

Introduction
Lung cancer is the most common cancer worldwide. In the United States, it causes more cancer-related deaths than the next four causes (breast cancer, prostate cancer, colon cancer, and pancreatic cancer) of cancer-related mortality combined (1). About 30% of people have already progressed to stage III lung cancer and 40% to stage IV at the time they are diagnosed (2). Although chest X-ray and sputum cytology, when applied in health check-ups, can identify some relatively small tumors, they are not able to lower the overall mortality (3). More recently, the low-dose spiral CT scanning reduces the mortality of lung cancer when applied for lung cancer screening (4,5).
Along with the wider application of chest CT for lung cancer screening, an increasing number of small pulmonary masses can now be identified. About 40-60% of these small masses are primary lung cancer or lung metastases, for which surgical treatment is required. CT-guided biopsy is the common pathological approach before surgical treatment. For small lung cancer, however, the results of lung biopsy are not always reliable. Therefore, microscopic examination of frozen tissue sections is often performed firstly. Surgical decision (lobectomy and/or mediastinal lymph node dissection) is made based on the pathological findings (6).
We recently treated a patient with a small pulmonary nodule located in the central part of the left lower lobe. Upon the request of the patient, lobectomy and mediastinal lymph node dissection was not performed until the nodule was pathologically confirmed to be lung cancer.
Case report
A 60-year-old man was admitted due to “a mass in the left lower lobe of his lung during health check-up one week ago”. Routine blood test and tests for liver, kidney, heart, and lung functions at admission did not show any abnormal finding. Whole-body PET/CT showed that the mass was located at the middle part of the left lower lobe (Figure 1). It was 2.3 cm × 3.0 cm in size, with heterogeneous density and a maximum SUV value of 3.4. The patient was informed about his conditions and the need for surgical treatment. The patient agreed to receive surgical treatment, but requested that the pathology should be confirmed via lobectomy before the application of radical treatment. On July 7, 2012, he received surgical treatment under epidural anesthesia without endotracheal intubation. During the surgery, after the bronchi, arteries, and veins at the basilar segments of the left lower lobe were exposed and dissected, anatomical resection was performed for the basilar segments of the left lower lobe using Johnson & Johnson surgical stapler (Figure 2A). The specimen was immediately sent to the pathology department for frozen section, which reported “invasive adenocarcinoma” (Figure 2B). Then the arteries and veins at the dorsal segment of the left lower lung were separated and dissected, the root of the left lower lobe bronchus was dissected, and thus the left lower lobe was resected. After the dissection of the superior mediastinum, subcarinal, and inferior pulmonary ligament lymph nodes, and left upper mediastinal lymph nodes through an incision in the mediastinal pleura, the surgery was completed. During the 95-minute surgery, the intra-operative blood loss was 100 mL. A chest tube was placed for the first 48 hours post surgery. Eleven lymph nodes were removed, and metastasis was found in station 10 (2/5). The post-operative recovery was smooth. He was discharged on the 5th post-operative day.
Figure 1.

PET/CT shows the mass is located at the central part of the left lower lobe
Figure 2.
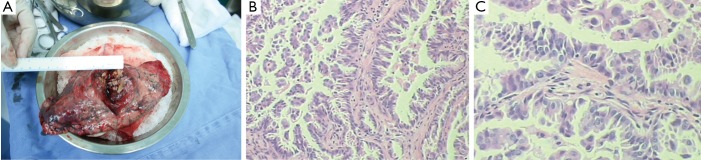
Anatomical resection of the basilar segments of the left lower lobe and the mass at the central part (A); the mass is pathologically confirmed as adenocarcinoma (B,C)
Discussion
An increasing number of small lung nodules have been detected along with the application of chest CT for health check-ups (4,5). It has been found that about 0.2% of small lung nodules were detected by low-dose CT, although 40-60% of these nodules can be malignant (7). Also, as confirmed by pathological examinations, about half (53.6%) of the small pulmonary masses found during health check-ups can be primary lung cancer and pulmonary metastases (6), and the prognosis is directly related with the sizes of these masses (8,9). However, a definitive diagnosis usually can not be made by pre-operative bronchoscopy, percutaneous lung biopsy, or PET, and timely surgical treatment is essential for these patients.
Before the surgery, marking of the mass is useful for localizing the mass intraoperatively and for mass resection for biopsy (10-12). Currently the most common methods for pre-operative localization include percutaneous placement of annular metal ring, percutaneous methylene blue injection, and transbronchial ultralocalization (13-15). However, these methods are often associated with high incidences of complications and high failure rate. In another study, patients with small pulmonary nodules underwent injection of a solution composed of [99] Tc-labeled human serum albumin microspheres into the nodule. During the surgery, the area of major radioactivity was resected. However, drug leakage and localization failure still occurred; meanwhile, due to the rapid decay of the radioactive element, reasonable control of the injection time is also a challenging task (6). In our patient, since the mass was deep inside the lobe, it is impossible to localize it.
