

Abstract
OBJECTIVE
This study was designed to examine whether residents living in neighborhoods that are less conducive to walking or other physical activities are more likely to develop diabetes and, if so, whether recent immigrants are particularly susceptible to such effects.
RESEARCH DESIGN AND METHODS
We conducted a population-based, retrospective cohort study to assess the impact of neighborhood walkability on diabetes incidence among recent immigrants (n = 214,882) relative to long-term residents (n = 1,024,380). Adults aged 30–64 years who were free of diabetes and living in Toronto, Canada, on 31 March 2005 were identified from administrative health databases and followed until 31 March 2010 for the development of diabetes, using a validated algorithm. Neighborhood characteristics, including walkability and income, were derived from the Canadian Census and other sources.
RESULTS
Neighborhood walkability was a strong predictor of diabetes incidence independent of age and area income, particularly among recent immigrants (lowest [quintile 1 {Q1}] vs. highest [quintile 5 {Q5}] walkability quintile: relative risk [RR] 1.58 [95% CI 1.42–1.75] for men; 1.67 [1.48–1.88] for women) compared with long-term residents (Q1 to Q5) 1.32 [1.26–1.38] for men; 1.24 [1.18–1.31] for women). Coexisting poverty accentuated these effects; diabetes incidence varied threefold between recent immigrants living in low-income/low walkability areas (16.2 per 1,000) and those living in high-income/high walkability areas (5.1 per 1,000).
CONCLUSIONS
Neighborhood walkability was inversely associated with the development of diabetes in our setting, particularly among recent immigrants living in low-income areas.
Recent decades have seen an unprecedented rise in the global burden of diabetes. According to the World Health Organization, nearly 350 million people worldwide have diabetes, and these figures will continue to climb, fueled by the ongoing epidemic of obesity and aging of the world’s population (1–3). The largest increases in diabetes prevalence are projected to occur in low- and middle-income countries, with the greatest relative rises expected in the Middle East, sub-Saharan Africa, and India (2,4). In many developing countries, globalization as a phenomenon has led not only to economic growth and development but to an increasingly “Western” way of life characterized by sedentarism and the overconsumption of high-energy foods that are low in nutrients (5,6). Local residents in many of these regions carry a high genetic predisposition toward developing diabetes, which renders them particularly vulnerable to elements of the environment that contribute to obesity (4–7).
In developing countries, the rise in diabetes seems to be intricately linked to shifts in urbanization (5,6). In these settings, urbanization has proceeded at a particularly rapid pace, incited by economic development, population growth, and rural-to-urban migration (6,8). The move from a rural, agrarian existence to urban living is associated with increased exposure to unhealthy foods, fewer opportunities for physical activity, and a heightened risk of becoming obese and developing diabetes (3,6).
For the first time in human history, one-half of the world’s population is living in urban areas, and most of the future population growth is expected to occur in such settings (8). Thus, the way we structure and build our cities will play an increasingly greater role in shaping the health of the world’s population. Evidence from industrialized countries suggest that physical activity levels are lower in newly developed areas—characterized by urban sprawl—than older, more traditionally designed neighborhoods, in part because of the reliance suburban design places on mass automobile transit (9–12). The growing literature suggests that residents living in areas that are more walkable are less likely to be obese (11–15). Recent immigrants may be particularly susceptible to such effects. Migration studies have demonstrated that Asian and African populations who move to more Westernized countries experience an accelerated risk of obesity-related conditions, including diabetes within the first 10 years of arrival, a period marked by changes in lifestyle caused by acculturation (16). It is unknown whether the characteristics of communities in which immigrants settle further influences this risk.
The purpose of this study was to examine the impact of neighborhood walkability on the risk of diabetes among recent immigrants to Canada relative to long-term residents. To do so, we used population-level data from Toronto, Canada, one of the most multicultural cities in the world and home to up to 100,000 new immigrants each year (accounting for one-third of all immigration into Canada) (17). We hypothesized that living in a less walkable environment accelerates the risk of diabetes—more so among recent immigrants than long-term residents. We further hypothesized that the combination of genetic predisposition, low income, and a living environment that is less conducive to physical activity constitutes a particularly high-risk exposure for the development of diabetes among recent immigrants (18,19).
