

Abstract
Context
Overhead athletes commonly have poor posture. Commercial braces are used to improve posture and function, but few researchers have examined the effects of shoulder or scapular bracing on posture and scapular muscle activity.
Objective
To examine whether a scapular stabilization brace acutely alters posture and scapular muscle activity in healthy overhead athletes with forward-head, rounded-shoulder posture (FHRSP).
Design
Randomized controlled clinical trial.
Setting
Applied biomechanics laboratory.
Patients or Other Participants
Thirty-eight healthy overhead athletes with FHRSP.
Intervention(s)
Participants were assigned randomly to 2 groups: compression shirt with no strap tension (S) and compression shirt with the straps fully tensioned (S + T). Posture was measured using lateral-view photography with retroreflective markers. Electromyography (EMG) of the upper trapezius (UT), middle trapezius (MT), lower trapezius (LT), and serratus anterior (SA) in the dominant upper extremity was measured during 4 exercises (scapular punches, W's, Y's, T's) and 2 glenohumeral motions (forward flexion, shoulder extension). Posture and exercise EMG measurements were taken with and without the brace applied.
Main Outcome Measure(s)
Head and shoulder angles were measured from lateral-view digital photographs. Normalized surface EMG was used to assess mean muscle activation of the UT, MT, LT, and SA.
Results
Application of the brace decreased forward shoulder angle in the S + T condition. Brace application also caused a small increase in LT EMG during forward flexion and Y's and a small decrease in UT and MT EMG during shoulder extension. Brace application in the S + T group decreased UT EMG during W's, whereas UT EMG increased during W's in the S group.
Conclusions
Application of the scapular brace improved shoulder posture and scapular muscle activity, but EMG changes were highly variable. Use of a scapular brace might improve shoulder posture and muscle activity in overhead athletes with poor posture.
Key Words: shoulder, upper extremity, electromyography, braces
Key Points
-
•
Changes occurred in forward shoulder angle and the electromyographic activity of the upper, middle, and lower trapezius muscles when participants wore the scapular-stabilizing brace.
-
•
The compression garment and the tension straps selectively affected posture by reducing forward shoulder angle, but associated electromyographic activity changes were small and do not appear to be influenced by strap tension.
-
•
Scapular bracing appeared to produce beneficial changes in muscular activity and posture in healthy overhead athletes.
-
•
Clinicians might consider using a scapular brace as an adjunct to prerehabilitation and rehabilitation exercises in the athlete with poor posture.
Shoulder injuries are a common and disabling condition among athletes, particularly overhead athletes (baseball, softball, swimming, volleyball, track and field throwing events, and tennis). Recent National Collegiate Athletic Association (NCAA) injury-surveillance system research has shown that shoulder injuries account for 39.4% of all injuries in baseball,1 15.8% of injuries in softball,2 and 21.7% of injuries in volleyball.3 Most of these injuries are classified as overuse injuries of muscles, tendons, and other tissues within the joint.4–7 These overuse injuries can result from incorrect posture, mechanics, or techniques during overhead throwing, hitting, or striking motions.8–10 Therefore, when working with athletes involved in overhead sports, clinicians should address posture, as well as sport-specific mechanics, during the evaluation and rehabilitation process.
Forward-head, rounded-shoulder posture (FHRSP) is a specific postural anomaly that might play a role in the development of shoulder pain and pathologic conditions. Both forward-head (FH) and rounded-shoulder (RS) postures are defined as excessive anterior orientation of the head or glenohumeral joint relative to the vertical plumb line of the body.8,11 These postural abnormalities often occur in conjunction and might be associated with other overuse injuries in the shoulder.11–14 Many clinicians and researchers8,14–16 believe that FHRSP alters scapular mechanics and muscular activity about the shoulder complex, causing altered force couples and scapular motions that result in tissue overuse, injury, and pain. Greenfield et al13 reported greater FH posture in patients with shoulder conditions than in healthy control participants. Griegel-Morris et al17 found an association between both FH and RS postures and reports of shoulder or scapular pain. Patients with preexisting FHRSP exhibited greater anterior tilt and upward rotation of the scapula during flexion motions at the shoulder.16 Acutely, adopting a FHRSP also creates increased scapular anterior tilt and upward rotation.18 Both of these specific scapular positions are related to shoulder conditions, suggesting that head and shoulder posture might influence the development and progression of overuse injuries.8,14,15
The altered positions of the scapula seen in individuals displaying FHRSP might change the electromyographic (EMG) activity of the musculature surrounding the scapula and glenohumeral joint, leading to tissue overload and injury. Patients with overuse shoulder conditions commonly display decreased serratus anterior (SA) and lower trapezius (LT) activity during shoulder motions.8,16,19–21 Most researchers8,14,15 believe that these altered EMG patterns disrupt the normal force couples surrounding the scapula, leading to dyskinesis and increasing the risk of pain. Researchers16,19,20 studying participants with FH, RS, or both, postures have demonstrated that these postures are related to decreased SA activity and increased upper trapezius (UT) activity. Given that these alterations in SA and UT activity have been observed in individuals with shoulder conditions, posture might play an important role in the development or progression of overuse shoulder injuries.21
One method for restoring normal posture and muscular activity around the scapula involves bracing or taping the scapulothoracic articulation. Scapular taping typically involves having the patient retract and depress the scapula, then applying tape over the scapular spine and medial border.11,22–25 The patients who have used scapular taping generally displayed altered scapular position, decreased UT muscle activity, and decreased or improved pain profiles.11,23–25 However, the application of adhesive tape might cause skin irritation in some patients and might not be a feasible intervention for daily or prolonged use. Based on the results of this research, companies have developed braces that patients can use to improve scapular position and muscle activity and treat shoulder conditions. These braces are designed to alter the posture of the shoulder and thoracic spine, causing favorable changes in scapular position, muscle activity, and movement . In studies of 15 healthy participants and 15 participants with scapular dyskinesis, Uhl et al26,27 found that wearing 1 type of commercially available scapular brace increased posterior tipping, decreased upward rotation in the dominant and nondominant upper extremities, and decreased internal rotation during the lowering phase of elevation. They concluded26,27 that the brace affected scapular position at rest and in the lower ranges of motion and might assist the scapular muscles in controlling scapular motion. Walther et al28 compared the effects of a functional brace with traditional rehabilitation and home-based programs in a group of participants with subacromial impingement syndrome. After 6 and 12 weeks, the braced group demonstrated the same improvements in shoulder pain and function as traditional rehabilitation groups. The authors28 concluded that bracing might be as effective as traditional methods for treating impingement syndrome. Thus, bracing might be a new tool to help correct scapular position and treat pain in individuals with shoulder conditions.
Scapular braces commonly are used for athletes with shoulder conditions in conjunction with rehabilitation. Clinically, athletic trainers might use bracing or taping to complement a corrective exercise program or might use bracing or taping to restore more normal length-tension relationships in muscles during the exercise program itself. Because of this, a better understanding of the effects these braces have on healthy individuals is needed. In the few studies of the effects of bracing or taping on the shoulder girdle, investigators have not examined short-term changes that take place during the performance of rehabilitative exercises, and no researchers have evaluated the effects of a brace application on factors such as scapular muscle activity and posture in healthy overhead athletes. Therefore, the purpose of our study was to examine whether a scapular stabilization brace acutely altered posture and scapular muscle activity in healthy overhead athletes with FHRSP while performing 4 common rehabilitation exercises and 2 functional shoulder movements compared with not wearing the brace.
METHODS
Participants
Ninety-three healthy participants were screened from the student population at the University of North Carolina at Chapel Hill, and 46 met the inclusion criteria to participate in our study. We examined 38 (men = 9, women = 29; age = 19.5 ± 1.2 years, mass = 75.4 ± 15.5 kg) of the 46 eligible participants. Descriptive statistics are presented in Table 1. The remaining 8 eligible individuals were not tested because of scheduling conflicts. An a priori power calculation using means from previous studies11,29 involving individuals with subacromial impingement syndrome revealed that 40 participants (20 participants per group) would be required for a power of .80. However, we ran our statistical analyses after 38 participants, and after examining the power of the results, we determined that testing 2 additional participants was unnecessary to achieve adequate power for this study.
