

Abstract
Background:
Bladder cancer is the fourth most common malignancy in men and the eighth most common in women. It causes 8% of all malignancies in men and 3% of all malignancies in women. The trend of bladder cancer is increasing in Iran. This study was conducted to estimate the survival rate of bladder cancer based on life table method.
Materials and Methods:
In this study, at first, data were collected based on individual variables of 514 patients suffering from bladder cancer and referred them to cancer registry center of Shiraz University of Medical Sciences from 2001-2009. Data were collected at two stages and analyzed by life table method and Wilcox on test. Significant level considered at 0.05.
Results:
Our findings showed that probability of survival accumulation at the end of 1, 3, 5, 10 years in patients with bladder cancer were equal to 0.8989, 0.7132, 0.5752 and 0.2459 respectively. There was significant difference in survival rate among age groups and treatment types (P < 0.05). However, we did not observe any difference in survival time based on smoking (P = 0.578), alcohol (P = 0.419) and education level (P = 0.371) of patients.
Conclusion:
The overall survival rate of bladder cancer in the present study was less than other areas. Patients’ age and treatment type were the influential factor in survival time. So continuous screening for early diagnosis suggested for older people.
Keywords: Life tables, survival time, urinary bladder neoplasm
INTRODUCTION
Bladder cancer is the eighth cause of deaths resulting from different types of cancer.[1] In addition, it leads to 3% of malignancies. Based on the available statistics, bladder cancer is the fourth common cancer causing 8% of malignancies as well as 3% of deaths resulting from cancer in males, and causing 3% of malignancies as well as 1.5% of deaths resulting from cancer in females.[1,2] Available statistics in Iran reveal that bladder cancer is of great importance. Based on the Fars cancer statistics center, bladder cancer has been the fifth common cancer in Fars.[3] Moreover, this disease has been the second, the third, and the fourth common cancer in Markazi, Kordestan, and in general, respectively.[4,5]
Bladder cancer leads to a large number of deaths. Hematuria is the clinical protest of the bladder cancer which can be observed in 75% of the patients; however, since it is not accompanied with pain, it does not produce any symptoms at the beginning of the disease.[6] Various studies conducted on the bladder cancer have proved the relationship between the occupation, smoking, and gender, and the bladder cancer. For example, these studies have shown that the incidence of bladder cancer in males is 4 to 5.2 times more than females.[6–8] Also, smoking cigarettes has been considered the greatest factor resulting in bladder cancer in western societies. Results of a review study in Europe depicted that about 66% of bladder cancer in males as well as 30% of this disease in females is due to smoking cigarettes.[9,10] Smoking cigarettes in addition to being exposed to carcinogenic chemicals because of one's occupation, both, lead to bladder cancer as well as its development.[11–13] Moreover, Urinary Tract Infection (UTI), kidney and bladder stones, parasitic infections, and the causes of chronic bladder irritation are, all, related to the bladder cancer, but do not necessarily lead to the incidence of the disease.[14]
The studies conducted abroad show that the five year survival in invasive cancers and the overall survival of such patients are variable from 40% to 60% and from 70% to 85%, respectively. In general, the rate of survival in females is poor compared to males.[15–18] Although the incidence of bladder cancer is increasing in Iran, no research was found regarding the specification of the survival rate in Iranian patients suffering from the bladder cancer; most of studies were carried out in order to examine the development of the cancer as well as its causes and epidemiologic study.[3–5,19] Therefore, the present study aims at estimating the rate of survival in patients suffering from the bladder cancer according to the life table method and based on the important influential variables.
