.18) | -1 | 1.44 (0.16) | 18 | 1.42 (0.17) | 5 | 1.20 (0.11) | 13 |
| Medial Thrust | 1.24 (0.16) | -14 | 1.17 (0.15) | -4 | 1.34 (0.15) | -1 | 1.02 (0.06) | -4 |
| Forefoot Strike | 1.32 (0.13) | -9 | 1.21 (0.15) | -1 | 1.29 (0.07) | -4 | 1.07 (0.06) | 1 |
| Bouncy | 1.50 (0.14) | 4 | 1.30 (0.20) | 7 | 1.23 (0.11) | -9 | 1.09 (0.06) | 3 |
| Short, normal | 1.40 (0.15) | -3 | 1.05 (0.09) | -14 | 1.16 (0.12) | -14 | 0.98 (0.05) | -8 |
| Long, normal | 1.35 (0.14) | -6 | 1.01 (0.12) | -17 | 1.11 (0.14) | -18 | 0.92 (0.06) | -13 |
| Short, wide | 1.47 (0.13) | 2 | 1.03 (0.06) | -15 | 1.06 (0.10) | -21 | 0.97 (0.05) | -8 |
| Long, wide | 1.37 (0.11) | -5 | 0.88 (0.08) | -28 | 0.89 (0.10) | -34 | 0.87 (0.06) | -18 |
Average and standard deviation values (in BW) were calculated for ten stance phases of each gait pattern. Percent difference values (% Diff.) were calculated for each gait modification relative to the normal condition. Bold values indicate statistically significant differences from the normal condition (p < 0.05).
Lateral contact force was significantly changed by five of the nine modified gait patterns relative to normal gait (Fig. 3, Table 3). Mild crouch gait significantly reduced lateral contact force by 23% at 25% of stance phase (p = 0.08, 95% CI [1.0, 82.2]) and by 12% over all of stance phase (p = 0.003, 95% CI [1.0, 82.2]), while moderate crouch and bouncy gait reduced lateral contact force by 29% (p < 0.001, 95% CI [25.3, 108.9]) and 36% (p < 0.001, 95% CI [32.2, 113.4]), respectively, at 75% of stance phase. Statistically significant reductions in lateral contact force achieved by the various hiking pole configurations mirrored those observed for medial contact force. Specifically, no hiking pole condition produced statistically significant changes at 25% of stance phase (p > 0.05), while only long hiking poles with wide pole placement produced significant reductions at all remaining time points (p < 0.001, 95% CI at 50%: [9.1, 90.4], 75%: [12.9, 94.1], 0-100%: [12.1, 93.3]). These reductions ranged from 14% over all of stance phase (i.e., 0-100%) to 26% at 50% of stance phase. In addition, short hiking poles with wide pole placement produced a significant reduction of 19% at 75% of stance phase (p < 0.001, 95% CI [4.0, 85.2]).
Figure 3.