Table 1.
Participant Demographics
| Characteristic |
Finding |
| Sex, n | |
| Men | 9 |
| Women | 29 |
| Age, mean ± SD, y | 19.5 ± 1.2 |
| Mass, mean ± SD, kg | 75.4 ± 15.5 |
| Hand dominance, n | |
| Right | 36 |
| Left | 2 |
| Sport, n | |
| Baseball | 1 |
| Softball | 6 |
| Swimming | 13 |
| Volleyball | 9 |
| Track throwers | 9 |
| Level of participation, n | |
| Varsity | 23 |
| Club | 11 |
| Recreational | 4 |
Participants were recruited through mass e-mails, flyers placed around campus, exercise and sports science classes, and the intercollegiate and club sporting groups. Volunteers were included if they were participating in an NCAA, club, or recreational overhead sport 3 to 4 days per week for 1 hour or more. An overhead sport was defined as baseball, softball, swimming, volleyball, tennis, or overhead events in track and field (javelin, shotput).30 Volunteers were excluded if they had injured their shoulders or back in the 6 months before the study, had histories of shoulder or back surgery, had scoliosis, were performing formal shoulder rehabilitation at the time of the study, had any congenital postural abnormalities, had FHRSP less than the criteria specified by Thigpen et al,16 or had any experience with the scapular brace. The dominant upper extremity, which was defined as the extremity with which the participant would throw a ball, was tested for each participant. Forward head angle (FHA) was defined as an FHA angle equal to or greater than 46° relative to the vertical line extending from C7 to the line connecting C7 to the tragus. Rounded shoulder position was described as having a forward shoulder angle (FSA) of equal to or greater than 46° relative to the vertical line extending from C7 to the line connecting C7 to the acromion (Figure 1).16
Figure 1. .
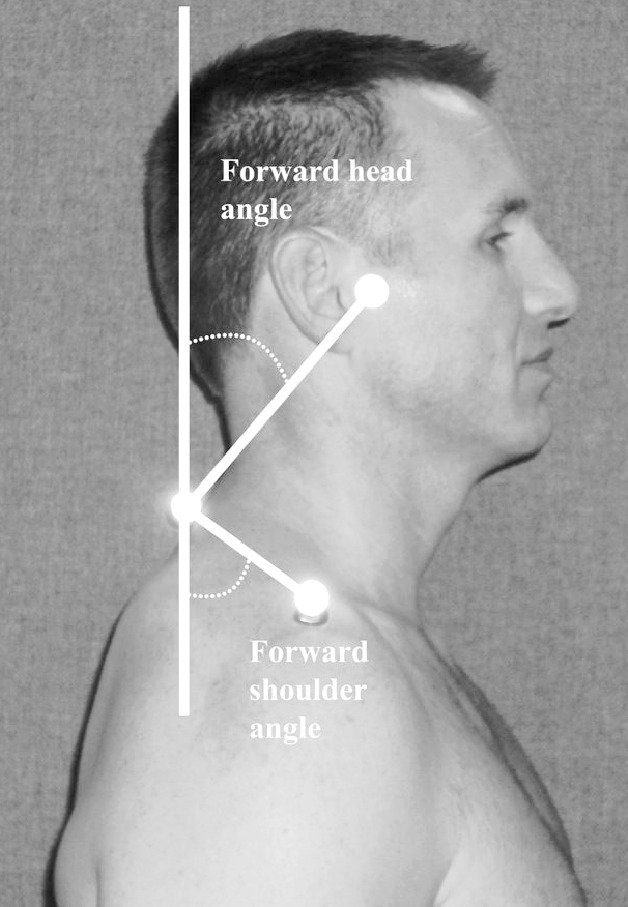
Method of calculating forward head rounded shoulder posture. Forward head angle was determined by measuring the angle between a line drawn from the tragus to the C7 spinous process and a vertical plumb line through C7. Forward shoulder angle was determined by measuring the angle between a line drawn from the tip of the acromion process to the C7 spinous process and a vertical plumb line through C7.
All participants provided written informed consent, and the study was approved by the University of North Carolina at Chapel Hill Biomedical Institutional Review Board.
Equipment and Materials
Posture
Reflective markers (Biotonix, Inc, Montreal, Quebec, Canada) and a 5.0-megapixel digital camera (Powershot A95; Canon, Lake Success, NY) were used to assess posture. Adobe Photoshop (version 7.0; Adobe, San Jose, CA) was used to calculate FHA and FSA (Figure 1).
Electromyography
The Bagnoli 8-channel hard-wired EMG system (Delsys Inc, Boston, MA) was used with differential amplification, common mode rejection ratio greater than 80 dB, input impedance greater than 1015//0.2 Ω//pF, and signal-to-noise ratio greater than 40 dB using an 8-channel amplifier. The EMG signal was amplified by a factor of 1000 over a bandwidth of 0.01 to 2000 Hz that was passed via an analog-to-digital converter (National Instruments, Austin, TX) sampling at 1000 Hz and corrected for direct-current bias. Raw EMG data were collected using the Motion Monitor (Innovative Sports Training Inc, Chicago, IL) software. Surface EMG reliability has been described in previous studies.31,32
Motion Analysis
The Motion Star (Ascension Technologies, Inc, Burlington, VT) electromagnetic motion-analysis system was used to determine the onset of each repetition during the exercises. This was used to ensure that the same motion was performed during each exercise under the brace and no-brace conditions. Positional data were collected using the Motion Monitor capture system and sampled at 50 Hz. Position error has been reported to be 3.3 mm, and orientation error has been reported to be 0.57°.33
Scapular Brace
We used the commercially available Spine and Scapula Stabilizing (S3) brace (Alignmed, Santa Ana, CA) (Figures 2 and 3).
Figure 2. .
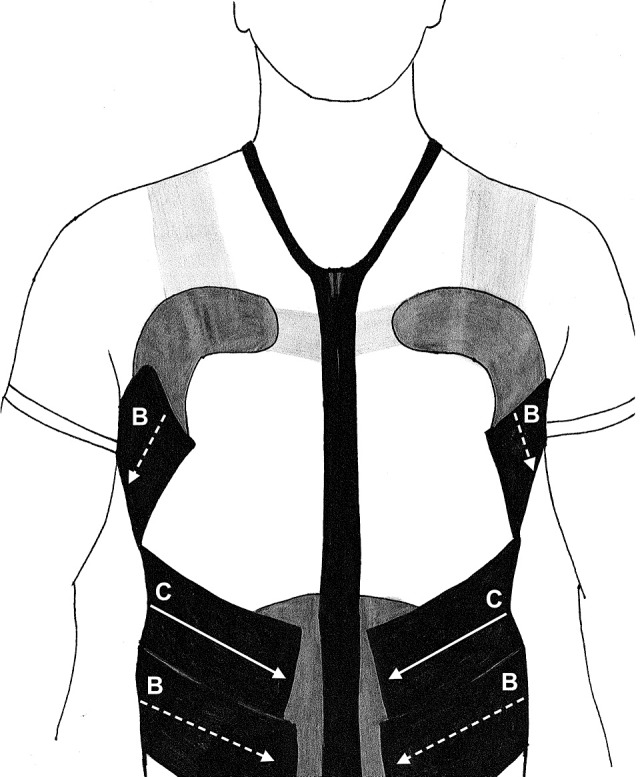
Scapular brace. The Spine and Scapula Stabilizing brace (Alignmed, Santa Ana, CA) consists of a compression shirt with a front zipper and hook-and-loop attachment sites and elastic straps that can be attached to the hook-and-loop pads. The placement of the B and C straps is labeled and represents the straps used in the compression shirt with fully tensioned straps condition. The C straps run from the scapular pads, cross at the midthorax, and terminate at the waist (indicated with solid arrows). The B straps run from the pectoral pads, cross at the lumbar spine, and terminate at the waist (indicated with dashed arrows).
