

Abstract
Introduction
Developmental dysplasia of the hip (DDH) is the most frequent inborn deformity of the locomotor apparatus. Ultrasound screening is frequently used to identify DDH in view of the brevity of the preclinical period during which diagnosis is possible. Appropriate therapeutic intervention during this period can positively affects the evolution of the disorder.
Methods
An unselected population of 1158 Sardinian neonates underwent ultrasound examinations of both hips, and findings were classified according to the method described by Graf. Patients were assessed by means of retrospective analysis to reveal cases of congenital dislocation of the hip joint. All cases were classified and treatment outcomes determined.
Results
A total of 145 hips requiring treatment were observed in 122 children. Hip dysplasia and/or dislocation were diagnosed between the ages of 14 days and 3 months. One month after diagnosis ultrasound findings were normal in 94% of the infants with at least one hip classified as type 2a. The remaining 6% were classified as types 2b, 2c, D, and 3. All were treated with abduction splints, and normal hip development was observed after one or two months of treatment. Type 4 hips were referred to an orthopedic surgeon for specialist treatment.
Conclusions
When performed by skilled operators, ultrasonographic techniques are of considerable value in prescribing treatment for DDH. The satisfactory prognosis associated with early treatment of severe congenital dislocation of the hip joint underlines the advisability of scheduling routine hip screening programs to ensure early diagnosis and effective treatment of the disorder.
Keywords: Dysplasia of the hip, Ultrasound, Newborn, Screening, DDH
Sommario
Introduzione
La displasia evolutiva dell'anca (DDH) costituisce la deformità più frequente dell'apparato locomotore. Lo screening ecografico è la metodica più utilizzata nell'identificazione della DDH, considerando la brevità del periodo in cui la diagnosi è possibile prima della comparsa dei sintomi clinici. Un intervento terapeutico appropriato precoce può avere un effetto positivo in relazione all'evoluzione di tale patologia.
Metodi
L'esame ecografico, la sua valutazione, la classificazione e la tipizzazione delle anche sono stati effettuati secondo il metodo descritto dal Graf. I pazienti sono stati valutati per mezzo di un'analisi retrospettiva volta a identificare i casi di DDH. Tutti i casi sono stati classificati e in base a ciò si è deciso il tipo di trattamento da attuare.
Risultati
Complessivamente sono state osservate 145 anche in 122 bambini che presentavano un certo grado di displasia. L'età alla diagnosi variava da 14 a 90 giorni con una media di 52 giorni di vita. Un mese dopo la diagnosi ecografica le anche di tipo 2a, sia bilaterali che unilaterali, sono risultate normali nel 94%. Il restante 6% così come i tipi 2b, 2c, D e 3 sono stati trattati con un divaricatore e la guarigione completa è stata ottenuta dopo due mesi di trattamento. Il tipo 4 è stato monitorato esclusivamente da un chirurgo ortopedico per un trattamento specialistico.
Conclusioni
Una volta effettuata l'indagine ecografica da operatori esperti si può decidere il tipo di trattamento più adeguato. L'ottima prognosi osservata a seguito del trattamento iniziale della DDH sottolinea la necessità di eseguire uno screening dell'anca allo scopo di effettuare una diagnosi e un trattamento precoce in questa patologia.
Introduction
The term developmental dysplasia of the hip (DDH) is used to denote a range of abnormalities involving the shape and/or abduction of the infant hip [1]. When present at birth, the disorder is commonly known as congenital dislocation of the hip (CDH). However, the term developmental dysplasia better describes the evolving nature of the condition and stresses the need for close monitoring throughout childhood, adolescence, and even during adulthood. DDH represents the most frequent inborn deformity of the locomotor apparatus. Ultrasonographic techniques provide a more detailed visualization of anatomic features of the hip that are often not revealed by the radiographic examination [2]. It is an acknowledged fact that earlier treatment for hip dysplasia carries a higher probability of success [3,4]. Ideally, therefore, the condition should be diagnosed within the first six weeks of life. In recent years, the increasing use of ultrasound [5] has markedly changed the diagnostic approach to this disorder. Today, in fact, ultrasonography represents the method of choice for screening newborns for dysplasia of the hip during the first months of life [6].
