

Abstract
Swelling of the salivary glands occurring after injection of iodine based contrast agent is a rare late adverse reaction. Only a few cases in the literature report such diagnostic findings. We present our color Doppler ultrasound findings in a case of swelling of both submandibular glands occurring after administration of iodinated contrast agent.
Keywords: Iodine mumps, Ultrasound, Sialadenitis, Contrast media
Sommario
L'ingrandimento delle ghiandole salivari dopo iniezione di mezzo di contrasto iodato è una rara reazione avversa tardiva. In letteratura sono pochi i casi in cui vengono riportati i reperti diagnostici. In questo lavoro viene presentato un caso di tumefazione di entrambe le ghiandole sottomandibolari avvenuta dopo somministrazione di mezzo di contrasto iodato, studiato con esame eco-color-Doppler.
Introduction
Swelling of the salivary glands occurring after administration of iodinated contrast agent is a rare late adverse reaction which Anglo-Saxon authors call “iodide mumps” [1]. The cause of this reaction is unclear, but the most probable hypothesis is that it is caused by accumulation of iodide in the ductal system of the salivary glands with consequent inflammatory swelling of the glands. In this report we present ultrasound (US) findings obtained in a patient who presented swelling of both submandibular glands 18 h after administration of contrast agent in connection with a chest CT examination.
Presentation of the case
A 77-year-old woman underwent chest CT using contrast agent (120 mL Ultravist 370, 2.5 mL/s, Schering) because of a suspicious mass in the lung. Her biochemical values were not significantly altered (azotaemia 34 mg/dL, serum creatinine level 0.50 mg/dL and normal leucocyte formula). There were no immediate allergic reactions at the time of the examination.
About 18 h after the examination, the patient arrived at the Emergency Department because her neck was clearly swollen. Clinical examination revealed a painful swelling of both submandibular glands which felt solid on palpation.
US examination using a 10 MHz linear probe (Esaote, Genoa, Italy) showed significant swelling of both submandibular glands with lobular structures well-defined by hypoechoic septa (Fig. 1a) and surrounded by thin layers of peripheral fluid collection (Fig. 1b) and some dilated ducts (Fig. 2). Color Doppler US evaluation showed increased vascularity (Fig. 3) but this finding was not compatible with acute infectious sialadenitis as color-velocity based findings were normal. The parotid glands were not swollen. The patient was prescribed cortisone therapy: injections of 4 mg Bentelan (Sigma Tau) for 2 days. At follow-up examination after 48 h, clinical symptoms had substantially regressed and US findings were normal in both glands (Fig. 4). Ethical approval for this study was granted by the Medical Research Ethics Committee of our Institute, and informed consent was obtained from all patients.
Fig. 1.
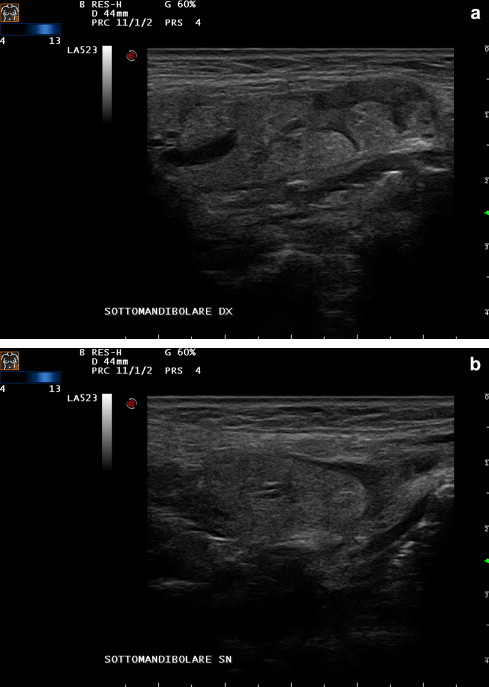
Swelling of the submandibular gland with the lobules of the gland defined by hypoechoic septa (a) and surrounded by peripheral fluid collection (b).
Fig. 2.

Swelling of the submandibular gland with distally dilated ducts.
Fig. 3.
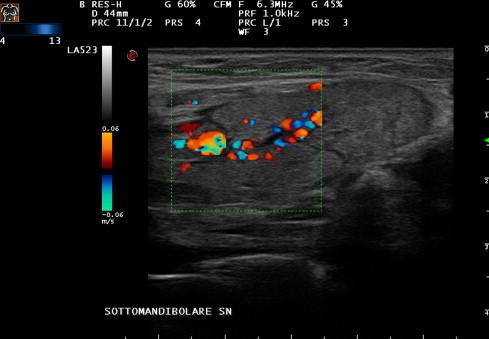
Color Doppler US shows enlarged vessels in the central portion of the gland.
Fig. 4.