Figure 3. .
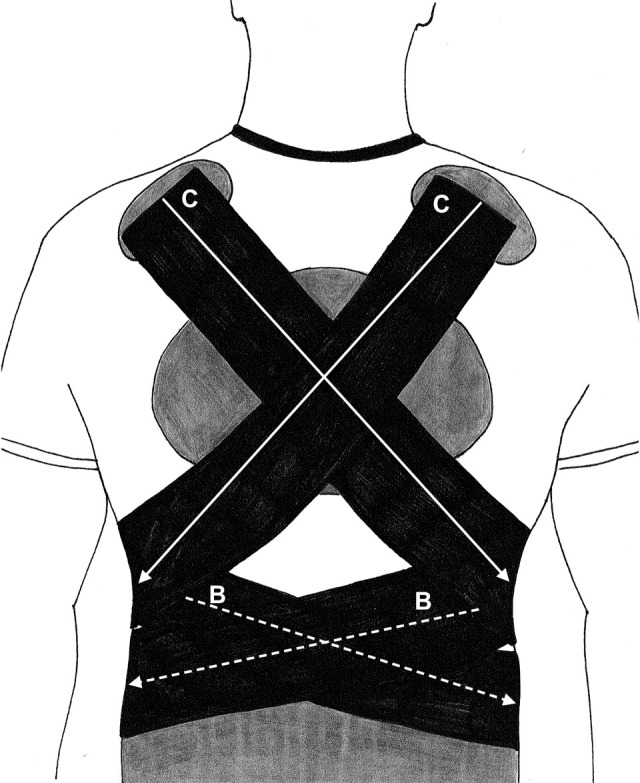
The strap configuration used in the fully tensioned straps condition (S+T) and one of the recommended strap configurations by the manufacturer of the Spine and Scapula Stabilizing brace (Alignmed, Santa Ana, CA). The C straps run from the scapular pads, cross at the midthorax, and terminate at the waist (indicated with solid arrows). The B straps run from the pectoral pads, cross at the lumbar spine, and terminate at the waist (indicated with dashed arrows).
Testing Procedures
Screening
Participants entered the sports medicine research laboratory for a 10-minute posture-screening session before testing began. Sagittal-plane photographs were taken to determine the presence of FHRSP. Calculations of the shoulder and head angles were performed to determine whether these volunteers met the inclusion criteria. Those who met the criteria for FHRSP and the previously mentioned inclusion criteria returned to the sports medicine research laboratory for the fitting and testing session.
Posture
Participants' FHRSPs were measured at 2 points during the testing session by the principal investigator (A.K.C.). The first photograph was taken before any other measures and without the brace applied, which was considered the no-brace condition. In the no-brace condition, participants were shirtless (men) or wore a sports bra (women). The second photograph was taken immediately after the brace was applied, which was described as the brace condition, using either the compression shirt with no strap tension (S) or the compression shirt with the straps fully tensioned (S + T) method as dictated by group assignment. Reflective markers were placed on the right tragus (ear), right acromion, and C7 vertebral spinous process.16 The locations of the retroreflective markers (Biotonix, Inc) were marked on the skin so that they were placed in identical locations for both photographs. Participants stood in a relaxed position, 40 cm in front of a grid, with their feet shoulder width apart. They were instructed to march in place 5 times, moving both the upper and lower extremities. Next, participants were instructed to look straight ahead in their natural resting positions. High-resolution digital pictures in the sagittal plane were taken from a tripod 3 m away from the grid. After the testing session ended, the photographs were uploaded onto a personal computer for postural analysis using Adobe Photoshop. Within-day posture measures using this method have demonstrated acceptable reliability for FHA (intraclass correlation coefficient [ICC] [2,1] = 0.92, SEM = 2°) and FSA (ICC [2,1] = 0.89, SEM = 5°).16
Electromyography
Electromyographic analyses were used to measure muscle activity of the SA, UT, LT, and middle trapezius (MT). The skin was prepared before EMG electrode placement by cleaning the area with alcohol to ensure good electrode contact and transmission. A bar Ag/AgCl single differential surface electrode (Delsys, Inc) was fixed onto the midpoint of each muscle belly so that the bars lay perpendicular to the muscle fibers. The electrodes were attached with adhesive stickers and secured with surgical tape. Electrode placements were based on published research:
-
1.
For the UT, the electrode was placed one-half the distance from the mastoid process to the root of the spine of the scapula, approximately at the angle of the neck and shoulder.16
-
2.
For the MT, it was placed midway along a horizontal line between the root of the spine of the scapula and the T3 spinous process.29,34
-
3.
For the LT, the electrode was placed 2 finger widths medial to the inferior angle of the scapula on a 45° angle toward T10.16
-
4.
For the SA, it was placed below the axilla and anterior to the latissimus dorsi over the fourth through sixth ribs and angled at 30° above the nipple line.16
-
5.
A common reference electrode was placed over the opposite acromion.16
Motion Analysis
After the EMG electrodes were placed on each participant, an electromagnetic receiver (the Motion Monitor) was placed on the posterior distal brachium to collect positional data.
Maximal Voluntary Isometric Contraction
After placing the EMG electrodes and the electromagnetic receiver on each participant, we assessed maximal voluntary isometric contraction (MVIC) using manual resistance to normalize EMG data. Participants performed 1 submaximal contraction to familiarize themselves with the manual muscle testing position. Participants performed three 5-second MVICs for each muscle, resting 1 minute between muscles and 30 seconds between trials. The average amplitude for all trials was recorded.
For the UT trial, the participant was seated with the upper extremities at his or her sides. The examiner (A.K.C.) stood behind the participant and instructed him or her to shrug the shoulder and rotate the head in the opposite direction. The examiner applied a stabilizing force to the back of the head with one hand and a downward force to the acromion for 5 seconds with the other hand. The participant then was instructed to relax.35
For the MT trial, the participant was in the prone position with the shoulder abducted to 90° and externally rotated. The examiner stood at the participant's side, instructed him or her to raise the extremity toward the ceiling, and applied a downward force to the proximal end of the brachium for 5 seconds. The participant then was instructed to relax.35
For the LT trial, the participant was positioned prone with his or her upper extremities raised overhead in line with the LT muscle fibers. The examiner stood at the participant's side, instructed him or her to raise the extremity toward the ceiling, and applied a downward force to the proximal end of the brachium for 5 seconds. The participant then was instructed to relax.35
For the SA trial, the participant was seated and instructed to sit up straight with the shoulder flexed between 120° and 130° and the upper extremity internally rotated. No support was provided to the participant's back. The examiner stood beside the participant, instructed him or her to raise the extremity toward the ceiling, and applied a downward force to the proximal end of the brachium for 5 seconds. The participant then was instructed to relax.35
Group Assignment and Counterbalancing
A counterbalancing procedure was used to determine group assignment (S, S + T) and the order of condition (brace, no brace). Nineteen cards with S written on them and 19 cards with S + T written on them were placed in a hat, drawn randomly by a secondary investigator (M.L.M.), and recorded in order on a master spreadsheet (eg, draw 1 = S, draw 2 = S + T, draw 3 = S + T). The first participant in the study was assigned the group from the first draw, the second participant was assigned the group from the second draw, and so on through participant 38. An identical procedure was used for order of condition (brace, no brace). Group assignment was concealed from the principal investigator. The use of S and S + T was considered the brace condition, whereas lack of any type of compression shirt or brace was considered the no-brace condition. The following procedures were performed on each participant under each testing condition.