RESEARCH DESIGN AND METHODS
Study design
We conducted a retrospective cohort study using a combination of administrative health claims and small area–level data from Toronto, Ontario, Canada. In the province of Ontario, as in the rest of Canada, comprehensive coverage for hospital, physician, and laboratory services is provided to all permanent residents with no deductibles or copayments. Health records for each individual in our cohort were linked anonymously across datasets using an encrypted version of their health card number. Neighborhood-level attributes were then assigned to individuals using their postal code of residence. This protocol received ethical approval from the institutional review boards at St. Michael’s Hospital and Sunnybrook Health Sciences Centre in Toronto.
Study population
The study population was identified using the Registered Persons Database, a provincial health care registry that contains demographic, residential, and vital statistics for virtually all Ontario residents. Men and women living in Toronto on 1 April 2005 who were free of diabetes and eligible for health care coverage for a minimum of 3 years at baseline were eligible for inclusion in our cohort. The population was restricted to adults aged 30 to 64 years because this group is experiencing the most rapid rise in diabetes incidence (20), likely because of trends in obesity. Individuals living in a chronic care institution were excluded from the study.
Recent immigrants were defined as those who first registered for coverage under the province’s healthcare plan within 10 years of baseline (on 1 April 1995 or later). Recent registration has been shown to be a good proxy for recent immigration to Ontario (21). Although country of origin was not available in the databases we used, previous research has shown that most recent immigrants to Toronto are from Asia, Africa, and the Middle East, with only 12% being of European descent (17). This is in contrast to the general Toronto population, in which 58% report being of European ancestry. The final sample size was 1,239,262, consisting of 214,882 recent immigrants and 1,024,380 long-term residents.
Measures
Our primary covariate was the degree to which an individual’s area of residence supports walking and other physical activities. We used a validated walkability index created for Toronto, as described previously (22). Briefly, candidate variables were identified from the literature and were generated using geographic information systems methodology and a combination of census, land use, retail, and public services data. From these, the following area-level attributes were selected for the final index using principal components analysis: population density, dwelling density, street connectivity, and the availability of walkable destinations (number of retail stores and services within a 10-min walk). Index scores positively predicted rates of walking, cycling, and public transit use and were inversely associated with car ownership, driving trips, and levels of obesity (22). For this study, walkability scores were derived for 10,535 dissemination blocks, which are small, residential parcels of land (average population, ∼200). Dissemination blocks were subsequently divided into quintiles, from most walkable (quintile [Q5]) to least walkable (quintile [Q1]), which were then assigned to individuals in our cohort based on their postal code of residence on 1 April 2005.
Other covariates included age, sex, and income. Because individual-level information about income was not available for members of our cohort, we used area-level poverty as a surrogate. This was based on data collected for the 2006 Canadian census, which was used to generate relative income quintiles adjusted for household and community size that were then assigned to individuals. This measure was available at the dissemination area level, a unit slightly larger than dissemination blocks.
Study outcomes
Members of our cohort were followed forward in time, from 1 April 2005 to 31 March 2010, for the development of diabetes. New cases of diabetes were identified using the Ontario Diabetes Database. The Ontario Diabetes Database is a validated electronic database that uses the following algorithm to identify persons with diagnosed diabetes: individuals with at least one hospitalization or at least two claims for physicians’ services (within 2 years) bearing a diagnosis of diabetes are included in the database. This algorithm was found to be highly sensitive (86%) and specific (97%) for identifying patients for whom diabetes was recorded in primary care charts (23). The same algorithm was used to exclude individuals who had pre-existing diabetes at baseline from our study cohort.
Analysis
Random effects Poisson models were used to examine the impact of neighborhood walkability on the incidence of diabetes over the 5-year study period among members of our cohort, according to their immigration status. Separate models were created for men and women on the basis of an a priori hypothesis that neighborhood effects may vary by sex (19). Random effects models were used to account for the clustering of individuals within the same area and the inherent autocorrelation between adjacent areas. We calculated the median rate ratio to quantify this variation in diabetes incidence between geographic clusters (dissemination areas) (24). Additional covariates included in the final models were age (in years) and area income quintile. Tests for interaction between walkability and income were performed based on our a priori hypothesis that concomitant poverty would accentuate the effect of low walkability on diabetes incidence. Person-years of observation were used as an offset in the model. Individuals were followed from 1 April 2005 until the development of diabetes, death, loss of health insurance eligibility because of emigration, or the end of the observation period (31 March 2010), whichever occurred first.