MATERIALS AND METHODS
The present study is a retrospective cohort study of survival analysis which has been conducted on 514 patients suffering from the bladder cancer registered in cancer registry center of Namazi hospital. This hospital is the only referral center in Fars which registers and follows up all the patients referred from different cities of the province. The participants of the study must have had at least one complete follow-up which indicated their living status for a while. Therefore, the patients who were not available due to either the change in their address and phone number or migration as well as recurrent cases were excluded from the study (N = 36). The statistical society under study included the residents of Shiraz and South of Iran who – in case of suffering from the bladder cancer – referred to the cancer registry center of Shiraz Namazi hospital and were cured and cared for. Sampling census was conducted, and all the patients who had registered in the cancer registry center of Shiraz Namazi hospital from 1380 to 1388 entered the study. In order to gather the data, first, the patients’ information files were prepared by referring to the cancer registry center of Shiraz Namazi hospital and obtaining the patients’ basic information. On the second step, the final status of the patients was tracked by their addresses and phone numbers. In case the phone calls were not successful, patients were called three times a week in a two-week period. If the patients did not respond to the phone calls in this period, they were considered as the lost data.
Two questionnaires were used in order to gather the data. The first one consisted of the patients’ general information including demographic variables such as: age, sex, marital status, ethnicity, nationality, blood group, grade of the disease, and type of treatment which was completed by using the patients’ files. The second questionnaire, on the other hand, was related to the participants’ follow-up, and included information regarding the call time as well as the patients’ status at the moment of their follow-up. Survival time was considered the period from the definite diagnosis of the disease to the time of death and the time of follow-up for dead and alive participants, respectively.
The data gathered from the patients was coded and then analyzed through the SPSS software (version 13). Since, the patients’ survival time was gathered in a classified manner based on the season, the data was analyzed through the life table and the Wilcox on test. The level of significance was considered as 0.05.
RESULTS
The information file of 478 participants was complete. However, the information regarding the final status of 28 participants was not found after calling the patients three times a week or visiting them in two consecutive weeks. Therefore, the survival analysis was carried out on 450 participants among whom 206 participants (45.8%) were alive and had recovered or were being followed up or cured and 244 participants (54.2%) had died. The mean and the standard deviation of variables of age, BMI, and time of follow-up were obtained as 64.2 ± 12.9 years, 23.7 ± 4.7 kg/m2, and 62.6 ± 48.4 months respectively. Male participants constituted 84.5% (404 participants) of the study, while females constituting only 15.5% (74 participants). Besides, 431 participants (90.5%) were married, and 387 participants (81.6%) were Persian. Taking the grade of the disease into account, all patients were located in the zero or one grade. Also, regarding the age, 67 participants (14%) were below 50, 111 participants (23.2%) were between 50 and 60, 128 participants (26.8%) were between 60 and 70, and 172 participants (36%) aged over 70 years old. Moreover, 45 participants of the study (10.2%) were thin, 241 participants (54.6%) had a normal weight, and 155 participants (35.1%) suffered from obesity. The prevalence of alcohol consumption among the participants of the study was 5.5% (25 participants). And taking smoking into consideration, 38.3% (180 participants) smoked, 11.3% (53 participants) used the Hookah, 15.1% (71 participants) were addicted to morphine, and 35.3% (166 participants) included the non-smokers. Moreover, 130 participants (27.8%) were farmers, 76 participants (16.3%) were homemakers, 98 participants (21%) were employees, and 163 participants (34.9%) were workers. In addition, the education level of 27 participants (16.3%) was below the guidance school, while that of 139 participants (83.7%) was up the guidance school. Regarding the type of treatment, 373 participants (78.7%) were operated, 17 participants (3.6%) went under either chemotherapy or radio therapy, and 84 participants (17.7%) were treated through the combination therapy. The survival accumulation at the end of 1, 3, 5, and 10 years in the patients were equal to 0.8989, 0.7132, 0.5752, and 0.2459 respectively. According to the life table method as well as the results depicted in Table 1, one can observe that only the two variables of age and type of treatment affect the patients’ survival.
Table 1.