Scapular Brace
The S3 brace was fitted and applied by 2 researchers (M.L.M. and S.E.H.) according to the manufacturer's specifications using a 2-strap method to blind the primary investigator to the participant's group assignment (Figure 2). The secondary researchers fit all participants for the correct size. The S + T group and the S group were not informed about the reasons for wearing the S3 brace. After putting on the S3 brace, both groups had the hook-and-loop pads tightened on the waistband so that they were snug but not uncomfortable. Both groups were instructed to retract and depress the shoulder blades in preparation for strap placement. The S + T group had a small (C) strap applied from the posterosuperior hook-and-loop pad, which was over the UT muscle, to the contralateral waistband. This method was repeated for the opposite side. Next, the medium (B) strap was attached from the lateral-superior hook-and-loop pad, which was over the pectoralis major muscle, to the contralateral waistband hook-and-loop pad inferior to the C strap. This method was repeated for the opposite side (Figure 3). The S group had the brace applied in the same method; however, the B straps were used in place of the C straps, and the long (A) straps were used in place of the B straps. A 5.5- to 6-in (14- to 15-cm) difference existed between the B and C straps and a 6-in (15-cm) difference existed between the A and B straps. Use of the longer straps prevented mechanical retraction from occurring at the shoulder girdle, allowing the investigators to examine the selective differences caused by strap tension. These longer straps also maintained the look of the brace, so that the primary investigator could maintain blinding to group assignment.
Exercises
All exercises were performed in randomized order. Participants drew numbers from a cup to determine exercise order. A device was constructed to provide consistency with the end point of the exercises as noted in Figures 4–9. The exercises performed were based on common clinical practice exercises and included scapular punches, W's, Y's, T's, forward flexion, and shoulder extension. These exercises also have been shown to produce high levels of EMG activation.36,37 A cuff weight was attached around each participant's wrist. The amount of weight used for scapular punches was 5% of the participant's body mass. The amount of weight used for each exercise was 1% of the participant's body mass for W's, Y's, T's, forward flexion, and shoulder extension. Participants were allowed to perform no more than 5 repetitions of each exercise as practice before data collection, when they performed 10 repetitions of each exercise using the dominant arm. A 1-minute rest period was allowed between exercises. A metronome was set at 60 beats per minute and was used to time each exercise.
Figure 4. .

Scapular punches in the no-brace condition.
Figure 9. .

Shoulder extension in the no-brace condition.
Scapular Punches
The participant lay supine on a table with his or her upper extremity in 90° of flexion. He or she protracted the scapula by raising the fist toward the ceiling while keeping the elbow straight (Figure 4).37
W's
The participant lay prone on the table with the upper extremities hanging down beside the table and the shoulder flexed to 90°. The upper extremity was raised so the brachium was parallel to the floor with the elbow bent to 90°. The extremity then was rotated externally to a comfortable end point (Figure 7).
Figure 7. .

W's in the no-brace condition.
Y's
The participant lay prone on a table with the upper extremities hanging down beside the table, shoulder flexed to 90°, and palms facing each other. The upper extremity was raised above the head with the extremity in line with the LT muscle fibers in the prone position.36 The upper extremity was flexed in the scapular plane to a terminal position of approximately 125° of abduction with the thumb raised toward the ceiling. The instruction given to the participant was, “Raise your arm like you are making a Y with your arm in a 10 o'clock or 2 o'clock position and keep your thumb pointed at the ceiling.” The upper extremity was raised until it was parallel to the floor (Figure 5).
Figure 5. .

Y's in the no-brace condition.
T's
The participant lay prone on a table with the upper extremity hanging down beside the table and shoulder flexed to 90°. The upper extremity was abducted horizontally until it was parallel to the floor (Figure 6).36
Figure 6.

T's in the no-brace condition.
Forward Flexion
The standing participant began the exercise with the upper extremity at 0° of flexion. The extremity was elevated with the forearm in a neutral position (thumb facing the ceiling) in the sagittal plane to full shoulder flexion (Figure 8).37
Figure 8. .
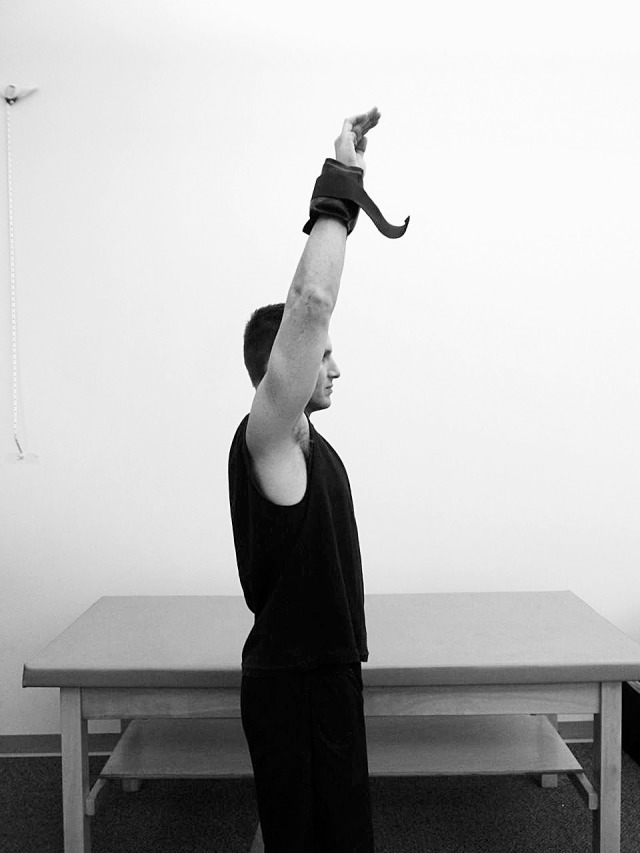
Forward flexion in the no-brace condition.
Shoulder Extension
The standing participant began the exercise with the upper extremity in 90° of flexion and the forearm in a neutral position (thumb facing the ceiling). The extremity was moved into full shoulder extension and back to 90° (Figure 9).37
Data Collection and Processing
All data were exported into a custom MATLAB program (The MathWorks, Inc, Natick, MA). Electromyography was rectified, band-pass filtered from 10 to 350 Hz, and smoothed via root mean square with a time constant of 15 milliseconds. Electromyography was normalized to the mean EMG amplitude obtained during the middle 1 second of the three 5-second MVIC trials. Mean normalized EMG amplitude was calculated across the entire movement (from the onset of movement to the end of that repetition). Onset of movement and end of the repetition were identified visually using the positional data from the electromagnetic motion-analysis system. The EMG amplitudes were averaged across all 10 trials for data analysis. Posture measurement and EMG values were imported into SPSS (version 14.0; SPSS Inc, Chicago, IL) for analysis.
Statistical Analyses
Means, SDs, and 95% confidence intervals (CIs) for each dependent variable were calculated by group (S, S + T) and condition (brace, no brace). The EMG data were screened for outliers, which were defined as values that were more than 3 SDs above or below the mean and were removed from statistical analysis. Twelve separate 2 × 2 mixed-model analyses of variance (ANOVAs) were used to analyze EMG activity during each of the exercise conditions. The between-subjects factor was group (S, S + T), and the within-subject factor was condition (brace, no brace). For EMG, data from all 4 muscles were compared during functional motions (shoulder flexion and extension). For the other 4 exercises, EMG was compared only for the muscle targeted by that specific exercise (UT, W's; MT, T's; LT, Y's; SA, punches). Two separate 2 × 2 mixed-model ANOVAs were used to analyze posture. The between-subjects factor was group (S, S + T), and the within-subject factor was condition (brace, no brace). Post hoc Bonferroni tests were used when an interaction was found. For statistical analyses, the α level was set a priori at .05. Effect sizes were calculated as partial η2 (η2p) and have been described as small (0.10), medium (0.25), and large (0.40).38 In addition, descriptive statistics (means, SDs, and 95% CIs) were calculated for the percentage change between the brace and no-brace conditions in each group for each dependent variable to observe the magnitude of change caused by brace application. Percentage change scores were calculated as (brace score − no-brace score)/no-brace score.
RESULTS
Means, SDs, and 95% CIs for each dependent variable are reported in Table 2. Descriptive data for percentage changes are reported in Table 3. A total of 14 EMG data points, which represented 0.7% of all EMG data points collected for this study, were identified as statistical outliers: 6 in the brace condition and 8 in the no-brace condition. No more than 2 outlier values were removed from any single comparison. In addition, 1 observation for FSA in the no-brace condition was removed because of measurement error.
Table 2.