The aim of the present study was to assess the role of ultrasound-based population screening for DDH in promoting early diagnosis and onset of treatment. We also evaluated the importance of risk-factor assessment and clinical assessment of hip stability in the early diagnosis of dislocation of the hip.
Materials and methods
From 1 January 2005 to 1 January 2006, ultrasonographic techniques were used in the screening of 1158 infants (586 males, 572 females) for CDH. All examinations were performed in the outpatient department of the Center for Prevention of Dysplasia of the Hip (CPDH) at the University of Cagliari. Most of the infants screened (69.8%) came from the nursery of San Giovanni di Dio Hospital or from the University of Cagliari's Neonatal Pathology Unit; 19% had been referred to the CPDH through the hospital call center, and the remaining 12% had been referred by local pediatricians. For the purposes of the present study, the Graf method [5–7] was used to classify the forms of hip dysplasia on the basis of their ultrasound features, as shown in Table 1.
Table 1.
The Graf classification of hip dysplasia (Graf et al. 2001).
| Type | Superior bone rim | Cartilaginous rim | Alpha angle | Beta angle |
|---|---|---|---|---|
| 1A Mature hip (all ages) | Sharp | Thin triangle covering the femoral head | >60° | <55° |
| 1B Mature hip (all ages) | Blunted | Wide base, short, covering the femoral head | >60° | >55° |
| 2A (+/−) (up to 1 month) | Rounded | Wide, covering the femoral head | 50°–59° | >55° |
| 2B (>12 weeks) | Rounded | Covering the femoral head | 50°–59° | >55° |
| 2C | Rounded/flattened | Borderline coverage | 43°–49° | <77° |
| D | Rounded/flattened | Compressed | 43°–49° | >77° |
| 3A | Flattened | Compressed cranially without structural alterations | <43° | >77° |
| 3B | Flattened | Compressed cranially with structural alterations | <43° | >77° |
| 4 | Flattened | Compressed caudally | Not measurable |
For each case, we recorded findings obtained at ultrasound examination, age at diagnosis, outcome of the Ortolani maneuver, and risk factors, which included positive family history (first-degree); breech presentation, oligohydramnios, premature birth, twinness, malposition in utero, malformations, maternal diabetes, and decreased hip abduction. Data were evaluated by means of retrospective analysis.
The ultrasound examination was carried out by two specialists in the CPDH using a Synergy Diasonic scanner equipped with a 7.5-MHz linear probe.
All ultrasound images obtained were assessed and classified according to the method described by Graf. Each examination was corroborated by at least one image (alpha and beta angles were measured using a protractor), and a written report was provided that included the following items:
-
1.
age of patient;
-
2.
description of structures examined (femoral head and cartilaginous head);
-
3.
CDH type;
-
4.
measurements obtained for alpha and beta angles;
-
5.
therapeutic requirements (need for monitoring, therapeutic advice).
Results
Of the 1158 newborns (2316 hips) who underwent ultrasonographic screening, 122 (86 females and 36 males) had one or both hips classified as type 2a or higher. Most of the 145 hips in this subgroup (122/145) were type 2a (+/−); the remaining 23 were type 2b (n = 2); type 2c (n = 9); type D (n = 6); type 3a (n = 5); or type 4 (n = 1) (Fig. 1). Fifty-one of the 122 affected newborns had right-hip involvement, 54 had left hip involvement, and the other 20 had bilateral involvement.
Fig. 1.
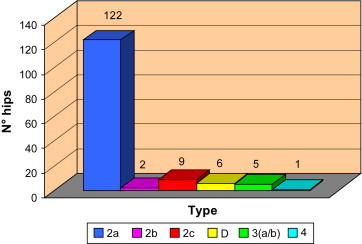
Distribution (according to the method described by Graf) of the 145 types of hips classified as type 1b or higher.