The relationship between the variables under study and the survival rate of bladder cancer
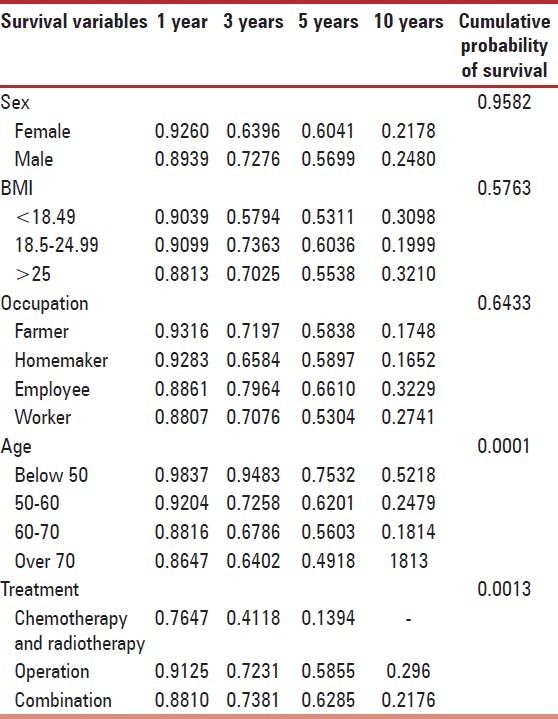
Wilcoxon test in a two-way analysis revealed that the survival of the patients under 50 years old was more than other age groups. Also, the patients who had gone under combination therapy had a higher survival rate comparing to the patients who had received the other types of treatment. Nevertheless, there was no significant difference in the survival rate based on the variables of sex, occupation, and BMI (P > 0.05). There was, also, no significant difference in survival rate and the variables of smoking (P = 0.578), alcohol consumption (P = 0.419), level of education (P = 0.371), ethnicity (P = 0.205), marital status (P = 0.820), blood group (P = 0.58), and the grade of the disease (P = 0.326).
DISCUSSION
The survival accumulation at the end of 1, 3, 5, and 10 years in the patients were equal to 0.8989, 0.7132, 0.5752, and 0.2459 respectively. Sex ratio of males to females was equal to 5.5 in the present study. Therefore, males constituted 84.5% of the participants. However, no significant difference was observed in the survival rate between male and female participants. Rodriguez et al., also, conducted a study in which male patients constituted 83.3% of the participants.[18] Results of another study – in which females constituted 34.6% of the participants – depicted that the survival accumulation in males was more than females at the end of five years in a way that the survival rate in males was 10.9% more than females three months after the diagnosis. Six months after the diagnosis, this result increased to 19.9%. However, the difference reduced after six months.[20] According to WHO, the survival accumulation at the end of five years in Thai females and males suffering from the bladder cancer has been equal to 39 and 61.5% respectively. Nevertheless, the survival accumulation at the end of five years in female and male patients from Madras, India has been reported as 15 and 25% respectively.[21] Moreover, a multi ethnic study revealed that the survival rate of Asian females was lower than Asian males.[22]
Based on the life table model, the survival accumulations at the end of five and ten years were equal to 0.5752 and 0.2459 respectively. In a study by Manterola et al., the survival accumulation at the end of five years was reported as 50%.[23] Also, in another study which was carried out on 333 patients treated by radio therapy, the survival accumulations at the end of five and ten years were calculated as 57 and 54% respectively.[24] Another multi ethnic study showed that the overall survival of bladder cancer was 66, 61, 59, and 52% in Japanese, Caucasian, Filipino, and Hawaiian patients respectively.[22] In the same line, it seems that the survival rate of patients suffering from the bladder cancer is lower than other areas. Of course, the influence of the early diagnosis of the disease due to the newer and more effective methods employed in developed countries must, also, be taken into consideration. Besides, the difference might, also, be due to the Lead time Bias.
