

Abstract
We report a case of altered mental status secondary to acute Toxoplasma Gondii encephalitis. The patient had no medical or surgical history and presented with acute onset of lethargy with no clear precipitant. A physical exam revealed no focal neurological deficits and a subsequent medical workup revealed multiple intracranial lesions with a biopsy confirming the diagnosis of Toxoplasma Gondii encephalitis in the setting of newly diagnosed human immunodeficiency virus (HIV). A literature review revealed that this is a unique case of toxoplasmic encephalopathy in the United States in a previously undiagnosed HIV positive patient presenting to an emergency department.
A 33-year-old Yemenese male presented to the emergency department (ED) accompanied by family members who relayed a 2-day history of fever, headaches, nausea, vomiting, and confusion. The patient had increased sleepiness and progressive mental status changes over the preceding 48 hours, and the family had noted that he had become more disoriented and lethargic in nature.
There was no reported medical or surgical history, although the patient was recently treated as an outpatient for community-acquired pneumonia. The patient and present family members denied any history of depression, drug use, sick contacts, or trauma. The patient had resided in the United States for the past 10 years and had not traveled outside of the country in that time.
On physical examination the patient was afebrile with normal vitals. The patient would respond “yes” or “no” to questions, but would not speak in complete sentences. The Glasgow Coma Scale (GCS) was 13, with points subtracted for opening his eyes to only pain. Physical exam revealed white plaques in the intra-oral cavity. A focused neurologic exam, to the best of the patient’s ability to cooperate, revealed no focal deficits. The patient’s cranial nerves were intact and he was moving all extremities with no noted weakness or decrease in sensation. His reflexes were normal and there was no ataxia present. Other systems, including cardiac, respiratory, abdominal, and genitourinary examination, were normal.
A differential diagnosis for the patient’s presentation included concern for drug or alcohol intoxication, endocrine abnormalities, central nervous system (CNS) infection, toxic ingestion, sepsis, ischemic or hemorrhagic stroke, uremia, and CNS tumors.
Laboratory tests revealed normal blood glucose, negative urine drug screen, normal electrolytes, and normal complete blood count. Additionally, a blood alcohol was negative, as well as a urine toxicology screen, and the patient had a normal anion gap and osmolar gap. A head computerized tomography (CT) was obtained (Figure 1). The CT showed multiple areas of vasogenic edema involving the supratentorial brain parenchyma with the largest of these involving the left anterior/inferior frontal lobe, right parietal lobe, left thalamus, right frontal and temporal lobe and right perisylvian region. There was also noted mass effect on the left frontal horn and right temporal horn and for this reason a lumbar puncture was not performed in the ED. Urgent magnetic resonance imaging of the head was obtained with gadolinium, which demonstrated multiple solid and irregular rim enhancing lesions with surrounding vasogenic edema (Figure 2).
Figure 1.
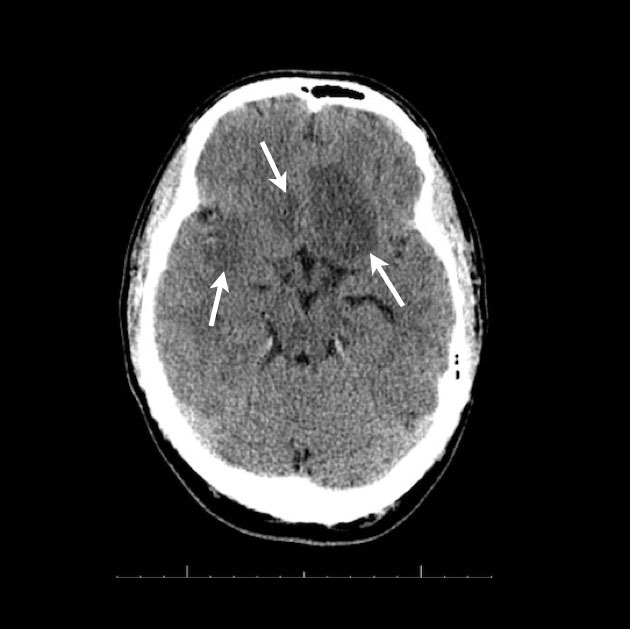
Head computed tomography of patient demonstrating areas of intracerebral vasogenic edema (arrows).
Figure 2.

Magnetic resonance imaging with gadolinium with multiple enhancing lesions (arrows).
The patient was taken by neurosurgery service to the operating room where a biopsy was taken, which was positive for Toxoplasmosis gondii. The patient was then found to be positive for the human immunodeficiency virus (HIV) with subsequent testing. While in the intensive care unit the patient required mannitol, steroids, and hypertonic saline for cerebral edema, and his neurologic status improved with treatment. The patient was treated for cerebral toxoplasmosis, subsequent Pneumocystis carini pneumonia, oral thrush, and was started on highly active anti-retroviral therapy (HAART).