Three hundred sixty-four of the 1158 infants had at least one of the risk factors considered in the present study. Of the 122 patients with at least one hip that was type 2a or higher, 81 had no risk factors for CDH, 19 had histories of a breech presentation at the time of delivery or throughout pregnancy, 7 had first-degree relatives with CDH, 6 had histories of malposition in utero, 4 displayed decreased abduction, 3 were premature, 1 had malformations, and 1 had a diabetic mother. A positive Ortolani maneuver was observed in 2 cases; negative results were observed for the remaining hips (Fig. 2).
Fig. 2.

Distribution of risk factors in the 122 patients with at least one hip classified as type 2a or higher. No risk factors (NO RF); breech presentation or malposition in utero (BP), positive family history (F), reduced abduction (RA), prematurity (P), positive Ortolani maneuver (ORT), malformations (M), diabetic mother (FD).
The age at diagnosis ranged from 14 to 90 days with a mean age of 52 days. DDH was diagnosed before the age of 3 weeks in 31.6% of the infants and between the ages of 3 and 8 weeks in 68.4%. Treatment was begun at the time of diagnosis. One month after diagnosis, ultrasound studies revealed spontaneous evolution towards normal bone coverage in 94% of the Graf type 2a+/2a – hips (decreased bone coverage and alpha angles of 50°–59° diagnosed within the first three months of life). In the remaining cases (6%), bone coverage was achieved by means of soft retractor devices applied 24 h a day for a period of 30 days.
Type 2b hips were treated with a Milgram retractor. After 1 month of treatment, the ultrasound examination revealed a mature hip.
Types 2c, D, 3a and 3b were also treated with Milgram retractors, although in these cases the 1-month sonogram revealed incomplete recovery. All these hips showed complete recovery after two months' treatment.
Following ultrasound confirmation of the diagnosis, the single patient with a type 4 hip was monitored and referred to an orthopedic surgeon for treatment.
With regard to the follow-up, all patients with a hip classified as type 2a and higher underwent ultrasound monitoring and orthopedic examination every 30 days until complete recovery was achieved.
Immediately after application of the Milgram retractor, the correct position of the femoral head was verified with anterior and posterior radiographic examinations of the pelvis.
Discussion
The use of routine screening procedures for DDH is a subject of considerable ongoing debate. The high rates of spontaneous improvement reported for this condition (>80%) have led to considerable uncertainty regarding the approach to be used for screening positive infants. Recent reviews [8–10] have underlined the impossibility of evaluating the actual efficacy of screening on the basis of the results obtained, due to the lack of studies on spontaneous improvement of hip instability and on the functional outcomes of the treatments prescribed. These reviews emphasize the need for reliable proof of benefits afforded by screening procedures.
It has been argued that, compared with clinical examination (based on the Ortolani and Barlow maneuvers), ultrasound screening techniques lead to the identification of a higher number of cases of DDH, and that this can increase the risk of treatment being prescribed unnecessarily. However, the evolution of an uncomplicated case of dysplasia into coxarthrosis, or worse, into an untreated luxation of the hip, has considerable economic and social implications. Indeed, the cost of a mass screening program has to be analyzed in light of the economic burden represented by such cases – in terms of repeated, prolonged hospitalizations, surgery, residual disability, and rehabilitation programs. In Europe, this type of comparative analysis has revealed the advisability of performing mass ultrasound screening in young babies (<3 months) [11], whereas, to date authors in the United States have expressed a contrasting opinion [12].
The cases included in this study (which were observed between 1 January 2005 and 1 January 2006) were representative of an unselected sample of newborns.
Early diagnosis was achieved in 100% of the cases, during the first 2 weeks of life in 31.6%. On the average, the condition was diagnosed and treatment was started when the infant was 52 days old. The latter finding underlines the skill of physicians in identifying the disorder: pediatricians and neonatologists referred the newborns for ultrasound examination at an early age.
In recent years, early diagnosis of CDH in numerous areas has markedly reduced the need for traditional radiographic studies, but it has also led to diversification in the approaches used to manage this disorder and decreased the duration of treatment. It has also significantly decreased the use of surgery to treat late-diagnosed cases and the frequency of postoperative cephalic necrosis.