Last, we examined whether area income modified any association between area walkability and diabetes risk. To do so, we compared 5-year age- and sex-standardized diabetes incidence rates within subgroups of our population, defined by their immigration status (recent immigrants versus long-term residents) and income level (lowest, middle, and highest quintile).
RESULTS
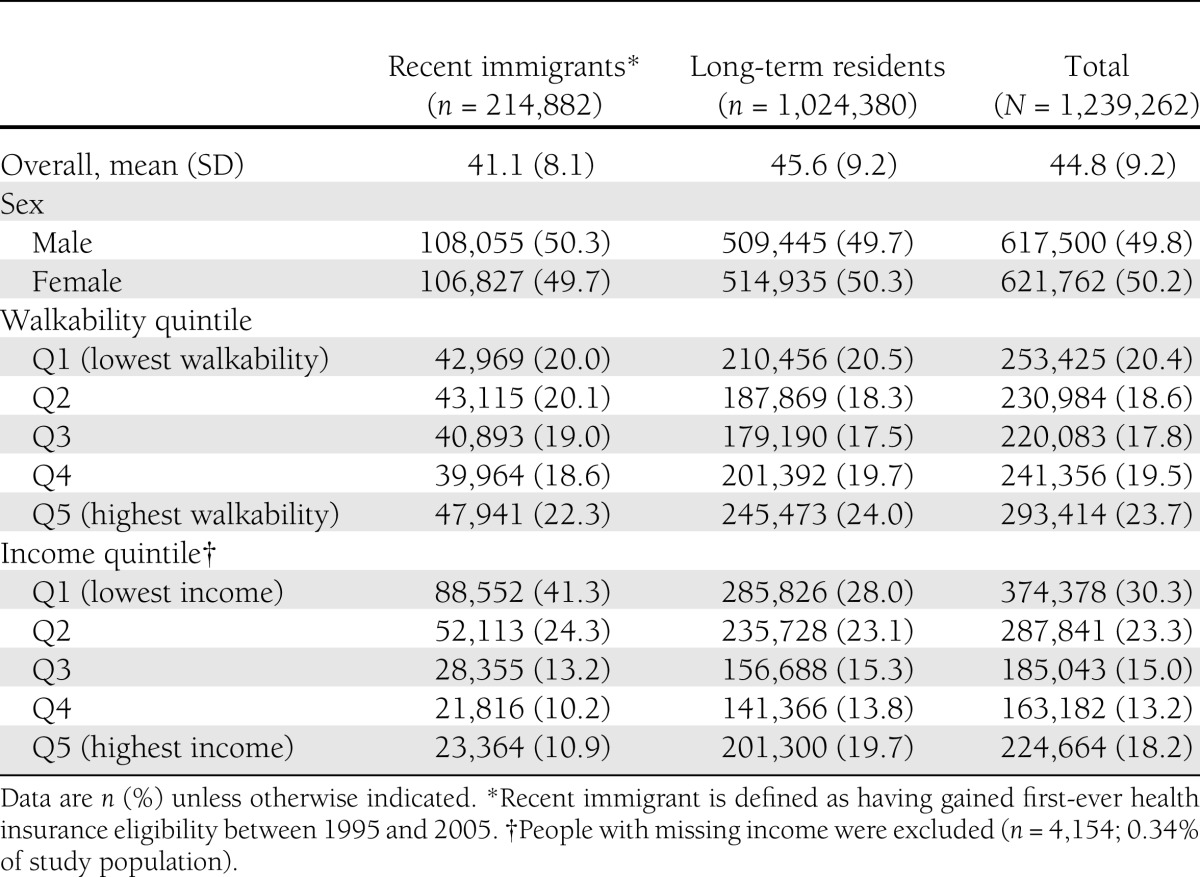
Baseline characteristics of the study population are shown in Table 1. The recent immigrant group was similar to long-term residents in terms of their demographic characteristics and the walkability of their residential area. Recent immigrants, however, were more likely than long-term residents to live in low-income areas.