Descriptive Statistics for Group and Condition
| Variable |
Group |
|||||||
| Compression Shirt Only |
Compression Shirt With Fully Tensioned Straps |
|||||||
| No Brace |
Brace |
No Brace |
Brace |
|||||
| Mean ± SD |
95% Confidence Interval |
Mean ± SD |
95% Confidence Interval |
Mean ± SD |
95% Confidence Interval |
Mean ± SD |
95% Confidence Interval |
|
| Forward head angle, ° | 48.6 ± 2.2 | 47.5, 49.6 | 47.9 ± 2.9 | 46.5, 49.3 | 47.3 ± 4.8 | 45.0, 49.6 | 46.6 ± 4.3 | 44.5, 48.6 |
| Forward shoulder angle, °a | 61.0 ± 8.2 | 57.0, 65.0 | 58.6 ± 10.0 | 53.8, 63.4 | 63.3 ± 8.6 | 59.0, 67.6 | 57.2 ± 7.3 | 53.7, 60.7 |
| Forward flexion | ||||||||
| Upper trapezius, % maximal voluntary isometric contraction | 41.9 ± 16.9 | 33.6, 50.3 | 44.0 ± 17.7 | 35.2, 52.8 | 55.4 ± 21.2 | 45.2, 65.6 | 51.6 ± 23.7 | 40.1, 63.0 |
| Middle trapezius, % maximal voluntary isometric contraction | 26.6 ± 13.1 | 20.0, 33.2 | 25.8 ± 14.4 | 18.7, 33.0 | 31.0 ± 18.4 | 22.2, 39.9 | 27.3 ± 10.4 | 22.1, 32.5 |
| Lower trapezius, % maximal voluntary isometric contractionb | 27.2 ± 13.5 | 20.4, 33.9 | 31.4 ± 15.1 | 24.1, 38.7 | 24.1 ± 11.0 | 18.8, 29.4 | 28.9 ± 12.8 | 22.8, 35.1 |
| Serratus anterior, % maximal voluntary isometric contraction | 49.1 ± 25.9 | 36.6, 61.6 | 48.8 ± 30.2 | 34.3, 63.4 | 46.0 ± 14.1 | 38.9, 53.0 | 46.7 ± 20.9 | 36.2, 57.1 |
| Shoulder extension | ||||||||
| Upper trapezius, % maximal voluntary isometric contractionc | 22.0 ± 10.8 | 16.8, 27.2 | 19.0 ± 8.9 | 14.7, 23.3 | 22.3 ± 9.3 | 17.8, 26.7 | 19.2 ± 7.2 | 15.6, 22.7 |
| Middle trapezius, % maximal voluntary isometric contractiond | 15.1 ± 5.5 | 12.5, 17.7 | 13.8 ± 6.0 | 10.9, 16.7 | 14.5 ± 5.9 | 11.6, 17.3 | 13.6 ± 5.6 | 10.9, 16.2 |
| Lower trapezius, % maximal voluntary isometric contraction | 24.5 ± 8.1 | 20.3, 28.7 | 28.5 ± 13.5 | 21.9, 35.0 | 18.7 ± 9.8 | 14.0, 23.4 | 21.2 ± 13.5 | 14.6, 27.7 |
| Serratus anterior, % maximal voluntary isometric contraction | 14.9 ± 8.9 | 10.6, 19.1 | 14.7 ± 8.8 | 10.5, 18.9 | 16.0 ± 8.1 | 12.0, 20.1 | 15.9 ± 6.9 | 12.5, 19.3 |
| W's (upper trapezius), % maximal voluntary isometric contractione | 40.9 ± 22.5 | 30.1, 51.8 | 45.1 ± 23.6 | 33.7, 56.4 | 45.8 ± 22.9 | 34.7, 56.8 | 39.0 ± 23.4 | 27.7, 50.2 |
| T's (middle trapezius), % maximal voluntary isometric contraction | 67.7 ± 18.6 | 58.7, 76.7 | 67.2 ± 19.5 | 57.8, 76.6 | 67.1 ± 26.6 | 53.9, 80.3 | 65.4 ± 23.3 | 54.2, 76.7 |
| Y's (lower trapezius), % maximal voluntary isometric contractionf | 64.5 ± 29.9 | 52.1, 82.2 | 67.1 ± 26.9 | 53.7, 80.4 | 60.5 ± 19.8 | 51.0, 70.1 | 69.4 ± 26.2 | 56.7, 82.0 |
| Serratus punch (serratus anterior), % maximal voluntary isometric contraction | 26.9 ± 9.9 | 22.2, 31.7 | 25.9 ± 13.0 | 19.6, 32.2 | 26.2 ± 11.1 | 20.9, 31.6 | 30.6 ± 14.8 | 23.5, 37.8 |
Indicates interaction effect for brace × group (P = .048). Forward shoulder angle was lower in the group with compression shirt with fully tensioned straps when the brace was applied.
Indicates main effect for brace (P = .001). Lower trapezius activity was higher when the brace was applied, regardless of method.
Indicates main effect for brace (P = .001). Upper trapezius activity was lower when the brace was applied, regardless of method.
Indicates main effect for brace (P = .01). Middle trapezius activity was lower when the brace was applied, regardless of method.
Indicates interaction effect for brace × group (P = .04). Upper trapezius activity was lower in the group with group compression shirt with fully tensioned straps when the brace was applied. Upper trapezius activity was higher in the group with compression shirt only when the brace was applied.
Indicates main effect for brace (P = .02). Lower trapezius activity was higher when the brace was applied, regardless of method.
Table 3.
Percentage Changes in Dependent Variables Due to Brace Applicationa,b
| Variable |
Group, Mean ± SD (95% Confidence Interval) |
|
| Compression Shirt Only |
Compression Shirt With Fully Tensioned Straps |
|
| Forward head angle | −1.4 ± 3.9 (−3.3, 0.4) | −1.3 ± 3.9 (−4.1, 1.5) |
| Forward shoulder angle | −3.7 ± 10.4 (−8.8, 1.2) | −9.4 ± 8.3 (−13.5, −5.2) |
| Forward flexion | ||
| Upper trapezius | 7.7 ± 33.9 (−9.1, 24.6) | −6.6 ± 18.7 (−15.6, 2.4) |
| Middle trapezius | 1.1 ± 57.4 (−27.5, 29.6) | 6.4 ± 18.7 (−15.8, 28.6) |
| Lower trapezius | 15.2 ± 35.5 (−2.4, 32.9) | 23.7 ± 23.2 (12.6, 34.9) |
| Serratus anterior | −2.5 ± 11.2 (−7.9, 2.9) | −1.7 ± 18.2 (−10.7, 7.3) |
| Shoulder extension | ||
| Upper trapezius | −9.6 ± 20.4 (−19.5, 0.2) | −10.4 ± 16.3 (−18.2, −2.5) |
| Middle trapezius | −10.2 ± 16.2 (−18.1, −2.4) | −4.6 ± 16.5 (−12.6, 3.3) |
| Lower trapezius | 5.1 ± 35.4 (−13.1, 23.3) | 10.9 ± 28.1 (−2.7, 24.4) |
| Serratus anterior | 1.9 ± 16.5 (−6.1, 9.8) | 4.3 ± 18.3 (−4.8, 13.4) |
| W's (upper trapezius) | 21.7 ± 58.3 (−6.4, 49.8) | −11.7 ± 29.0 (−25.7, 2.3) |
| T's (middle trapezius) | −0.3 ± 18.1 (−9.0, 8.5) | −1.1 ± 30.3 (−16.2, 14.0) |
| Y's (lower trapezius) | 7.6 ± 19.7 (−1.9, 17.1) | 16.5 ± 34.8 (−0.3, 33.2) |
| Serratus punch (serratus anterior) | 0.7 ± 35.9 (−16.6, 18.0) | 19.0 ± 38.4 (0.5, 37.5) |
Values given are percentage change from the no-brace condition.
Values are calculated as (brace value – no-brace value)/no-brace value. Negative numbers indicate that brace application caused a decline in value.