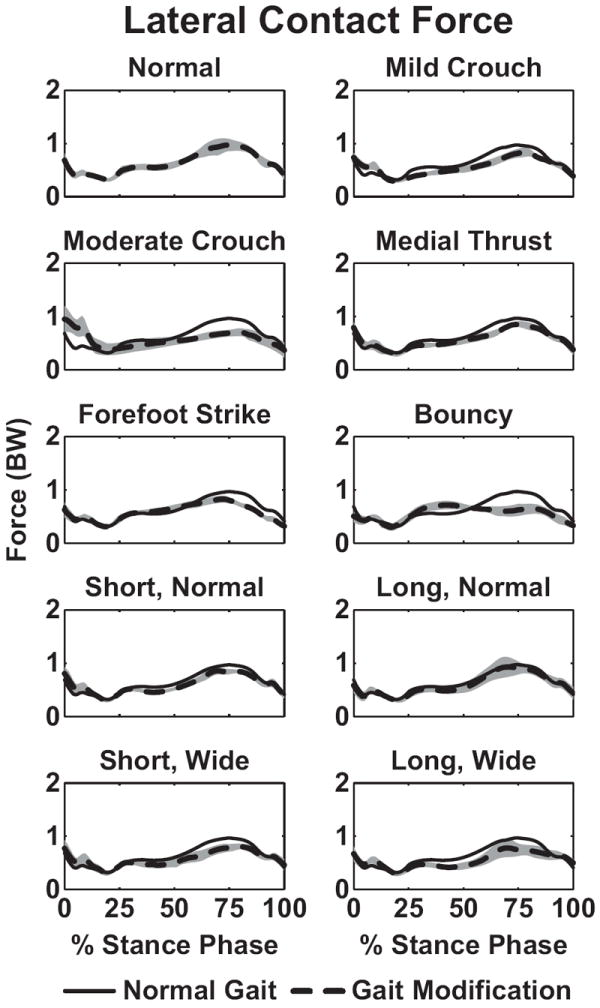
Average curves for lateral knee contact force during the stance phase of gait from five trials of each gait modification. For each gait modification the average data (dashed line) and standard deviation (gray shaded area) are shown. The average curve for normal gait (solid line) is also shown for comparison.
Table 3.
Lateral knee contact force at 25%, 50% and 75% of the stance phase and the average value over the stance phase (0-100%).
| 25% | 50% | 75% | 0-100% | |||||
|---|---|---|---|---|---|---|---|---|
| Avg (SD) | % Diff. | Avg (SD) | % Diff. | Avg (SD) | % Diff. | Avg (SD) | % Diff. | |
| Normal | 0.46 (0.08) | - | 0.60 (0.06) | - | 0.97 (0.11) | - | 0.63 (0.04) | - |
| Mild Crouch | 0.35 (0.04) | -23 | 0.51 (0.06) | -15 | 0.82 (0.08) | -16 | 0.56 (0.04) | -12 |
| Moderate Crouch | 0.40 (0.11) | -11 | 0.54 (0.07) | -11 | 0.69 (0.07) | -29 | 0.57 (0.08) | -9 |
| Medial Thrust | 0.41 (0.06) | -11 | 0.55 (0.07) | -8 | 0.86 (0.05) | -12 | 0.57 (0.03) | -10 |
| Forefoot Strike | 0.45 (0.07) | -1 | 0.66 (0.06) | 9 | 0.80 (0.06) | -17 | 0.58 (0.02) | -8 |
| Bouncy | 0.48 (0.08) | 4 | 0.69 (0.05) | 14 | 0.62 (0.11) | -36 | 0.56 (0.04) | -11 |
| Short, normal | 0.43 (0.05) | -7 | 0.52 (0.03) | -14 | 0.84 (0.05) | -13 | 0.59 (0.02) | -7 |
| Long, normal | 0.39 (0.07) | -14 | 0.52 (0.08) | -13 | 0.91 (0.12) | -6 | 0.60 (0.05) | -6 |
| Short, wide | 0.44 (0.06) | -3 | 0.50 (0.08) | -17 | 0.78 (0.07) | -19 | 0.57 (0.04) | -9 |
| Long, wide | 0.40 (0.07) | -13 | 0.44 (0.07) | -26 | 0.75 (0.12) | -23 | 0.55 (0.03) | -14 |
Average and standard deviation values (in BW) were calculated for ten stance phases of each gait pattern. Percent difference values (% Diff.) were calculated for each gait modification relative to the normal condition. Bold values indicate statistically significant differences from the normal condition (p < 0.05).
DISCUSSION
This study investigated changes in the magnitude of in vivo knee contact force achieved through a variety of gait modifications in a single subject with a force-measuring knee replacement. Two of the nine modified gait patterns significantly reduced medial contact force relative to normal gait (Fig. 2, Table 2), while lateral contact force was significantly reduced by five of the nine modified gait patterns (Fig. 3, Table 3). Walking with long hiking poles and wide pole placement consistently reduced both medial and lateral contact force over stance phase. This result suggests that walking with long hiking poles and wide pole placement reduces medial and lateral compartment knee loading and may be a safe way for individuals with medial knee OA to exercise.
