

LETTER
Recently, Geosentinel has been notified of patients with acute muscular Sarcocystis-like infections related to travel to Tioman Island, peninsular Malaysia (1). The outbreak started in the summer of 2011, and the initial patients were seen in Würzburg, Germany (2). The epidemic is currently ongoing, with a second wave of diseased travelers returning since the summer of 2012 (1). The organism responsible has not yet been properly characterized, but the clinical symptoms, laboratory parameters, and the histopathological characteristics shown in this report are highly compatible with a zoonotic Sarcocystis infection. Here we describe the initial cluster of patients and a muscle biopsy specimen showing this Sarcocystis-like infective agent for the first time.
In the period from 21 to 27 September 2011, 5 patients (3 males and 2 females; aged 31 to 32 years) were referred to the Department of Tropical Medicine, Medical Mission Hospital, Würzburg, Germany, with persisting severe myalgia after travel (Table 1). All had spent their vacation from 10 to 30 July 2011, in peninsular Malaysia with a stay on Tioman Island (July 20 to 29), 32 km off the east coast in the South China Sea (2° 48′ 47″ N, 104° 11′ 17″ E). A few days after returning home, all travelers, who belonged to a tourist group from southern Germany, had started suffering from a flu-like illness. Symptoms had commenced between August 1 and 8 with fatigue, headache, fever of 38 or 39°C, arthralgia (mild to moderate), and muscle pain (moderate to very severe) in the back and extremities. One patient suffered from watery diarrhea and urticarial rash 1 day before the onset of fever and later developed tachycardia, palpitations, and a recurring rash. Two patients reported that the pain had moved from the arms to the legs and then to the back from day to day, and one of these two patients had also developed a rash and cough. The pain was either increasing or persisting and located in the thighs, calves, upper arms, back, and in one patient also in the tongue. Electrocardiograms were unremarkable, except for one patient, who had an incomplete right bundle branch block and few ventricular extrasystoles. In all travelers, blood eosinophilia and elevated creatine kinase levels were noted, but trichinellosis and toxoplasmosis serologies were negative. A muscle biopsy specimen of the right anterior tibial muscle from one patient showed an oval structure filled with small protozoan cells surrounded by a very thin cyst lining located in a muscle cell (Fig. 1). The structure was compatible with a cyst of Sarcocystis sp. reported in Malaysia from human (3) and animal muscular tissue (4). Electron microscopy of the remaining tissue did not reveal any further parasitic cysts. PCR from the paraffin block for Toxoplasma gondii and Sarcocystis sp. were negative from two patients, possibly because of the formalin fixation or too few cysts present. On the basis of the clinical symptoms, laboratory data, and biopsy results, acute muscular sarcocystosis was suspected, and the local German health authorities, TropNet Europ, and Geosentinel were informed. All patients were treated with albendazole (400 mg twice a day [b.i.d.]) for 2 weeks and additional prednisone for 1 week (80, 40, and 20 mg per day in decreasing dosage) or 20 mg per day for 4 weeks. Treatment was well tolerated and led to improvement in 3 of the 4 travelers. One patient had to be treated twice, as symptoms relapsed after 4 weeks.
Table 1.
Patient characteristics and laboratory parameters at presentationa
| Patientb | Sex | Age (yr) | Result of muscle biopsy specimenc | % Eosinophilia (absolute no. in cells/μl) | IgE level (U/ml)d | Creatine kinase level (U/liter)e | CK-MB level (U/liter)f | Troponin I level (pg/ml)g |
|---|---|---|---|---|---|---|---|---|
| 1 | Female | 31 | ND | 10 (810) | 5 | 613 | 22 | 34 |
| 2 | Male | 31 | Mild myositis | 9 (890) | 25 | 1,127 | 27 | <3 |
| 3 | Male | 31 | ND | 23 (2,500) | 129 | 543 | 20 | 37 |
| 4 | Male | 31 | Parasitic cyst | 10 (820) | 200 | 630 | 14 | 12 |
| 5 | Female | 32 | ND | 8 (790) | 88 | 250 | 23 | 11 |
Patient characteristics and laboratory parameters when the patients went to the outpatient department in Würzburg, Germany, 21 to 27 September 2011.
Patients are numbered in the order they were seen in the outpatient department.
ND, not done.
The level for healthy individuals is <100 U/ml.
The level for healthy individuals is <171 U/liter.
CK-MB, creatine kinase isoform CK-MB (M for the muscle type subunit and B for the brain type subunit). The level for healthy individuals is <24 U/liter.
The level for healthy individuals is <14 pg/ml.
Fig 1.