Posture
A brace × group interaction effect was found for FSA (F1,35 = 4.20, P = .048, η2p = 0.107, observed power = .513). Post hoc Bonferroni testing revealed a decrease in FSA for the S + T group after brace application (t17 = −5.42, P < .001). Brace application decreased FSA posture by 3.7% (95% CI = −8.8, 1.2) and 9.4% (95% CI = −13.5, −5.2) in the S and S + T groups, respectively. We found no group main effect for FSA (F1,35 = 0.02, P = .89). We noted a main effect for brace condition for FSA (F1,35 = 21.21, P < .001, η2p = 0.380, observed power = .994). We demonstrated no differences for FHA (F1,36 range = 0.005–3.356, all P values > .05). All observed effect sizes for the FHA comparisons were less than 0.10, suggesting that no meaningful differences existed in the findings.
Electromyography
Forward Flexion
We found a main effect for normalized EMG for the LT in the brace condition (F1,35 = 12.59, P = .001, η2p = 0.265, observed power = .932). Brace application increased LT EMG by 15.2% (95% CI = −2.4, 32.9) and 23.7% (95% CI = 12.6, 34.9) in the S and S + T groups, respectively. We found no group main effects or interaction effects for this exercise or other muscles (F range = <0.001–2.74, all P values > .05). All observed effect sizes for all other results that were not different were less than 0.10.
Shoulder Extension
We noted a main effect for normalized EMG shoulder extension for the UT in the brace condition (F1,36 = 14.51, P = .001, η2p = 0.287, observed power = .960). Brace application decreased UT EMG by 9.6% (95% CI = −19.5, 0.2) and 10.4% (95% CI = −18.2, −2.5) in the S and S + T groups, respectively. A main effect was found for normalized EMG for the MT in the brace condition (F1,36 = 7.34, P = .01, η2p = 0.169, observed power = .750). Brace application decreased MT EMG by 10.2% (95% CI = −18.1, −2.4) and 4.6% (95% CI = −12.6, 3.3) in the S and S + T groups, respectively. We demonstrated no other differences (F range, <0.001–2.233, all P values > .05). Effect sizes for results that were not different were less than 0.10.
W's
We found an interaction effect in UT EMG activity for brace × group (F1,36 = 4.71, P = .04, η2p = 0.116, observed power = .560). Post hoc testing revealed no differences. We saw no main effects for this exercise and muscle (F1,36 range = 0.008–0.283, all P values > .05). Effect sizes for results that were not different were less than 0.10, suggesting that no meaningful differences existed in these comparisons.
Y's
We noted a main effect for the LT for the brace condition (F1,35 = 5.59, P = .02, η2p = 0.138, observed power = .633). Brace application increased LT EMG by 7.6% (95% CI = −1.9, 17.1) and 16.5% (95% CI = −0.3, 33.2) in the S and S + T groups, respectively. Effect sizes for results that were not different were less than 0.10.
T's
We observed no main effects or interaction effects for this exercise (F1,35 range = 0.210–0.852, all P values > .05). Effect sizes for results that were not different were less than 0.10.
Scapular Punch
We found no main or interaction effects for this exercise (F1,36 range = 0.299–3.077, P > .05). Effect sizes for results that were not different were less than 0.10.
DISCUSSION
The purpose of our study was to determine whether a commercially available shoulder brace could improve posture and muscle activity of the scapular stabilizers in overhead athletes with FHRSP. Our results suggested that the brace changes FSA and alters some muscular activity during activity. The changes in posture were seen primarily as a change in FSA in the S + T group, but alterations in EMG amplitude were observed regardless of the tension or lack of tension on the elastic straps. This might suggest that the brace's effects on posture are a combination of mechanical alteration of joint alignment and enhanced proprioception, whereas the EMG changes largely are due to proprioceptive feedback. However, many of the changes in EMG were highly variable, with wide 95% CIs. Thus, most of the EMG results should be considered cautiously.
In our study, FSA was decreased when participants were wearing the brace compared with when they were not wearing the brace. Post hoc testing of the interaction demonstrated that this change was different in the S + T group but was not different in the S group. This matches our hypothesis and suggests that the properly tensioned straps created postural alterations that were different from those created by wearing the compression garment alone. The potential for taping or bracing to change FSA posture has been demonstrated using tape application to the skin surrounding the scapula. Lewis et al11 found that scapular taping caused a decrease in FSA, with change scores similar to those in our study. However, a placebo tape application did not create the same alterations in posture as the properly tensioned therapeutic tape application. The results suggest that simply providing cutaneous stimulation is not enough to alter resting posture and that the tension of the tape might mechanically influence FSA posture and enhance proprioception surrounding the shoulder girdle. Our results add to the theory that shoulder posture can be changed in the short term via brace application. The mechanism behind this change appears to be a combination of mechanical alterations of the position of the shoulder girdle (tensioned straps) and enhanced proprioceptive feedback from the brace. Researchers39–41 have demonstrated a consistent improvement in both active and passive joint repositioning sense with the application of compressive sleeves and garments similar to the compression shirt used in our study. They have proposed that proprioception can be enhanced markedly via the cutaneous feedback that compression garments provide. Our results add to the literature on altered proprioception and static posture via compression garments, sleeves, or tape applied to the shoulder and scapular region.
Although a change occurred in FSA with the brace application, no alteration occurred in FHA. Because the shirt and elastic straps are applied to the shoulder and scapular region, feedback to the cervical spine might be insufficient to alter this posture variable. Because proprioceptive and cutaneous stimulation appear to be reasons for the changes observed in FSA, the lack of any compression or tactile feedback on the cervical spine might partially explain the results. However, Lewis et al11 found that scapular taping did improve FHA compared with placebo taping, despite no tape application to the cervical spine. The effects on FHA were similar to the changes in FSA described above and were far greater than the changes seen in our study. Whereas differences in participant demographics might help explain some of these differences (substantial FHRSP was required for our study but was not an inclusion criterion for Lewis et al11), inherent differences also might exist between tensioned tape applied to the skin and a compressive shirt. As applied by Lewis et al,11 the tape likely exerted a specific targeted cutaneous feedback from the scapular region. The compression shirt worn in our study provided more global feedback bilaterally from the entire shoulder girdle; thus, the effects on FHA might not have been as pronounced. Although definitive conclusions cannot be drawn from a single study, our results indicate that bracing might not be as effective as taping for the alteration of FHA.
Bracing might cause minor but desirable changes in muscle activation amplitude during shoulder exercises and functional movements. The changes in EMG amplitude were small, and although they were statistically different, their clinical importance is debatable. However, the observed changes were largely in the hypothesized direction and might be considered beneficial for athletes with shoulder conditions, particularly impingement syndrome.
The brace application slightly increased LT EMG amplitude during forward shoulder flexion and decreased MT and UT EMG amplitude during shoulder extension. Yet whether the straps were tensioned had no influence over these results. Again, this suggests a sensory or proprioceptive influence over muscle activation simply because of the compression of the brace on the shoulder girdle, in addition to any small changes due to altered scapulothoracic position. These results are in agreement with those of Selkowitz et al,25 who reported that scapular taping in patients with suspected impingement resulted in decreased UT amplitude and increased LT amplitude during reaching tasks. In their Kinesio Taping study, Hsu et al23 also found EMG amplitude changes with the application of tape regardless of tension, but the direction of change was different for some of the EMG variables tested. When evaluating EMG in relation to shoulder conditions, researchers14,15 have suggested that increased UT EMG amplitude, particularly in the presence of an underactive or weak LT, disrupts the normal force couple that guides the scapula during shoulder motion. Ultimately, these changes might lead to chronic shoulder conditions, such as subacromial impingement, associated subacromial bursitis, and rotator cuff or biceps tendinitis.9 Although our results showed that UT activity decreased while LT activity increased, the magnitude of these changes was only moderate (effect sizes = 0.287 and 0.265, respectively), and the variability of the percentage change was extremely high. This partially is due to inherent variability seen with surface EMG measurements and also to a wide range of responses from our participants in each group. Therefore, the findings that were different might have limited clinical application at this time. However, our results provide preliminary support for the potential use of a brace or compression garment to help correct these force couples in individuals who have poor posture and might be at risk of developing shoulder conditions.