Consistent with a previous study,11 walking with hiking poles was the most effective gait modification for reducing both medial and lateral contact force. Hiking pole gait has been suggested to reduce knee contact force by transferring some of the ground reaction force through the walking pole11,19 and by reducing the external knee adduction moment.12 Post-hoc statistical testing showed that the vertical ground reaction force was significantly reduced compared to normal gait at 75% of stance phase for three hiking pole conditions: long hiking poles with normal and wide pole placement and short hiking poles with wide pole placement. Thus, these findings suggest that hiking pole gait is effective in offloading the knee joint in part by transferring a portion of the ground reaction force through the arms instead of the legs. The changes in contact forces during hiking pole gait may have resulted from other factors, such as increased arm swing or the position of the arms relative to the body. Future studies should investigate if increased arm swing or alternative arm positioning may contribute to changes in knee joint loading. By utilizing an optimal hiking pole configuration (long hiking poles and wide pole placement), the effectiveness of hiking pole gait may be further enhanced.
Despite its general effectiveness, hiking pole gait was ineffective at reducing medial or lateral contact force in early stance, when contact forces are generally the highest in magnitude (Figs. 2 and 3, Tables 2 and 3). This result is in contrast to a previous study that reported significant reductions in medial contact force in early stance during hiking pole gait.11 A possible explanation for this result is that the ipsilateral hiking pole was placed on the ground slightly after, rather than coincident with, contralateral heel strike. To investigate this possibility, we performed a post-hoc analysis. The motion of reflective markers placed on the hiking poles during data collection as recorded with an 8-camera motion capture system (Vicon, Oxford Metrics Group, Oxford, UK) was used to determine the instant of pole strike with the ground. The hiking poles struck the ground on average at 8%, 10%, 11% and 7% of stance phase for short poles with normal pole placement, long poles with normal pole placement, short poles with wide pole placement, and long poles with wide pole placement, respectively. The delay in pole strike relative to heel strike likely reduced the effectiveness of the hiking poles in early stance. This quantitative finding is consistent with qualitative observations that the subject generally planted the ipsilateral pole after contralateral heel strike, possibly due to difficulty with trying to achieve the specified normal or wide pole placement. With sufficient practice and instruction, the individual in this study may be able to achieve contralateral pole strike coincident with ipsilateral heel strike and, therefore, may be able to reduce in vivo knee contact force during early stance.
Both mild and moderate crouch gait patterns significantly reduced lateral contact force at times during stance phase (Fig. 3, Table 3). However, both crouch gait modifications also increased medial contact force (Fig. 2, Table 2), although the increases were not statistically significant. For mild crouch gait at 25% of stance phase, knee contact force was transferred from the lateral compartment to the medial compartment and total contact force increased relative to normal gait. A similar lateral-to-medial transfer was observed for moderate crouch in late stance, though total contact force was reduced slightly. These results from this single-patient study may have implications for patient populations who exhibit crouch gait, who may transfer knee joint loads from the lateral to the medial compartment. This transfer of contact force to the medial compartment may increase the risk of developing medial compartment knee OA. However, further investigation in a larger patient population is needed to understand fully the impact of crouch gait on knee joint loading.