Results of the study depicted that the survival rate of the patients suffering from the bladder cancer is related to their age; the older the patients, the lower their survival rate will be. In a study conducted by Fairey et al, the survival rates of the patients between 60-70 and those between 70-80 were reduced respectively 1.3 and 1.2 times in comparison to the patients aging under 60 years old.[25]
It has been predicted that the burden of diseases related to cancer will increase due to the control of the infectious diseases as well as the growth of geriatric in developing countries. Therefore, cancer will have a 30% increase in developed countries and a 71% increase in developing countries from 1990 to 2010.[21]
Results of the present study revealed that the type of treatment is quite influential on the patients’ rate of survival. Patients who receive the chemotherapy or the radiotherapy have a lower survival rate comparing to those who are operated or receive a combination therapy including an operation and radiotherapy or chemotherapy. In a study by Gulliford et al., also, the type of treatment was reported as significant in the survival rate. Severity of the disease was considered the most influential factor on the patients’ survival in that study.[26] Chemotherapy has been considered a gold standard for patients suffering from the bladder cancer; however, 50% of the patients suffering from invasive diseases die in spite of chemotherapy.[27] Removal of the bladder and pelvic tissues involved is considered as the standard treatment of the patients suffering from invasive bladder cancer. Nevertheless, radiotherapy is the only solution for the patients who cannot receive the standard treatment due to their age, status, and suffering from other diseases.[28] Therefore, based on the available findings, combination therapy is the final treatment of the disease.[27] According to other studies carried out on the issue, a combination of radiotherapy, pharmaceutical supplements, and operation can be quite beneficial on the survival rate of the patients.[28] Of course, it should be noted that according to a study conducted in England, the survival rate of the bladder cancer has been decreasing from 1998 to 2004[29] which highlights the necessity of reform in early diagnosis of the disease, right use of medication, radiotherapy, operation, and a combination of all these methods. Available witnesses reveal that the accumulation of survival rate at the end of five years is variable less than 60% in the beginning and 20-30% in the third and the fourth grades based on the severity and the degree of the disease. Type of the treatment is highly effective on the rate of survival; the accumulation of survival rate at the end of five years increases up to 80% in patients who undergo the colon operation.[23] It is quite obvious that the type of treatment based on the patients’ conditions such as sex, severity of the disease, and age is highly influential on the prognosis of the disease. However, the present study did not show the effect of sex and severity of the disease on the survival rate due to the small number of the patients in sub categories.[23,24]
The manifest characteristic of the bladder cancer is that it tends to relapse as time passes, in a way that it relapses in an invasive manner in 10-15% of the cases. Therefore, relapse of the disease threats the patients all through their lives.[6] Also, various studies have shown that the delay in referring the patients to clinics in order to begin the treatment is one of the most important factors in management of the disease which can lead to the decrease in the patients’ survival rate.[30] Therefore, early diagnosis of the disease in the beginning process of the bladder tissue damage has been emphasized since it increases the accumulation of the survival rate at the end of five years up to 100%.[23] The overall survival rate of bladder cancer in participants of the present study was lower than other areas. Since age and the type of treatment are influential factors in survival time, continuous screening for early diagnosis as well as employing combination therapy is seems to be suggested for older people.