In the present study a total of 1154 infants (including 364 with at least one risk factor for CDH) were examined by means of ultrasonographic procedures [13]. Hip deficits were demonstrated in only 41 (3.6%) of these patients. Moreover, approximately 67% of the patients classified as type 2a or higher presented no risk factors: hip types (including type 4) were distributed equally.
The incidence of DDH we observed in Sardinia is higher than that reported in other Italian regions [2].
The findings obtained in the present study reveal how, in the majority of cases, the presence of risk factors per se is not particularly significant nor is it sufficient for early diagnosis of DDH. In particular, as previous reports have stressed [14], prematurity and twinness are no longer considered risk factors for this disorder.
For many years early screening for CDH in all parts of the world was based on the Ortolani [15] and Barlow [16] maneuvers. However, in recent years numerous publications have highlighted the shortcomings of this approach, which is based on the identification of an indirect functional sign rather than on morphological evaluation of the anatomopathological substrate underlying the disorder [17,18]. The Ortolani maneuver was positive in 2% of the patients examined in the present study, particularly those classified as types 3 and 4. It should be recalled, however, that the mean age of the infants evaluated in this study was 52 days. It is therefore possible that the maneuver would have elicited a positive result if the examination had been performed at an earlier date. When a newborn without risk factors and obtaining negative clinical findings, presents a positive clinical sign for hip dysplasia, late diagnosis will invariably ensue [19]. The aim, however, is to diagnose the disorder as early as possible [17]. Our experience shows that early treatment of CDH, made possible by ultrasound screening, can produce complete recovery of hip stability after one or two months of treatment. It is an acknowledged fact that type 4 hips are rarely observed at birth [16]. This indicates that the type 4 hip is frequently the outcome of a dysplastic process rather than a congenital disorder.
Early diagnosis of hip instability is fundamental in preventing the onset of DDH. Results obtained in patients treated to date corroborate the validity of the above statement. Indeed, the duration of treatment was shorter in patients treated at an early age (45 days), surgery was not required, and in all patients ultrasound findings provided evidence of normalization of clinical parameters. Moreover, all of the infants started to walk at the same mean age (12 months) as children without hip disorders.
Conclusions
To conclude, in terms of incidence, evolution, and difficulty of treatment, dysplasia of the hip constitutes one of the major orthopedic disorders. Over the last 20 years, the advent of ultrasonographic techniques has radically changed the prognosis of CDH, and today it rarely requires surgical treatment. Ultrasonography is the only procedure capable of identifying dysplastic and unstable hips at an early age, thus allowing timely treatment. To our knowledge, this is the first study of its kind published in the literature. Sardinia represents a special case since the region is characterized by genetic segregation and a high whole malformation of our region. Comparison of the results obtained in the present study with those published by De Pellegrin in 1979, 1985, 1989, and 1990 clearly shows that generalized screening at birth (1990) [17], regardless of the presence or absence of risk factors and/or clinical signs, is the only way to achieve early diagnosis rates of 100%. Therefore, the findings obtained by our group indicate that ultrasound screening should be extended to all newborn babies aged 4–6 weeks, even when clinical signs and risk factors for DDH are lacking, with the aim of enhancing early diagnosis and treatment of the disorder.
Declaration of competing interests
The authors declare that they have no competing interests.