For patients with small pulmonary nodules detected during health check-up, video-assisted thoracoscopic surgery (VATS) resection is a good option (7,16). In fact, since the introduction of VATS in our department in 1994, VATS has been applied for the surgical treatment of many chest diseases. VATS assisted small incision surgery can be used for more complicated sleeve pneumonectomy (17-19). In our current patient, pulmonary wedge resection was difficult because the mass was located at the central part of the left lower lobe. Since the pre-operative pathology was unclear, it would be unwise to perform lobectomy if the mass turned out to be benign. A better option is: segmentectomy is performed firstly, and the following procedure is decided on the basis of the pathological findings.
Acknowledgements
Disclosure: The authors declare no conflict of interest.
References
- 1.Jemal A, Siegel R, Xu J, et al. Cancer statistics, 2010. CA Cancer J Clin 2010;60:277-300 [DOI] [PubMed] [Google Scholar]
- 2.Ellis PM, Vandermeer R. Delays in the diagnosis of lung cancer. J Thorac Dis 2011;3:183-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wong MP. Circulating tumor cells as lung cancer biomarkers. J Thorac Dis 2012;4:631-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bach PB, Mirkin JN, Oliver TK, et al. Benefits and harms of CT screening for lung cancer: a systematic review. JAMA 2012;307:2418-29 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.National Lung Screening Trial Research Team , Aberle DR, Adams AM, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med 2011;365:395-409 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ambrogi MC, Melfi F, Zirafa C, et al. Radio-guided thoracoscopic surgery (RGTS) of small pulmonary nodules. Surg Endosc 2012;26:914-9 [DOI] [PubMed] [Google Scholar]
- 7.Henzler T, Shi J, Hashim Jafarov, et al. Functional CT imaging techniques for the assessment of angiogenesis in lung cancer. Transl Lung Cancer Res 2012;1:78-83 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Birim O, Kappetein AP, Takkenberg JJ, et al. Survival after pathological stage IA nonsmall cell lung cancer: tumor size matters. Ann Thorac Surg 2005;79:1137-41 [DOI] [PubMed] [Google Scholar]
- 9.Port JL, Kent MS, Korst RJ, et al. Tumor size predicts survival within stage IA non-small cell lung cancer. Chest 2003;124:1828-33 [DOI] [PubMed] [Google Scholar]
- 10.Kothary N, Lock L, Sze DY, et al. Computed tomography-guided percutaneous needle biopsy of pulmonary nodules: impact of nodule size on diagnostic accuracy. Clin Lung Cancer 2009;10:360-3 [DOI] [PubMed] [Google Scholar]
- 11.Rivera MP, Mehta AC, American College of Chest Physicians. Initial diagnosis of lung cancer: ACCP evidence-based clinical practice guidelines (2nd edition). Chest 2007;132:131S-148S. [DOI] [PubMed] [Google Scholar]
- 12.Kozower BD, Meyers BF, Reed CE, et al. Does positron emission tomography prevent nontherapeutic pulmonary resections for clinical stage IA lung cancer? Ann Thorac Surg 2008;85:1166-9; discussion 1169-70 [DOI] [PubMed] [Google Scholar]
- 13.Santambrogio R, Montorsi M, Bianchi P, et al. Intraoperative ultrasound during thoracoscopic procedures for solitary pulmonary nodules. Ann Thorac Surg 1999;68:218-22 [DOI] [PubMed] [Google Scholar]
- 14.Mack MJ, Gordon MJ, Postma TW, et al. Percutaneous localization of pulmonary nodules for thoracoscopic lung resection. Ann Thorac Surg 1992;53:1123-4 [DOI] [PubMed] [Google Scholar]
- 15.Wicky S, Mayor B, Cuttat JF, et al. CT-guided localizations of pulmonary nodules with methylene blue injections for thoracoscopic resections. Chest 1994;106:1326-8 [DOI] [PubMed] [Google Scholar]
- 16.Cao C, Manganas C, Ang SC, et al. A meta-analysis of unmatched and matched patients comparing video-assisted thoracoscopic lobectomy and conventional open lobectomy. Ann Cardiothorac Surg 2012;1:16-23 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Richards JM, Dunning J, Oparka J, et al. Video-assisted thoracoscopic lobectomy: The Edinburgh posterior approach. Ann Cardiothorac Surg 2012;1:61-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hansen HJ, Petersen RH. Video-assisted thoracoscopic lobectomy using a standardized three-port anterior approach - The Copenhagen experience. Ann Cardiothorac Surg 2012;1:70-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hennon MW, Demmy TL. Video-assisted thoracoscopic surgery (VATS) for locally advanced lung cancer. Ann Cardiothorac Surg 2012;1:37-42 [DOI] [PMC free article] [PubMed] [Google Scholar]