ACKNOWLEDGEMENT
The authors are also grateful for Research Improvement Center of Shiraz University of Medical Sciences and Ms. A. Keivanshekouh for their cooperation in improving the use of English in the manuscript.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Shah A, Rachet B, Mitry E, Cooper N, Brown CM, Coleman MP. Survival from bladder cancer in England and Wales up to 2001. Br J Cancer. 2008;99:S86–9. doi: 10.1038/sj.bjc.6604599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Andrew AS, Gui J, Sanderson AC, Mason RA, Morlock EV, Schned AR, et al. Bladder cancer SNP panel predicts susceptibility and survival. Hum Genet. 2009;125:527–39. doi: 10.1007/s00439-009-0645-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Tootoonchi M, Mazdak H, Najafipoor SH, Soleimani B. Bladder cancer risk factors among Isfahan population: A case-control study. [Persian] J Res Med Sci. 2000;2:156–1. [Google Scholar]
- 4.Mohaghegh F, Hamta A, Shariatzadeh SM. The study of cancer incidence and cancer registration in Markazi province between 2001-2006 and comparison with national statistics, Iran. [Persian] Rahavard Danesh. 2008;2:84–93. [Google Scholar]
- 5.Ahmad E, Ghasemkhani O, Dastoori P. Recurrence rate and prognostic factors of superficial bladder cancer in shiraz shahid faghihi hospital during the years 1998-2001. [Persian] J Zanjan Univ Med Sci. 2003;42:1–7. [Google Scholar]
- 6.Whelan P. Survival from bladder cancer in England and Wales up to 2001. Br J Cancer. 2008;99:S90–2. doi: 10.1038/sj.bjc.6604600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Scosyrev E, Noyes K, Feng C, Messing E. Sex and racial differences in bladder cancer presentation and mortality in the US. Cancer. 2009;115:68–74. doi: 10.1002/cncr.23986. [DOI] [PubMed] [Google Scholar]
- 8.Brookfield KF, Cheung MC, Gomez C, Yang R, Nieder AM, Lee DJ, et al. Survival disparities among African American women with invasive bladder cancer in Florida. Cancer. 2009;115:4196–209. doi: 10.1002/cncr.24497. [DOI] [PubMed] [Google Scholar]
- 9.Brennan P, Bogillot O, Cordier S, Greiser E, Schill W, Vineis P, et al. Cigarette smoking and bladder cancer in men: A pooled analysis of 11 case-control studies. Int J Cancer. 2000;86:289–94. doi: 10.1002/(sici)1097-0215(20000415)86:2<289::aid-ijc21>3.0.co;2-m. [DOI] [PubMed] [Google Scholar]
- 10.Brennan P, Bogillot O, Greiser E, Chang-Claude J, Wahrendorf J, Cordier S, et al. The contribution of cigarette smoking to bladder cancer in women (pooled European data) Cancer Causes Control. 2001;12:411–7. doi: 10.1023/a:1011214222810. [DOI] [PubMed] [Google Scholar]
- 11.Gaertner RR, Trpeski L, Johnson KC Canadian Cancer Registries Epidemiology Research Group. A casecontrol study of occupational risk factors for bladder cancer in Canada. Cancer Causes Control. 2004;15:1007–19. doi: 10.1007/s10552-004-1448-7. [DOI] [PubMed] [Google Scholar]
- 12.Kogevinas M, ‘t Mannetje A, Cordier S, Ranft U, González CA, Vineis P, et al. Occupation and bladder cancer among men in Western Europe. Cancer Causes Control. 2003;14:907–14. doi: 10.1023/b:caco.0000007962.19066.9c. [DOI] [PubMed] [Google Scholar]
- 13.Smailyte G, Kurtinaitis J, Andersen A. Mortality and cancer incidence among Lithuanian cement producing workers. Occup Environ Med. 2004;61:529–34. doi: 10.1136/oem.2003.009936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bejany DE, Lockhart JL, Rhamy RK. Malignant vesical tumors following spinal cord injury. J Urol. 1987;138:1390–2. doi: 10.1016/s0022-5347(17)43651-2. [DOI] [PubMed] [Google Scholar]
- 15.Manoharan M, Ayyathurai R, Soloway MS. Radical cystectomy for urothelial carcinoma of the bladder: An analysis of preoperative and survival outcome. BJU Int. 2009;104:1227–32. doi: 10.1111/j.1464-410X.2009.08625.x. [DOI] [PubMed] [Google Scholar]