Follow-up after 2 days shows regression of symptoms and normal echostructure of the gland.
Discussion
Iodide sialadenitis is referred to as a rare late reaction to intravascular administration of iodine containing contrast material leading to abnormal swelling of the salivary glands. Allergic reactions to the use of contrast agent are defined as late when onset is minimum 30 min after CT examination. In a prospective study, Yoshikawa reported 8% late reactions [2] while acute reactions are estimated to account for 3.8%.
Late reactions occur more often in women, in young patients and in patients with allergic diathesis causing mainly headache and rash. Use of low-osmolarity contrast agents reduces the incidence of adverse reactions, but the incidence of iodism, including iodide mumps, is the same for low and high osmolar contrast agents.
Ninety-eight percent of intravenously injected iodine is eliminated by the kidneys, and only 2% is excreted from other organs, such as salivary, sweat and lacrimal glands. The concentration of iodine in the parotid glands is 30 times higher than in the blood plasma and similar to the level found in the sweat, lacrimal and submandibular glands [3]. In normal subjects, the injected dose of contrast medium does not usually reach a sufficiently high iodide concentration to cause sialadenitis, whereas impaired renal excretion of contrast material may result in elevated concentrations of iodine and frequently lead to sialadenitis. The high concentration of iodine in the salivary secretion can induce oedematous swelling of the salivary ducts and lead to ductal obstruction with consequent inflammatory swelling of the salivary glands.
In the literature, some cases of swelling of the submandibular glands in patients with renal insufficiency are reported [4–6]. However, in the present case azotaemia and serum creatinine levels were normal, and the cause of this reaction was therefore unclear. US findings were diffuse swelling of the glands with prominent internal low echoic septa which evidenced the lobular structure without showing a significant increase in vascularity. The prognosis of this pathology is relatively benign. The onset varies from within a few minutes to up to 5 days after contrast medium administration. Associated adverse reactions are facial nerve paralysis, severe allergic vasculitis, skin erythema, enlargement of the thyroid as well as the lacrimal and salivary glands. The current management of iodine-induced sialadenitis is supportive therapy using analgesics and dialysis in cases of renal insufficiency. Although “iodide mumps” is a rare adverse reaction to the administration of contrast material, knowledge of the entity and ultrasound findings may facilitate the diagnosis in patients with neck swelling after administration of iodine containing contrast material.
Conflict of interest
The authors have no conflict of interest.
References
- 1.Berman H.L., Delaney V. Iodine mumps due to low osmolarity contrast material. AJR Am J Roentgenol. 1992;159:1099–1100. doi: 10.2214/ajr.159.5.1414783. [DOI] [PubMed] [Google Scholar]
- 2.Yoshikawa H. Late adverse reaction to non ionic contrast media. Radiology. 1992;183:737–740. doi: 10.1148/radiology.183.3.1584929. [DOI] [PubMed] [Google Scholar]
- 3.Kohri K., Miyoshi S., Nagahara A., Ohtani M. Bilateral parotid enlargement (“iodide mumps”) following excretory urography. Radiology. 1977;122:654. doi: 10.1148/122.3.654. [DOI] [PubMed] [Google Scholar]
- 4.Pavlica P., Derchi L.E., Barozzi L., Pasquali S. Acute enlargement of the submandibular glands following injection of nonionic contrast media. Study of a case with Doppler color ultrasonography. Radiol Med (Torino) 1996;92(3):326–328. [PubMed] [Google Scholar]
- 5.Park S.J., Hong H.S., Lee H.K., Joh J.H., Cha J.G., Kim H.C. Ultrasound findings of iodide mumps. Br J Radiol. 2005;78(926):164–165. doi: 10.1259/bjr/96432211. [DOI] [PubMed] [Google Scholar]
- 6.Acquaviva G., Galluzzo M., Millarelli S., Miele V., De Lillo M.L. Salivary glands swelling after the administration of a non-ionic iodized contrast medium. Acta Otorhinolaryngol Ital. 2000 Apr;20(2):125–128. [PubMed] [Google Scholar]