From a statistical perspective, no other gait modifications were found to be effective at reducing medial or lateral contact force during stance phase (Figs. 2 and 3, Tables 2 and 3). Although the changes were not statistically significant, several gait modifications reduced medial or lateral contact force by greater than 10%, which may be clinically significant. Such reductions were observed for medial thrust gait, forefoot strike gait, and hiking pole gaits with short and long poles and normal pole placement at various time points during stance (Figs. 2-3, Tables 2-3). Medial thrust and forefoot strike gait achieved average medial contact force reductions of 14% and 9%, respectively, at 25% of stance phase. Further investigation of the medial thrust gait results revealed that during five of the ten stance phases analyzed, medial contact force at 25% of stance phase was reduced between 22% and 25% relative to normal gait. Similarly, for forefoot strike gait, medial contact force at 25% of stance phase was reduced between 12% and 21% during five of the ten stance phases analyzed. Thus, with further practice to reduce variability between trials, it is possible that these two gait modifications could be clinically beneficial by reducing the critical first peak of medial contact force. Unlike a previous study,11 medial thrust gait did not reduce medial contact force in late stance. This result is likely because the subject was instructed to medialize his knees without increasing knee flexion significantly, as recommended by a previous study,12 making knee medialization more difficult to achieve consistently during late stance. Long-term training and feedback have been shown to improve long-term performance of medial thrust gait13 and, therefore, may improve the effectiveness of medial thrust gait at consistently reducing in vivo medial contact forces.
While this study provides important insight into changes in medial and lateral contact force through gait modification, the results are based upon data from a single subject implanted with a cruciate-retaining total knee replacement. Therefore, the extent to which these results can be generalized to other individuals with healthy or implanted knees is unknown. Future work will investigate gait modifications performed by other subjects implanted with force-measuring knee replacements to understand more fully how gait modification changes knee joint loading. In addition, while it is commonly believed that excessive loading of the articular cartilage is a contributing factor to the development or progression of knee OA, other factors, such as the location of the loading or the repetitive nature of the loading may also contribute to the development or progression of knee OA.3 Therefore, while the results of this study examined the changes in the magnitude of the loads on the knee though gait modification, other factors may provide additional insight into the impact of gait modifications in patients with knee OA. Despite these limitations, this study’s analysis of in vivo knee contact force data still provides unique information about the effectiveness of various gait modifications.
The purpose of this study was to understand changes in in vivo knee joint contact forces produced by gait modification. Walking with hiking poles was found to be the most effective at reducing medial and lateral contact force during stance phase. An optimal hiking pole configuration (long poles and wide pole placement) reduced medial contact force by 18% and lateral contact force by 14% on average over the stance phase. However, walking with hiking poles was not effective at reducing the contact forces in early stance, when contact forces are generally the highest in magnitude. Thus, strategies to improve the effectiveness of hiking pole gait in early stance such as placing the hiking pole on the ground slightly before heel strike, may be needed to achieve reductions in contact forces in early stance. The results of this study may have implications for individuals with knee osteoarthritis who may consider using hiking poles during walking to reduce the magnitude of knee joint loading and minimize further damage to the articular surfaces of the knee.
Acknowledgments
This study was funded by NIH grants R01EB009351 and R21HD053490. None of the authors’ professional and financial affiliations are perceived to have biased the presentation.
References