Table 1.
Baseline characteristics of study population by immigration status
During the period of follow-up, 58,544 men and women in our cohort developed diabetes. There was a large degree of variation in the incidence of diabetes between dissemination areas in our study area on the basis of the calculated median rate ratio (1.44).
We found a strong inverse gradient between area walkability and the incidence of diabetes among both men and women in our cohort (Figs. 1 and 2, respectively). The magnitude of this association was consistently greater among recent immigrants. Recent immigrants living in the least walkable areas had diabetes incidence rates that were more than 50% higher than those living in the most walkable areas (relative risk [RR] 1.58 [95% CI 1.42–1.75] for men; RR 1.67 [95% CI 1.48–1.88] for women) after accounting for differences in age and area poverty. In contrast, the association was less marked among long-term residents (1.32 [1.26–1.38] for men; 1.24 [1.18–1.31] for women). Parameter estimates and relative risks for all variables in our model are presented in Supplementary Tables 1 and 2.
Figure 1.
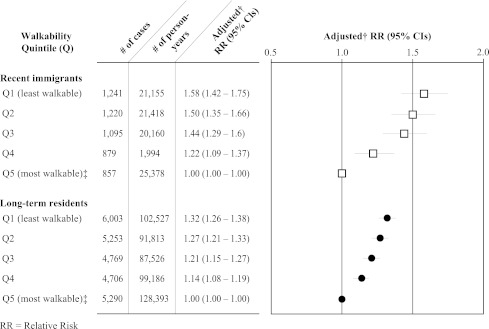
Diabetes risk among men aged 30–64 years by walkability quintile and immigration status (recent immigrants [white squares] vs. long-term residents [black circles]). †Adjusted for age and income using random intercept Poisson model. ‡Reference quintile.
Figure 2.
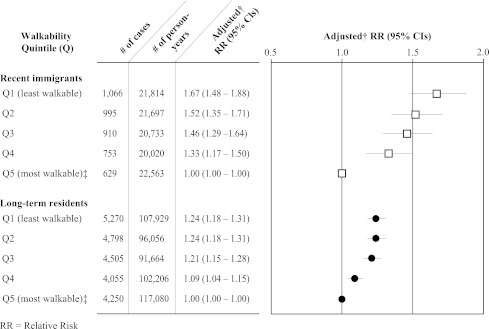
Diabetes risk among women aged 30–64 years by walkability quintile and immigration status (recent immigrants [white squares] versus long-term residents [black circles]). †Adjusted for age and income using random intercept Poisson model. ‡Reference quintile.
There was a significant interaction between neighborhood walkability and income, with respect to their effect on diabetes incidence, both for recent immigrants (P = 0.01) and long-term residents (P = 0.02). Figure 3 shows the relationships between age- and sex-adjusted diabetes incidence rates and area walkability by income and immigration. Low-income areas had diabetes incidence rates that were twofold greater than high-income areas at all levels of walkability. Within low-income areas that were also less walkable, recent immigrants had considerably higher diabetes incidence rates than long-term residents. However, these rates converged in areas of increased walkability. A similar pattern was observed among residents living in middle-income areas (data not shown). In high-income areas, diabetes incidence was low, did not differ greatly between recent immigrants and long-term residents, and declined slightly with increasing walkability. There was a more than threefold variation in diabetes incidence between recent immigrants living in low-income, low walkability areas (16.2 per 1,000) and those living in high-income, high walkability areas (5.1 per 1,000).
Figure 3.

Age- and sex-standardized 5-year diabetes incidence rates for adults aged 30–64 years by walkability index quintile, income, and immigration status. White squares indicate low-income recent immigrants based on data collected in 2005 for 2006 Canadian census. Black circles indicate low-income long-term residents based on 2006 Canadian census data. Black squares indicate high-income recent immigrants and white circles indicate high-income, long-term residents. *For period from 1 April 2005 to 31 March 2010.