Toxoplasmosis gondii is an opportunistic intracellular pathogen that has long been recognized as the most frequent cause of brain lesions in acquired immune deficiency syndrome (AIDS) patients.1,2 Seroprevalence of Toxoplasmosis gondii is estimated at 22.5% within the United States (U.S.) and may be higher within the general populous in Europe and tropical countries.3,4 Infection with Toxoplasmosis gondii in adults with normal immune function will normally be asymptomatic or cause mild complaints of fever or malaise, while in the immunocompromised host it can cause severe central nervous system infections. Up to 10% of newly diagnosed AIDS patients can present with neurologic toxoplasmosis with the classic finding on head CT of a ring-enhancing lesion.5 In the days prior to HAART treatment and rapid human HIV testing, up to 10–20% of newly diagnosed HIV patients presented with neurologic disease.6
A review of the literature shows that this is a unique case of toxoplasmic encephalopathy in the U.S. in a previously undiagnosed HIV positive patient presenting to an ED. Garcia-Gubern et al7 noted a case of toxoplasmic encephalopathy of the spinal cord; however, it was different than our case because the patient had focal neurologic deficits of the lower extremities. Lee et al8 relate a case of cerebral and optic nerve toxoplasmosis in an undiagnosed HIV positive patient, but this case differs in that the patient had neurologic symptoms manifested by vision loss. In a case reported by Snyder9, a 27-year-old male was diagnosed with CNS toxoplasmosis, although the patient was exhibiting right-sided weakness and had known risk factors associated with the acquisition of HIV. Jayawardena et al10 reported a case of a 35-year-old female with cerebral toxoplasmosis, but the patient was already known to be HIV positive. Therefore, this is the first published case report of toxoplasmic encephalopathy in a previously undiagnosed HIV positive patient presenting to an ED with altered mental status without focal neurological deficits and no known risk factors associated with the acquisition of HIV.
Footnotes
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
- 1.Luft BJ, Remington JS. Toxoplasmic encephalitis in AIDS. Clinical Infectious Diseases. 1992;15:211–222. doi: 10.1093/clinids/15.2.211. [DOI] [PubMed] [Google Scholar]
- 2.Rothman RE, Marco CA, Yang S. Chapter 149. Human Immunodeficiency Virus infection and Acquired Immunodeficiency Syndrome. In: Tintinalli JE, Stapczynski JS, Cline DM, Ma OJ, Cydulka RK, Meckler GD, et al., editors. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York: McGraw-Hill; 2011. Available at: http://www.accessmedicine.com/content.aspx?aID=6365597. Accessed March 20, 2012. [Google Scholar]
- 3.Jones JL, Kruszon-Moran D, Wilson M, et al. Toxoplasma gondii infection in the United States: seroprevalence. American Journal or Epidemiology. 2001;154:357–365. doi: 10.1093/aje/154.4.357. [DOI] [PubMed] [Google Scholar]
- 4.Vidal J, Hernandez AV, Penalva De Oliveira AC, et al. Cerebral toxoplasmosis in HIV-positive patients in Brazil: clinical features and predictors of treatment response in the HAART era. AIDS Patient Care & Stds. 2005;19(10):626–634. doi: 10.1089/apc.2005.19.626. [DOI] [PubMed] [Google Scholar]
- 5.Levy RM, Rosenbloom S, Perrett LV. Neuroradiologic findings in AIDS: a review of 200 cases. American Journal of Roentgenology. 1986;147:977–983. doi: 10.2214/ajr.147.5.977. [DOI] [PubMed] [Google Scholar]
- 6.Berger JR, Moskowitz L, Margaret F, et al. Neurologic disease as the presenting manifestation of Acquired Immunodeficiency Syndrome. Southern Medical Journal. 1987;80:683–686. doi: 10.1097/00007611-198706000-00004. [DOI] [PubMed] [Google Scholar]
- 7.Garcia-Gubern C, Fuentes CR, Colon-Rolon L, et al. Spinal cord toxoplasmosis as an unusual presentation of AIDS: case report and review of the literature. International Journal of Emergency Medicine. 2010;3:439–442. doi: 10.1007/s12245-010-0207-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lee MW, Fong KS, Hsu LY, et al. Optic nerve toxoplasmosis and orbital inflammation as initial presentation of AIDS. Graefe’s Archive for Clinical an Experimental Ophthalmology. 2006;244:1542–1544. doi: 10.1007/s00417-006-0295-5. [DOI] [PubMed] [Google Scholar]
- 9.Snyder Howard. CNS toxoplasmosis as the initial presentation of the Acquired Immunodeficiency Syndrome. American Journal of Emergency Medicine. 1989. Nevember. pp. 588–592. [DOI] [PubMed]
- 10.Jayawardena S, Singh S, Burzyantseva O, et al. Cerebral toxoplasmosis in adult patients with HIV infection. Hospital Physician. 2008 Jul 17–24; [Google Scholar]