- 1.Lawrence RC, Felson DT, Helmick CG, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the united states. Part ii Arthritis Rheum. 2008;58:26–35. doi: 10.1002/art.23176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wise BL, Niu J, Yang M, et al. Patterns of compartment involvement in tibiofemoral osteoarthritis in men and women and in caucasians and african americans: The multicenter osteoarthritis study. Arthritis Care Res. 2012 doi: 10.1002/acr.21606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Maly MR. Abnormal and cumulative loading in knee osteoarthritis. Curr Opin Rheumatol. 2008;20:547–552. doi: 10.1097/BOR.0b013e328307f58c. [DOI] [PubMed] [Google Scholar]
- 4.Guo M, Axe MJ, Manal K. The influence of foot progression angle on the knee adduction moment during walking and stair climbing in pain free individuals with knee osteoarthritis. Gait Posture. 2007;26:436–441. doi: 10.1016/j.gaitpost.2006.10.008. [DOI] [PubMed] [Google Scholar]
- 5.Hurwitz DE, Ryals AB, Case JP, et al. The knee adduction moment during gait in subjects with knee osteoarthritis is more closely correlated with static alignment than radiographic disease severity, toe out angle and pain. J Orthop Res. 2002;20:101–107. doi: 10.1016/S0736-0266(01)00081-X. [DOI] [PubMed] [Google Scholar]
- 6.Mündermann A, Dyrby CO, Hurwitz DE, et al. Potential strategies to reduce medial compartment loading in patients with knee osteoarthritis of varying severity: Reduced walking speed. Arthritis Rheum. 2004;50:1172–1178. doi: 10.1002/art.20132. [DOI] [PubMed] [Google Scholar]
- 7.Robbins SM, Maly MR. The effect of gait speed on the knee adduction moment depends on waveform summary measures. Gait Posture. 2009;30:543–546. doi: 10.1016/j.gaitpost.2009.08.236. [DOI] [PubMed] [Google Scholar]
- 8.Hunt MA, Birmingham TB, Bryant D, et al. Lateral trunk lean explains variation in dynamic knee joint load in patients with medial compartment knee osteoarthritis. Osteoarthritis Cartilage. 2008;16:591–599. doi: 10.1016/j.joca.2007.10.017. [DOI] [PubMed] [Google Scholar]
- 9.Hunt MA, Simic M, Hinman RS, et al. Feasibility of a gait retraining strategy for reducing knee joint loading: Increased trunk lean guided by real-time biofeedback. J Biomech. 2011;44:943–947. doi: 10.1016/j.jbiomech.2010.11.027. [DOI] [PubMed] [Google Scholar]
- 10.Mundermann A, Asay JL, Mundermann L, Andriacchi TP. Implications of increased medio-lateral trunk sway for ambulatory mechanics. J Biomech. 2008;41:165–170. doi: 10.1016/j.jbiomech.2007.07.001. [DOI] [PubMed] [Google Scholar]
- 11.Fregly BJ, D’Lima DD, Colwell CW. Effective gait patterns for offloading the medial compartment of the knee. J Orthop Res. 2009;27:1016–1021. doi: 10.1002/jor.20843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Walter JP, D’Lima DD, Colwell CW, Fregly BJ. Decreased knee adduction moment does not guarantee decreased medial contact force during gait. J Orthop Res. 2010;28:1348–1354. doi: 10.1002/jor.21142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Barrios JA, Crossley KM, Davis IS. Gait retraining to reduce the knee adduction moment through real-time visual feedback of dynamic knee alignment. J Biomech. 2010;43:2208–2213. doi: 10.1016/j.jbiomech.2010.03.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Zhao D, Banks SA, Mitchell KH, et al. Correlation between the knee adduction torque and medial contact force for a variety of gait patterns. J Orthop Res. 2007;25:789–797. doi: 10.1002/jor.20379. [DOI] [PubMed] [Google Scholar]
- 15.D’Lima DD, Townsend CP, Arms SW, et al. An implantable telemetry device to measure intra-articular tibial forces. J Biomech. 2005;38:299–304. doi: 10.1016/j.jbiomech.2004.02.011. [DOI] [PubMed] [Google Scholar]
- 16.Kirking B, Krevolin J, Townsend C, et al. A multiaxial force-sensing implantable tibial prosthesis. J Biomech. 2006;39:1744–1751. doi: 10.1016/j.jbiomech.2005.05.023. [DOI] [PubMed] [Google Scholar]
- 17.Heinlein B, Graichen F, Bender A, et al. Design, calibration and pre-clinical testing of an instrumented tibial tray. J Biomech. 2007;40(Suppl 1):S4–10. doi: 10.1016/j.jbiomech.2007.02.014. [DOI] [PubMed] [Google Scholar]
- 18.Fregly BJ, Besier TF, Lloyd DG, et al. Grand challenge competition to predict in vivo knee loads. J Orthop Res. 2012;30:503–513. doi: 10.1002/jor.22023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Willson J, Torry MR, Decker MJ, et al. Effects of walking poles on lower extremity gait mechanics. Med Sci Sports Exerc. 2001;33:142–147. doi: 10.1097/00005768-200101000-00021. [DOI] [PubMed] [Google Scholar]