CONCLUSIONS
Our findings demonstrate that residents living in less walkable areas, particularly recent immigrants in low-income neighborhoods, have an accelerated risk of developing diabetes compared with those living in more walkable areas. Although diabetes can be prevented through physical activity, healthy eating, and weight loss (25), the environment in which one lives may pose barriers to achieving these measures that are difficult to overcome. Lessons learned from successful antismoking campaigns in the past suggest that population-level strategies can play a key role in promoting healthy behaviors (26). Moreover, public policies that target whole populations may prevent as many cases of diabetes as those targeting high-risk individuals alone (27,28). Our findings support the concept that neighborhood design potentially could influence the health of urban populations through the opportunities it provides for residents to undertake healthy behaviors. This may have practical implications for community-level interventions aimed at diabetes prevention.
Like many cities in the U.S. and Europe, recent immigrants in our setting are most often of South Asian, East Asian, or African descent, groups that are particularly susceptible to the development of diabetes (7,29). Recent immigrants are often underemployed relative to their occupational roles in their home country and therefore experience low socioeconomic status relative to the host country population, leading to their residence in less desirable areas of major urban centers. Although the prevalence of chronic conditions is often lower among recent immigrants, a phenomenon known as the “healthy migrant” effect (30), this was not the case for diabetes among recent arrivals in our setting, especially for those living in low-income and low walkability areas. The growing trend of rapid urbanization in developing countries, together with rich diets and sedentary lifestyles in those settings, may have resulted in less healthy migrant populations to Canada in recent years, especially with regard to their risk of obesity-related conditions such as diabetes (5,6,31). The role of poverty in accentuating the risk of diabetes in recent immigrants is likely multifactorial. Lower-income populations may rely more on local, low-cost opportunities for physical activity within their neighborhood than their wealthier counterparts because of limited financial resources. Moreover, for complex diseases, such as diabetes, the cumulative effect of multiple environmental insults (e.g., poverty, lack of opportunities for physical activity, and greater exposure to inexpensive, unhealthy foods) may dramatically heighten the risk of disease in genetically susceptible individuals (18,19,32).
Our findings are supported by other studies demonstrating an association between neighborhood features that discourage physical activity and risk factors for diabetes such as physical inactivity, insulin resistance, and obesity (9–15,33). However, virtually all of these were cross-sectional in design. An exception is an analysis by Berry et al. (34), which noted several neighborhood characteristics that predicted long-term weight gain, including area poverty and higher levels of perceived traffic. Relatively few studies have examined the relationship between neighborhood features and discrete health outcomes such as diabetes. In the Multiethnic Study of Atherosclerosis, participants who reported having better neighborhood resources for physical activity and healthy foods were 38% less likely to develop diabetes over a 5-year period (35). Our study adds to this literature by suggesting that neighborhood walkability is also a significant risk factor for the development of diabetes among young and middle-aged adults living in urban settings and that recent immigrants are particularly susceptible to its influence.
In many cities around the world, the walkability of a neighborhood is tied to the era in which it was first developed. In Toronto, as in other North American cities, the older neighborhoods, built predominantly before World War II, have characteristics that enhance their walkability, including higher residential densities, shorter block lengths, and the coexistence of residential and commercial areas in the same neighborhood. The latter provides residents with a choice between walking and other modes of travel to reach routine destinations. During the period after World War II, this style of urban design was largely replaced by a shift toward sprawling developments and the separation of land uses through legislated changes in zoning. This led to tremendous growth of purely residential, automobile-oriented suburban communities. Suburban living dramatically reduces the opportunities residents have to engage in transportation-related physical activity, such as walking or bicycling to work or school or to run errands (9–12,36). The automobile-oriented planning practices of the 1960s and 1970s have been contested by the “New Urbanism” movement, which promotes a return to pre–World War II styles of urban design. Many cities are now setting limits on further suburban sprawl, instead favoring high-density development in major employment and retail areas and along major transportation corridors. In this way, urban landscapes can be modified over time.