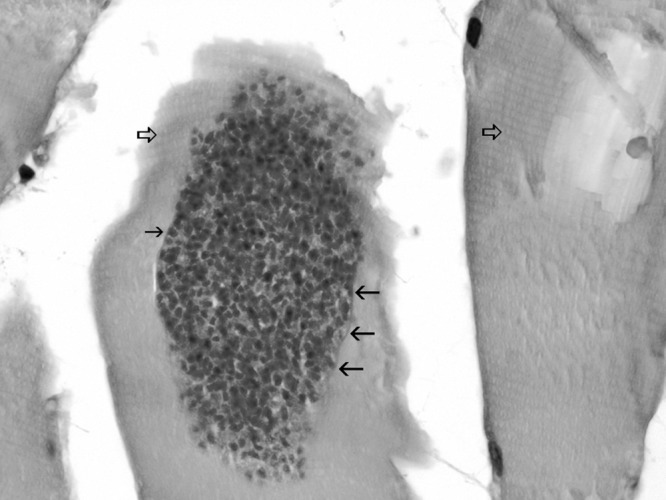
Muscle biopsy specimen from the right calf of a traveler who visited Tioman Island (patient 4) showing the Sarcocystis-like cyst filled with nucleated unicellular organisms inside a muscle cell in the center. The thin black arrows point to the faint cyst lining. The big empty arrows show the striation of the muscle cells. No inflammatory infiltrate is visible. This biopsy specimen was taken on 27 September 2011 (55 days after the onset of symptoms and 60 days after the patient returned from Tioman Island). The specimen was stained with hematoxylin and eosin. Original magnification, ×1,000.
Human muscular sarcocystosis is a zoonotic infection, with an unknown Sarcocystis sp. forming cysts in muscular tissue of the intermediate human host, and an unknown final host that harbors the apicomplexan parasites in the intestine (5). In 1991, sarcocystosis was already seen as a possible significant emerging food-borne zoonosis in Malaysia, as an overall seroprevalence of 19.8% was reported among the main racial groups (6), and 21% of autopsies showed sarcocysts (7). The first few cases in Malaysia were noted between 1975 and 1978 (8, 9), totaling to 11 cases by 1992 (10). The largest cluster of symptomatic muscular sarcocystosis was reported in 1999, affecting 7 U.S. servicemen working in a rural remote Malaysian village (5). In these patients, eosinophilia and muscle pain were also present, and sarcocysts were found in one patient.
The source of infection in Malaysia remains to be elucidated but seems to be persisting. Food or water contaminated with oocysts or sporocysts from feces of the animal host yet to be identified are the most likely origin of infection, and food and water should be properly cooked, washed, or obtained from a safe source. On Tioman Island, cats as well as macaques are abundant (1), and tourists should be aware of the risk of acquiring this infection.
Footnotes
Published ahead of print 5 December 2012
REFERENCES
- 1. Esposito DH, Freedman DO, Neumayr A, Parola P. 2012. Ongoing outbreak of an acute muscular Sarcocystis-like illness among travellers returning from Tioman Island, Malaysia, 2011–2012. Euro Surveill. 17(45):pii=20310. http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=20310 [PMC free article] [PubMed] [Google Scholar]
- 2. International Society for Infectious Diseases 21 October 2012. ProMED mail (Program for Monitoring Emerging Diseases). PRO/AH/EDR> Sarcocystosis, human—Malaysia (03): new cases, travel related. Archive no. 20111031.3240. International Society for Infectious Diseases, Brookline, MA [Google Scholar]
- 3. Wong KT, Clarke G, Pathmanathan R, Hamilton PW. 1994. Light microscopic and three-dimensional morphology of the human muscular sarcocyst. Parasitol. Res. 80:138–140 [DOI] [PubMed] [Google Scholar]
- 4. Latif B, Vellayan S, Omar E, Abdullah S, Mat Desa N. 2010. Sarcocystosis among wild captive and zoo animals in Malaysia. Korean J. Parasitol. 48:213–217 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Arness MK, Brown JD, Dubey JP, Neafie RC, Granstrom DE. 1999. An outbreak of acute eosinophilic myositis attributed to human Sarcocystis parasitism. Am. J. Trop. Med. Hyg. 61:548–553 [DOI] [PubMed] [Google Scholar]
- 6. Kan SP, Pathmanathan R. 1991. Review of sarcocystosis in Malaysia. Southeast Asian J. Trop. Med. Public Health 22(Suppl):129–134 [PubMed] [Google Scholar]
- 7. Wong KT, Pathmanathan R. 1992. High prevalence of human skeletal muscle sarcocystosis in south-east Asia. Trans. R. Soc. Trop. Med. Hyg. 86:631–632 [DOI] [PubMed] [Google Scholar]
- 8. Kutty MK, Dissanaike AS. 1975. A case of human Sarcocystis infection in west Malaysia. Trans. R. Soc. Trop. Med. Hyg. 69:503–504 [DOI] [PubMed] [Google Scholar]
- 9. Prathap K, Dissanaike AS. 1978. The fourth case of Sarcocystis infection in man in Malaysia. Southeast Asian J. Trop. Med. Public Health 9:452–453 [PubMed] [Google Scholar]
- 10. Pathmanathan R, Kan SP. 1992. Three cases of human Sarcocystis infection with a review of human muscular sarcocystosis in Malaysia. Trop. Geogr. Med. 44:102–108 [PubMed] [Google Scholar]