References
- 1.Dezateux C., Rosendahl K. Developmental dysplasia of the hip. Lancet. 2007;5(369):1541–1552. doi: 10.1016/S0140-6736(07)60710-7. [DOI] [PubMed] [Google Scholar]
- 2.Baronciani D., Atti G., Andiloro F., Bartesaghi A., Gagliardi L., Passamonti L. Screening for developmental Dysplasia of the Hip: from theory to practice. Pediatrics. 1997;99(2):E5. doi: 10.1542/peds.99.2.e5. [DOI] [PubMed] [Google Scholar]
- 3.American Academy of Pediatrics Committee on quality improvement, subcommittee on Developmental Dysplasia of the Hip. Pediatrics. 2000;105:869–905. doi: 10.1542/peds.105.4.e57. [DOI] [PubMed] [Google Scholar]
- 4.Catteral A. The early diagnosis of congenital dislocation of the hip (editorial) J Bone Joint Surg Br. 1994;76:515–516. [PubMed] [Google Scholar]
- 5.Graf R. The diagnosis of congenital hip joint dislocation by the ultrasonic compound-treatment. Arch Orthop Traumat. 1980;97:117–133. doi: 10.1007/BF00450934. [DOI] [PubMed] [Google Scholar]
- 6.De Pellegrin M., Tessari L. Early ultrasound diagnosis of developmental dysplasia of the hip. Bull Hosp Joint Dis. 1996;54(4):222–225. [PubMed] [Google Scholar]
- 7.Graf R. George Thieme Verlag; Stuttgart-New York: 1987. Guide to sonography of the infant hip. [Google Scholar]
- 8.Woolacott N.F., Puhan M.A., Steurer J., Kleijnen J. Ultrasonography in screening for developmental dysplasia in newborns: systematic review. BMJ. 2005;330:1413. doi: 10.1136/bmj.38450.646088.E0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.US Preventive Services Task Force Screening for developmental dysplasia of the hip: recommendation statement. Am Fam Physician. 2006 Jun 1;73(11):1992–1996. [PubMed] [Google Scholar]
- 10.Shipman S.A., Helfand M., Moyer V., Yawn B.P. Screening for developmental dysplasia of the hip: a systematic literature review for the US Preventive Services Task Force. Pediatrics. 2006;117:557–576. doi: 10.1542/peds.2005-1597. [DOI] [PubMed] [Google Scholar]
- 11.Rosendahl K., Toma P. Ultrasound in the diagnosis of developmental dysplasia of the hip in newborns. The European approach. A review of methods, accuracy and clinical validity. Eur Radiol. 2008;17:1960–1967. doi: 10.1007/s00330-006-0557-y. [DOI] [PubMed] [Google Scholar]
- 12.Godward S., Dezateux C. Surgery for congenital dislocation of the hip in the UK as a measure of outcome of screening. Lancet. 1998;351:1149–1152. doi: 10.1016/s0140-6736(97)10466-4. [DOI] [PubMed] [Google Scholar]
- 13.Jari S., Paton S.W., Srinivasan M.S. Unilateral limitation of abduction of the hip: a valuable clinical sign for DDH? J Bone Joint Surg. 2002;84-B(1):104–107. doi: 10.1302/0301-620x.84b1.11418. [DOI] [PubMed] [Google Scholar]
- 14.Bielski R.J., Gesell M.W., Teng A.L., Cooper D.H., Muraskas J.K. Orthopaedic implications of multiple Gestation Pregnancy with triplets. J Pediat Orthop. 2006;26:129–131. doi: 10.1097/01.bpo.0000188998.13803.c1. [DOI] [PubMed] [Google Scholar]
- 15.Ortolani M. Un segno poco noto e la sua importanza per la diagnosi precoce di prelussazione congenita dell'anca. Pediatria. 1937;45:129–136. [Google Scholar]
- 16.Barlow T.G. Early diagnosis and treatment of congenital dislocation of the hip. J Bone Joint Surg Br. 1962;44:292–301. [Google Scholar]
- 17.De Pellegrin M. Ultrasound screening for congenital dislocation of the hip. Results and correlations between clinical ultrasound findings. Italian J Orthop and Traumatol. 1991;17:547–553. [PubMed] [Google Scholar]
- 18.Tonnis D., Storch K., Ulbrich H. Results of newborn screening for CDH with and without sonography and correlation of risk factors. J Pediatr Orthop. 1990;10(2):145–152. [PubMed] [Google Scholar]
- 19.Paton R.W., Hinduja K., Thomas C.D. The significance of at-risk factors in ultrasound surveillance of developmental dysplasia of the hip. J Bone Joint Surg. 2005;87-B(9):1264–1266. doi: 10.1302/0301-620X.87B9.16565. [DOI] [PubMed] [Google Scholar]