Our research approach had both limitations and strengths. One limitation of this work is that it included a single municipality; therefore, our findings may not apply to other settings. However, historical trends in urban development that occurred in Toronto are typical of those that occurred in other cities in North America and elsewhere in the world. Our setting is also one of the most multicultural cities globally, making it an ideal setting for this type of research. Although our analysis was based on individuals, socioeconomic status could be measured at only the area level. That measure was based on very small residential units, which have been shown to be a good proxy for individual income (37). Our data did not include country or region of origin or timing of immigration, and for that reason we used a proxy measure for recent immigration: recent registration for Ontario health care. Previous research showed that most individuals (>80%) captured using this method are new immigrants; however, the remainder include both immigrants and nonimmigrants who migrate between provinces (21). This misclassification would tend to reduce the differences between the recent immigrant and long-term resident groups studied. The recent immigrant group is likely to be heterogeneous with respect to factors influencing their rate of assimilation, including their country of origin, prior “Westernization,” and the presence of family members in Canada, which we were not able to account for in our analysis. In addition, ethnoracial composition was not available in our data, but most immigrants to Ontario are from populations that carry a high genetic predisposition for developing diabetes (7,29). Furthermore, recent immigrants are well distributed across Toronto, with few ethnic enclaves (38); thus, clustering of ethnic populations should not account for our findings.
Other area-level factors could have contributed to our findings. Differences in the retail food environment potentially could influence rates of obesity and insulin resistance (32,33,35); however, a previous study found higher concentrations of convenience stores and fast food outlets in the more walkable neighborhoods of Toronto (38). Last, unmeasured confounders could have contributed to the association between neighborhood walkability and diabetes incidence; therefore, we cannot prove definitively that this relationship was directly causal. We hypothesize that living in a less walkable neighborhood increases one’s risk of diabetes through its effects on physical activity and obesity, based on the vast literature supporting the association between neighborhood environments and these entities, including research conducted in Toronto using our index and similar measures elsewhere (9–15,38,39). However, information about BMI, physical activity levels, and travel behaviors was lacking in our datasets.
Collectively, this line of research supports the notion that where one live has a profound influence on one’s health. This is a fundamental shift in the paradigm in which we view the etiology of chronic diseases such as diabetes—from a purely biomedical one to one that incorporates the larger world in which we live. Moreover, it opens up other avenues for the prevention of obesity-related diseases that include changes in the way communities are designed (40). As the fast pace of urbanization continues, particularly in developing countries, lessons learned from industrialized nations will be increasingly valuable. Further research is needed to establish the consistency of these findings in other settings, to identify the world regions and ethnoracial groups most susceptible to these effects, and, most importantly, to more fully understand what impact interventions targeting the built environment might have on levels of obesity and diabetes.
Supplementary Material
Acknowledgments
This work was funded by research grants from the Canadian Diabetes Association and the Canadian Institutes of Health Research. This study also was supported by the Institute for Clinical Evaluative Sciences and the Centre for Research on Inner City Health at The Keenan Research Centre in the Li Ka Shing Knowledge Institute of St. Michael’s Hospital, Toronto, Ontario, Canada, and the Ontario Ministry of Health and Long-Term Care. G.L.B. holds a New Investigator Award funded by the Canadian Institutes of Health Research and the Ontario Women’s Health Council.
No potential conflicts of interest relevant to this article were reported.
G.L.B. and R.H.G. conceived of and designed the study and wrote the manuscript. M.I.C. researched data, contributed to the discussion, and reviewed and edited the manuscript. R.M., P.G., J.T.W., and F.I.M. contributed to the discussion and reviewed and edited the manuscript. G.L.B. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
The authors thank Ghazal Fazli of the Li Ka Shing Knowledge Institute of St. Michael’s Hospital for administrative support.
Footnotes
This article contains Supplementary Data online at http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc12-0777/-/DC1.