The finding that UT EMG amplitude when performing the W's exercise increased during the S condition but decreased during the S + T condition was intriguing but lacked sufficient statistical power to find post hoc differences between groups and conditions. It was the only result with an interaction for the EMG data in different brace application conditions, and this interaction closely matched the interaction for the FSA. Thus, the changes in shoulder posture might have had a direct effect on UT EMG activity. Wearing the brace with tensioned straps reduced UT amplitude by 11.7%, whereas wearing the brace with untensioned straps actually increased UT amplitude by 21.7%. However, the 95% CIs for these percentage change scores were extremely wide, particularly for the untensioned straps. If a goal of rehabilitation is to reduce UT muscle activity to restore normal force couples in individuals with poor posture, a scapular brace might help augment targeted exercises for the shoulder. However, given the variation in the data, these responses might be influenced by several other factors that were not controlled in this study, including the influence of upper extremity dominance, specific training patterns, vestibular contributions, and participant-specific alterations in the fit of the brace. In the future, researchers should attempt to investigate these findings further, particularly in a group of participants with shoulder conditions.
Based on our findings, wearing a scapular-stabilizing brace appears to have caused positive changes in forward shoulder posture and EMG amplitude of the UT and LT. The changes in FSA posture likely were due to a combination of mechanical and proprioceptive changes, the compression garment, and the tension provided by the straps. The changes in EMG appeared to be associated more closely with simply wearing the compression garment, but our conclusions are somewhat weakened by the wide CIs and small to moderate effect sizes. The relative complexity of the scapulothoracic articulation might make actual mechanical alterations of scapular position and muscle activity more difficult and variable. Although we make no definitive recommendations based on this single study, the accumulating body of literature does suggest some benefit when using bracing or taping to alter scapular motion, muscle activation, and posture in both symptomatic and at-risk patient populations (eg, overhead athletes, patients with poor posture).11,22,23,25–27,41 Given the publication of randomized clinical trials24,28 in which the authors found that scapular taping and bracing does assist in recovery after impingement syndromes, bracing might be a useful method for improving patient outcomes during rehabilitation. In the future, researchers should continue to examine the differential improvement due to mechanical braces (tensioned straps) versus tactile feedback braces (compression sleeves or garments, padding) and the potential differences in strap placement and application.
One important limitation of this study was the variable fit of the scapular brace on each participant. Braces were provided in 6 sizes to fit the participants, and the investigators (M.L.M. and S.E.H.) involved in the application of the braces were trained by a representative from the manufacturer on how to fit each brace for each participant. However, the material of the compression top often gathered during movement, and participants with short torsos had more difficulty with fit than did other participants. The width of the shoulder region was also a concern for the female participants. This might have limited the ability to show differences in some of the variables and also will influence the efficacy of the bracing during clinical applications.
Another limitation was that 1 type of brace application was used. Different brace applications might affect posture and EMG differently, and using a different method might be more beneficial. Whereas the participants all had FHRSP, they were asymptomatic and had no history of major shoulder condition, which limits the ability to draw conclusions about how bracing might affect the treatment of pain or pathologic conditions. Variability in EMG variables was apparent from large SDs of the mean and wide CIs, which are common limitations when using EMG. Although the investigators tried to make a conscious effort to avoid additional compression over the EMG electrodes when applying the hook-and-loop pads, compression might have occurred and caused unknown alterations in EMG. In addition, although the a priori power analysis recommended a sample size of 40, there appeared to be a lack of power to detect differences on some variables. Finally, although every effort was made to blind the participants and the primary investigator to ensure the validity of the results, we cannot rule out that the participants might have altered their posture and muscle activity simply because of research participation.
CONCLUSIONS
We found changes in FSA and UT, MT, and LT EMG activity when participants wore the scapular-stabilizing brace. Posture was affected selectively by both the compression garment and the tension of the straps, producing a reduction in FSA. However, the EMG results demonstrated small changes that were largely equivalent between the 2 groups, suggesting some proprioceptive or sensory mechanism for the changes we observed. Scapular bracing appears to produce beneficial changes in muscle activity and posture in healthy overhead athletes. Clinicians might want to consider the potential benefit of brace use as an adjunct to prerehabilitation and rehabilitation exercises.
REFERENCES
- 1.Dick R, Sauers EL, Agel J et al. Descriptive epidemiology of collegiate men's baseball injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):183–193. [PMC free article] [PubMed] [Google Scholar]
- 2.Marshall SW, Hamstra-Wright KL, Dick R, Grove KA, Agel J. Descriptive epidemiology of collegiate women's softball injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):286–294. [PMC free article] [PubMed] [Google Scholar]
- 3.Agel J, Palmieri-Smith RM, Dick R, Wojtys EM, Marshall SW. Descriptive epidemiology of collegiate women's volleyball injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):295–302. [PMC free article] [PubMed] [Google Scholar]
- 4.Hill JL, Humphries B, Weidner T, Newton RU. Female collegiate windmill pitchers: influences to injury incidence. J Strength Cond Res. 2004;18(3):426–431. doi: 10.1519/1533-4287(2004)18<426:FCWPIT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 5.Wang HK, Cochrane T. A descriptive epidemiological study of shoulder injury in top level English male volleyball players. Int J Sports Med. 2001;22(2):159–163. doi: 10.1055/s-2001-11346. [DOI] [PubMed] [Google Scholar]
- 6.Aagaard H, Jorgensen U. Injuries in elite volleyball. Scand J Med Sci Sports. 1996;6(4):228–232. doi: 10.1111/j.1600-0838.1996.tb00096.x. [DOI] [PubMed] [Google Scholar]
- 7.McFarland EG, Wasik M. Epidemiology of collegiate baseball injuries. Clin J Sport Med. 1998;8(1):10–13. doi: 10.1097/00042752-199801000-00003. [DOI] [PubMed] [Google Scholar]
- 8.Lewis JS, Green A, Wright C. Subacromial impingement syndrome: the role of posture and muscle imbalance. J Shoulder Elbow Surg. 2005;14(4):385–392. doi: 10.1016/j.jse.2004.08.007. [DOI] [PubMed] [Google Scholar]
- 9.Ludewig PM, Hoff MS, Osowski EE, Meschke SA, Rundquist PJ. Relative balance of serratus anterior and upper trapezius muscle activity during push-up exercises. Am J Sports Med. 2004;32(2):484–493. doi: 10.1177/0363546503258911. [DOI] [PubMed] [Google Scholar]