- 16.Tracey E, Roder D, Luke C, Bishop J. Bladder cancer survivals in New South Wales, Australia: Why do women have poorer survival than men? BJU Int. 2009;104:498–504. doi: 10.1111/j.1464-410X.2009.08527.x. [DOI] [PubMed] [Google Scholar]
- 17.Luke C, Tracey E, Stapleton A, Roder D. Exploring contrary trends in bladder cancer incidence, mortality and survival: Implications for research and cancer control. Intern Med J. 2010;40:357–62. doi: 10.1111/j.1445-5994.2009.01980.x. [DOI] [PubMed] [Google Scholar]
- 18.Rodriguez-Alonso A, Pita-Fernandez S, Gonzalez- Carrero J, Nogueira-March JL. Multivariate analysis of survival, recurrence, progression and development of mestastasis in T1 and T2a transitional cell bladder carcinoma. Cancer. 2002;94:1677–84. doi: 10.1002/cncr.10376. [DOI] [PubMed] [Google Scholar]
- 19.Farahmand M, Khademolhosseini F, Medhati M, Shokrpour N, Joulaei H, Mehrabani D. Trend of bladder cancer in Fars province, southern Iran, 2002-2006. [Persian] IRCMJ. 2009;11:470–2. [Google Scholar]
- 20.Moran A, Sowerbutts AM, Collins S, Clarke N, Cowan R. Bladder cancer: Worse survival in women from deprived areas. Br J Cancer. 2004;90:2142–4. doi: 10.1038/sj.bjc.6601847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Mathers CD, Boschi-Pinto C, Lopez AD, Murray C. Cancer incidence, mortality and survival by site for 14 regions of the world. WHO. 2001 [Google Scholar]
- 22.Hashibe M, Gao T, Li G, Dalbagni G, Zhang ZF. Comparison of bladder cancer survival among Japanese, Chinese, Filipino, Hawaiian and Caucasian populations in the United States. Asian Pac J Cancer Prev. 2003;4:267–73. [PubMed] [Google Scholar]
- 23.Manterola C, Vial M, Roa JC. Survival of a cohort of patients with intermediate and advanced gall bladder cancer treated with a prospective therapeutic protocol. Acta Cir Bras. 2010;25:225–30. doi: 10.1590/s0102-86502010000300003. [DOI] [PubMed] [Google Scholar]
- 24.Monzó Gardiner JI, Herranz Amo F, Díez Cordero JM, Cabello Benavente R, Silmi Moyano A, Hernández Fernández C. Prognostic factors for survival in patients with transitional bladder cancer treated with radical cystectomy. Spanish [Abstract] Actas Urol Esp. 2009;33:249–57. doi: 10.1016/s0210-4806(09)74138-5. [DOI] [PubMed] [Google Scholar]
- 25.Fairey AS, Jacobsen NE, Chetner MP, Mador DR, Metcalfe JB, Moore RB, et al. Associations between comorbidity, and overall survival and bladder cancer specific survival after radical cystectomy: Results from the Alberta urology institute radical cystectomy database. J Urol. 2009;182:85–92. doi: 10.1016/j.juro.2008.11.111. [DOI] [PubMed] [Google Scholar]
- 26.Gulliford MC, Petruckevitch A, Burney PG. Survival with bladder cancer, evaluation of delay in treatment, type of surgeon, and modality of treatment. BMJ. 1991;303:437–40. doi: 10.1136/bmj.303.6800.437. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Bellmunt J, Hautmann RE. Open to debate: The motion: Perioperative chemotherapy in muscle invasive bladder cancer improves survival. Eur Urol. 2008;54:1192–7. doi: 10.1016/j.eururo.2008.07.056. [DOI] [PubMed] [Google Scholar]
- 28.Rivera I, Wajsman Z. Bladder-sparing treatment of invasive bladder cancer. Cancer Causes Control. 2000;7:340–6. doi: 10.1177/107327480000700403. [DOI] [PubMed] [Google Scholar]
- 29.Ellis L, Rachet B, Shah A, Walters S, Coleman MP, Cooper N, et al. Trends in cancer survival in spearhead primary care trusts in England, 1998-2004. Health Stat Q. 2009:7–12. doi: 10.1057/hsq.2009.3. [DOI] [PubMed] [Google Scholar]
- 30.Lamm DL, Torti FM. Bladder cancer, 1996. CA Cancer J Clin. 1996;46:93–112. doi: 10.3322/canjclin.46.2.93. [DOI] [PubMed] [Google Scholar]