References
- 1.World Health Organization. Diabetes fact sheet no. 312. 2011. Available from http://www.who.int/mediacentre/factsheets/fs312/en/ Accessed 14 July 2011
- 2.Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 2004;27:1047–1053 [DOI] [PubMed] [Google Scholar]
- 3.Swinburn BA, Sacks G, Hall KD, et al. The global obesity pandemic: shaped by global drivers and local environments. Lancet 2011;378:804–814 [DOI] [PubMed] [Google Scholar]
- 4.Danaei G, Finucane MM, Lu Y, et al. Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (Blood Glucose) National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2·7 million participants. Lancet 2011;378:31–40 [DOI] [PubMed] [Google Scholar]
- 5.Hu FB. Globalization of diabetes: the role of diet, lifestyle, and genes. Diabetes Care 2011;34:1249–1257 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Shetty P, Schmidhuber J. Nutrition, lifestyle, obesity and chronic disease. United Nations Department of Economic and Social Affairs, Population Division Expert Paper No. 2011/3. New York, NY: United Nations; 2011. Avilable from http://www.un.org/esa/population/publications/expertpapers/2011-3-shetty.pdf Accessed 1 August 2011
- 7.Chiu M, Austin PC, Manuel DG, Shah BR, Tu JV. Deriving ethnic-specific BMI cutoff points for assessing diabetes risk. Diabetes Care 2011;34:1741–1748 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cohen B. Urbanization in developing countries: current trends, future projections, and key challenges for sustainability. Technol Soc 2006;28:63–80 [Google Scholar]
- 9.Frank LD, Schmid TL, Sallis JF, Chapman J, Saelens BE. Linking objectively measured physical activity with objectively measured urban form: findings from SMARTRAQ. Am J Prev Med 2005;28(Suppl 2):117–125 [DOI] [PubMed] [Google Scholar]
- 10.Owen N, Cerin E, Leslie E, et al. Neighborhood walkability and the walking behavior of Australian adults. Am J Prev Med 2007;33:387–395 [DOI] [PubMed] [Google Scholar]
- 11.Berke EM, Koepsell TD, Moudon AV, Hoskins RE, Larson EB. Association of the built environment with physical activity and obesity in older persons. Am J Public Health 2007;97:486–492 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Frank LD, Andresen MA, Schmid TL. Obesity relationships with community design, physical activity, and time spent in cars. Am J Prev Med 2004;27:87–96 [DOI] [PubMed] [Google Scholar]
- 13.Hoehner CM, Handy SL, Yan Y, Blair SN, Berrigan D. Association between neighborhood walkability, cardiorespiratory fitness and body-mass index. Soc Sci Med 2011;73:1707–1716 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Feng J, Glass TA, Curriero FC, Stewart WF, Schwartz BS. The built environment and obesity: a systematic review of the epidemiologic evidence. Health Place 2010;16:175–190 [DOI] [PubMed] [Google Scholar]
- 15.Papas MA, Alberg AJ, Ewing R, Helzlsouer KJ, Gary TL, Klassen AC. The built environment and obesity. Epidemiol Rev 2007;29:129–143 [DOI] [PubMed] [Google Scholar]
- 16.Misra A, Ganda OP. Migration and its impact on adiposity and type 2 diabetes. Nutrition 2007;23:696–708 [DOI] [PubMed] [Google Scholar]
- 17.Citizenship and Immigration Canada. Facts and figures, 2010—Immigration Overview. Ottawa, Ontario: Strategic Policy, Planning and Research, Citizenship and Immigration Canada, 2011. Available from http://www.cic.gc.ca/english/resources/statistics/menu-fact.asp Accessed 18 October 2011
- 18.Ludwig J, Sanbonmatsu L, Gennetian L, et al. Neighborhoods, obesity, and diabetes—a randomized social experiment. N Engl J Med 2011;365:1509–1519 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Matheson FI, Moineddin R, Glazier RH. The weight of place: a multilevel analysis of gender, neighborhood material deprivation, and body mass index among Canadian adults. Soc Sci Med 2008;66:675–690 [DOI] [PubMed] [Google Scholar]
- 20.Lipscombe LL, Hux JE. Trends in diabetes prevalence, incidence, and mortality in Ontario, Canada 1995-2005: a population-based study. Lancet 2007;369:750–756 [DOI] [PubMed] [Google Scholar]
- 21.Ray JG, Vermeulen MJ, Schull MJ, Singh G, Shah R, Redelmeier DA. Results of the Recent Immigrant Pregnancy and Perinatal Long-term Evaluation Study (RIPPLES). CMAJ 2007;176:1419–1426 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Glazier RH, Weyman JT, Creatore MI, et al. A Geographic Approach for Developing and Validating Urban Walkability Indices. Available from http://www.torontohealthprofiles.ca/a_documents/aboutTheData/12_1_ReportsAndPapers_Walkability_WKB_2012.pdf Accessed 16 April 2012