- 10.Voight ML, Thomson BC. The role of the scapula in the rehabilitation of shoulder injuries. J Athl Train. 2000;35(3):364–372. [PMC free article] [PubMed] [Google Scholar]
- 11.Lewis JS, Wright C, Green A. Subacromial impingement syndrome: the effect of changing posture on shoulder range of movement. J Orthop Sports Phys Ther. 2005;35(2):72–87. doi: 10.2519/jospt.2005.35.2.72. [DOI] [PubMed] [Google Scholar]
- 12.Fu FH, Harner CD, Klein AH. Shoulder impingement syndrome: a critical review. Clin Orthop Relat Res. 1991;269:162–173. [PubMed] [Google Scholar]
- 13.Greenfield B, Catlin PA, Coats PW, Green E, McDonald JJ, North C. Posture in patients with shoulder overuse injuries and healthy individuals. J Orthop Sports Phys Ther. 1995;21(5):287–295. doi: 10.2519/jospt.1995.21.5.287. [DOI] [PubMed] [Google Scholar]
- 14.Michener LA, McClure PW, Karduna AR. Anatomical and biomechanical mechanisms of subacromial impingement syndrome. Clin Biomech (Bristol, Avon) 2003;18(5):369–379. doi: 10.1016/s0268-0033(03)00047-0. [DOI] [PubMed] [Google Scholar]
- 15.Kibler WB, McMullen J. Scapular dyskinesis and its relation to shoulder pain. J Am Acad Orthop Surg. 2003;11(2):142–151. doi: 10.5435/00124635-200303000-00008. [DOI] [PubMed] [Google Scholar]
- 16.Thigpen CA, Padua DA, Michener LA et al. Head and shoulder posture affect scapular mechanics and muscle activity in overhead tasks. J Electromyogr Kinesiol. 2010;20(4):701–709. doi: 10.1016/j.jelekin.2009.12.003. [DOI] [PubMed] [Google Scholar]
- 17.Griegel-Morris P, Larson K, Mueller-Klaus K, Oatis CA. Incidence of common postural abnormalities in the cervical, shoulder, and thoracic regions and their association with pain in two age groups of healthy subjects. Phys Ther. 1992;72(6):425–431. doi: 10.1093/ptj/72.6.425. [DOI] [PubMed] [Google Scholar]
- 18.Finley MA, Lee RY. Effect of sitting posture on 3-dimensional scapular kinematics measured by skin-mounted electromagnetic tracking sensors. Arch Phys Med Rehabil. 2003;84(4):563–568. doi: 10.1053/apmr.2003.50087. [DOI] [PubMed] [Google Scholar]
- 19.Ludewig PM, Cook TM, Nawoczenski DA. Three-dimensional scapular orientation and muscle activity at selected positions of humeral elevation. J Orthop Sports Phys Ther. 1996;24(2):57–65. doi: 10.2519/jospt.1996.24.2.57. [DOI] [PubMed] [Google Scholar]
- 20.Weon JH, Oh JS, Cynn HS, Kim YW, Kwon OY, Yi CH. Influence of forward head posture on scapular upward rotators during isometric shoulder flexion. J Bodyw Mov Ther. 2010;14(4):367–374. doi: 10.1016/j.jbmt.2009.06.006. [DOI] [PubMed] [Google Scholar]
- 21.Ludewig PM, Cook TM. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Phys Ther. 2000;80(3):276–291. [PubMed] [Google Scholar]
- 22.Cools AM, Witvrouw EE, Danneels LA, Cambier DC. Does taping influence electromyographic muscle activity in the scapular rotators in healthy shoulders? Man Ther. 2002;7(3):154–162. doi: 10.1054/math.2002.0464. [DOI] [PubMed] [Google Scholar]
- 23.Hsu YH, Chen WY, Lin HC, Wang WT, Shih YF. The effects of taping on scapular kinematics and muscle performance in baseball players with shoulder impingement syndrome. J Electromyogr Kinesiol. 2009;19(6):1092–1099. doi: 10.1016/j.jelekin.2008.11.003. [DOI] [PubMed] [Google Scholar]
- 24.Miller P, Osmotherly P. Does scapula taping facilitate recovery for shoulder impingement symptoms? A pilot randomized controlled trial. J Man Manip Ther. 2009;17(1):E6–E13. doi: 10.1179/jmt.2009.17.1.6E. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Selkowitz DM, Chaney C, Stuckey SJ, Vlad G. The effects of scapular taping on the surface electromyographic signal amplitude of shoulder girdle muscles during upper extremity elevation in individuals with suspected shoulder impingement syndrome. J Orthop Sports Phys Ther. 2007;37(11):694–702. doi: 10.2519/jospt.2007.2467. [DOI] [PubMed] [Google Scholar]
- 26.Uhl TL, Kibler WB, Tripp BL, Spigelman TH, McClelland RI. Effects of S3 brace on scapular resting position and kinematics. Annual Meeting of the American Orthopaedic Society for Sports Medicine. 2006. Paper presented at: June 29–July. 2, Hershey, PA.
- 27.Uhl TL, Kibler WB, Tripp BL, Spigelman TH, McClelland RI. Paper presented at: Annual Conference of the Society of Shoulder and Elbow Therapists; November 9–12. Palm Beach, FL: 2005. The effectiveness of a scapular brace on scapular kinematics. [Google Scholar]
- 28.Walther M, Werner A, Stahlschmidt T, Woelfel R, Gohlke F. The subacromial impingement syndrome of the shoulder treated by conventional physiotherapy, self-training, and a shoulder brace: results of a prospective, randomized study. J Shoulder Elbow Surg. 2004;13(4):417–423. doi: 10.1016/j.jse.2004.02.002. [DOI] [PubMed] [Google Scholar]
- 29.Cools AM, Declercq GA, Cambier DC, Mahieu NN, Witvrouw EE. Trapezius activity and intramuscular balance during isokinetic exercise in overhead athletes with impingement symptoms. Scand J Med Sci Sports. 2007;17(1):25–33. doi: 10.1111/j.1600-0838.2006.00570.x. [DOI] [PubMed] [Google Scholar]
- 30.Padua DA. Assessment of shoulder-girdle posture in overhead athletes. Athl Ther Today. 2006;11(6):42–46. [Google Scholar]
- 31.Larsson B, Karlberg C, Elert J, Gerdle B. Reproducibility of surface EMG during dynamic shoulder forward flexions: a study of clinically healthy subjects. Clin Physiol. 1999;19(5):433–439. doi: 10.1046/j.1365-2281.1999.00199.x. [DOI] [PubMed] [Google Scholar]
- 32.Meskers CG, de Groot JH, Arwert HJ, Rozendaal LA, Rozing PM. Reliability of force direction dependent EMG parameters of shoulder muscles for clinical measurements. Clin Biomech (Bristol, Avon) 2004;19(9):913–920. doi: 10.1016/j.clinbiomech.2004.05.012. [DOI] [PubMed] [Google Scholar]
- 33.Myers J, Jolly J, Nagai T, Lephart SM. Reliability and precision of in vivo scapular kinematic measurements using an electromagnetic tracking device. J Sport Rehabil. 2006;15(2):125–143. [Google Scholar]
- 34.Cools AM, Witvrouw EE, Declercq GA, Danneels LA, Cambier DC. Scapular muscle recruitment patterns: trapezius muscle latency with and without impingement symptoms. Am J Sports Med. 2003;31(4):542–549. doi: 10.1177/03635465030310041101. [DOI] [PubMed] [Google Scholar]
- 35.Kendall FP, McCreary EK, Provance PG, Rodgers MM, Romani WA. Muscles: Testing and Function With Posture and Pain. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins;; 2005. [Google Scholar]
- 36.Ekstrom RA, Donatelli RA, Soderberg GL. Surface electromyographic analysis of exercises for the trapezius and serratus anterior muscles. J Orthop Sports Phys Ther. 2003;33(5):247–258. doi: 10.2519/jospt.2003.33.5.247. [DOI] [PubMed] [Google Scholar]
- 37.Myers JB, Pasquale MR, Laudner KG, Sell TC, Bradley JP, Lephart SM. On-the-field resistance-tubing exercises for throwers: an electromyographic analysis. J Athl Train. 2005;40(1):15–22. [PMC free article] [PubMed] [Google Scholar]
- 38.Cohen J. A power primer. Psychol Bull. 1992;112(1):155–159. doi: 10.1037//0033-2909.112.1.155. [DOI] [PubMed] [Google Scholar]
- 39.Birmingham TB, Inglis JT, Kramer JF, Vandervoort AA. Effect of a neoprene sleeve on knee joint kinesthesis: influence of different testing procedures. Med Sci Sports Exerc. 2000;32(2):304–308. doi: 10.1097/00005768-200002000-00009. [DOI] [PubMed] [Google Scholar]
- 40.Birmingham TB, Kramer JF, Inglis JT et al. Effect of a neoprene sleeve on knee joint position sense during sitting open kinetic chain and supine closed kinetic chain tests. Am J Sports Med. 1998;26(4):562–566. doi: 10.1177/03635465980260041601. [DOI] [PubMed] [Google Scholar]
- 41.Ulkar B, Kunduracioglu B, Cetin C, Guner RS. Effect of positioning and bracing on passive position sense of shoulder joint. Br J Sports Med. 2004;38(5):549–552. doi: 10.1136/bjsm.2002.004275. [DOI] [PMC free article] [PubMed] [Google Scholar]