- 23.Hux JE, Ivis F, Flintoft V, Bica A. Diabetes in Ontario: determination of prevalence and incidence using a validated administrative data algorithm. Diabetes Care 2002;25:512–516 [DOI] [PubMed] [Google Scholar]
- 24.Larsen K, Merlo J. Appropriate assessment of neighborhood effects on individual health: integrating random and fixed effects in multilevel logistic regression. Am J Epidemiol 2005;161:81–88 [DOI] [PubMed] [Google Scholar]
- 25.Knowler WC, Barrett-Connor E, Fowler SE, et al. Diabetes Prevention Program Research Group Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002;346:393–403 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Yach D, McKee M, Lopez AD, Novotny T. Improving diet and physical activity: 12 lessons from controlling tobacco smoking. BMJ 2005;330:898–900 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Rosella LC, Manuel DG, Burchill C, Stukel TA, PHIAT-DM team A population-based risk algorithm for the development of diabetes: development and validation of the Diabetes Population Risk Tool (DPoRT). J Epidemiol Community Health 2011;65:613–620 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Wang YC, McPherson K, Marsh T, Gortmaker SL, Brown M. Health and economic burden of the projected obesity trends in the USA and the UK. Lancet 2011;378:815–825 [DOI] [PubMed] [Google Scholar]
- 29.Creatore MI, Moineddin R, Booth G, et al. Age- and sex-related prevalence of diabetes mellitus among immigrants to Ontario, Canada. CMAJ 2010;182:781–789 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Singh GK, Siahpush M. All-cause and cause-specific mortality of immigrants and native born in the United States. Am J Public Health 2001;91:392–399 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Yang W, Lu J, Weng J, et al. China National Diabetes and Metabolic Disorders Study Group Prevalence of diabetes among men and women in China. N Engl J Med 2010;362:1090–1101 [DOI] [PubMed] [Google Scholar]
- 32.Hemphill E, Raine K, Spence JC, Smoyer-Tomic KE. Exploring obesogenic food environments in Edmonton, Canada: the association between socioeconomic factors and fast-food outlet access. Am J Health Promot 2008;22:426–432 [DOI] [PubMed] [Google Scholar]
- 33.Auchincloss AH, Diez Roux AV, Brown DG, Erdmann CA, Bertoni AG. Neighborhood resources for physical activity and healthy foods and their association with insulin resistance. Epidemiology 2008;19:146–157 [DOI] [PubMed] [Google Scholar]
- 34.Berry TR, Spence JC, Blanchard C, Cutumisu N, Edwards J, Nykiforuk C. Changes in BMI over 6 years: the role of demographic and neighbourhood characteristics. Int J Obes (Lond) 2010;34:1275–1283 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Auchincloss AH, Diez Roux AV, Mujahid MS, Shen M, Bertoni AG, Carnethon MR. Neighborhood resources for physical activity and healthy foods and incidence of type 2 diabetes mellitus: the Multi-Ethnic study of Atherosclerosis. Arch Intern Med 2009;169:1698–1704 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Larsen K, Gilliland J, Hess P, Tucker P, Irwin J, He M. The influence of the physical environment and sociodemographic characteristics on children’s mode of travel to and from school. Am J Public Health 2009;99:520–526 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Krieger N. Overcoming the absence of socioeconomic data in medical records: validation and application of a census-based methodology. Am J Public Health 1992;82:703–710 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Glazier RH, Booth GL, Gozdyra P, Creatore MI, Tynan A-M (eds). Neighbourhood environments and resources for healthy living: a focus on diabetes in Toronto. Toronto, Ontario: Institute for Clinical Evaluative Sciences, 2008. Available from http://www.ices.on.ca/file/TDA_ICES_Prelim_press.pdf Accessed 31 May 2008
- 39.Toronto Public Health. The walkable city: neighbourhood design and preferences, travel choices and health. April 2012. Available from http://www.toronto.ca/health/hphe/pdf/walkable_city.pdf 18 April 2012.
- 40.Gortmaker SL, Swinburn BA, Levy D, et al. Changing the future of obesity: science, policy, and action. Lancet 2011;378:838–847 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.