

Abstract
Context
Prior research suggests that drug abuse (DA) is strongly influenced by both genetic and familial environmental factors. No large-scale adoption study has previously attempted to verify and integrate these findings.
Objective
To determine how genetic and environmental factors contribute to the risk for DA.
Design
Follow-up in 9 public databases (1961–2009) of adopted children and their biological and adoptive relatives.
Setting
Sweden.
Participants
The study included 18 115 adopted children born between 1950 and 1993; 78 079 biological parents and siblings; and 51 208 adoptive parents and siblings.
Main Outcome Measures
Drug abuse recorded in medical, legal, or pharmacy registry records.
Results
Risk for DA was significantly elevated in the adopted offspring of biological parents with DA (odds ratio, 2.09; 95% CI, 1.66–2.62), in biological full and half siblings of adopted children with DA (odds ratio, 1.84; 95% CI, 1.28–2.64; and odds ratio, 1.41; 95% CI, 1.19–1.67, respectively), and in adoptive siblings of adopted children with DA (odds ratio, 1.95; 95% CI, 1.43–2.65). A genetic risk index (including biological parental or sibling history of DA, criminal activity, and psychiatric or alcohol problems) and an environmental risk index (including adoptive parental history of divorce, death, criminal activity, and alcohol problems, as well as an adoptive sibling history of DA and psychiatric or alcohol problems) both strongly predicted the risk for DA. Including both indices along with sex and age at adoption in a predictive model revealed a significant positive interaction between the genetic and environmental risk indices.
Conclusions
Drug abuse is an etiologically complex syndrome strongly influenced by a diverse set of genetic risk factors reflecting a specific liability to DA, by a vulnerability to other externalizing disorders, and by a range of environmental factors reflecting marital instability, as well as psychopathology and criminal behavior in the adoptive home. Adverse environmental effects on DA are more pathogenic in individuals with high levels of genetic risk. These results should be interpreted in the context of limitations of the diagnosis of DA from registries.
The abuse of illicit psychoactive substances is a major worldwide public health problem.1 Because familial factors contribute strongly to the risk for drug abuse (DA),2–4 much effort has gone into understanding the nature of these influences.
Twin studies have shown the substantial role genetic factors play in the etiology of DA5–9 and others5,8,9 have also shown an impact of the shared family environment. Developmental and epidemiologic studies show that numerous aspects of family functioning correlate with risk for substance use and subsequent DA in off-spring including low socioeconomic status, parental divorce or death, parental history of DA, parental criminal behavior and/or psychopathology, and disrupted family functioning.10–14 However, these studies are typically performed in intact families where relatives share genes and environment, making it impossible to determine whether these aspects of familial dysfunction directly cause DA or reflect susceptibilities in parents that are transmitted genetically to their offspring.
These questions can be addressed in an adoption design where information on DA and associated risk factors are available on adopted children and their biological and adoptive relatives. To our knowledge, ours is the first large-scale adoption study of DA performed in a national adoption sample from Sweden. We seek to clarify the nature of the genetic and familial environmental risk factors for DA and the interaction between them.
METHODS
To assess DA among Swedish adopted children and their relatives, we linked comprehensive registry and health care data from multiple nationwide sources to form a DA database. This linking was based on the Swedish unique individual 10-digit personal identification number that is nearly 100% complete and assigned at birth for all Swedish residents for their lifetime. This number was replaced by a serial number to provide anonymity. Our database contained 9 sources:
The Swedish Hospital Discharge Register included all hospitalizations (including for DA) for all people in Sweden from 1964 to 2009. Every record has the main discharge diagnosis and 8 secondary diagnoses.
The Swedish Prescribed Drug Register included all prescriptions in Sweden picked up by patients from 2005 to 2009. It is complete as all prescriptions are registered at the National Board of Health and Welfare.
The Swedish Mortality Register contained all causes of death and time of death from 1961 to 2009.
The National Censuses provided information on education and marital status in 1960, 1970, 1980, and 1990.
The Total Population Registry included annual data on education and marital status from 1990 to 2009.
The Multi-Generation Register provided information on family relationships from 1932 to 2009 including all adoptions and adoptive and biological parents and siblings. Biological siblings reared with the adopted child were excluded.
The Outpatient Care Register included information from all outpatient clinics in Sweden from 2001 to 2009.
The Primary Health Care Register included outpatient care data on diagnoses and time for diagnoses from 2001 to 2007 for 1 million patients from Stockholm and middle Sweden.
The Swedish Crime Register included national complete data on all convictions including those for DA from 1973 to 2007.
This study was approved by the ethics committee of Lund University in Malmö, Sweden.
SAMPLE
The study population consisted of individuals born between 1950 and 1993 who had been adopted, with information available on both adoptive parents and at least 1 biological parent. Individuals adopted by biological relatives or by an adoptive parent living with a biological parent were excluded. Age at formal adoption was not available in national records until 1991. Therefore, we estimated age at first cohabitation with adoptive parents (AFCAP) from census data including individual addresses available every 5 years (eg, 1950, 1955, 1960, etc). For an adopted child born in 1961 and living with adoptive parents in the 1965 census, AFCAP was calculated as 4 years, although it could have been from 0 to 4 years. Thus, AFCAP represents an upper limit of true age at adoption. We constructed 2 cohorts with maximal AFCAPs of 5 years (n=12 783) and 10 years (n=18 115), and we performed all analyses in parallel. To maximize statistical power, we present results on the entire cohort.
OUTCOME VARIABLE
Drug abuse was operationalized in this study using a range of Swedish registries. We identified DA in the Swedish hospital discharge, mortality, primary care, and outpatient care registers with the following codes from the eighth, ninth, and tenth revisions of the International Classification of Disease: ICD-8 codes for drug dependence (304); ICD-9 codes for drug psychoses (292) and drug dependence (304); and ICD-10 codes for mental and behavioral disorders due to psychoactive substance use (F10–F19), except those due to alcohol (F10) or tobacco (F17).
Drug abuse was also identified in the Crime Register by codes 5011 and 5012, which reflect crimes related to DA. Crimes related only to alcohol abuse or to trafficking in or possession of drugs of abuse were excluded. Plea bargains in Sweden only occur with minor offenses. An arrest for serious offenses including drug-related crimes routinely leads to prosecution. The Crime Register includes only criminal convictions that occur in general courts in Sweden. Minor offenses that typically do not go to these courts such as traffic and parking violations were not included.
Drug abuse was identified in individuals in the Prescribed Drug Register who had retrieved (on average) more than 4 daily doses for 12 months of hypnotics and sedatives (Anatomical Therapeutic Chemical Classification System codes N05C and N05BA) or opioids (Anatomical Therapeutic Chemical Classification System code N02A). Patients with cancer were excluded.
The 820 unique cases of DA in our cohort came from the following registries: Discharge (n=527), Crime (n=313), Out-patient (n=264), Prescribed Drugs (n=118), and Primary Health Care (n=8). No unique cases of DA were identified through the Mortality Register. Table 1 shows the odds ratios (ORs) and 95% confidence intervals for the ascertainment of DA among these 5 sources. Odds ratios ranged from a low of 5.6 between the Prescription and Crime Registers to a high of 118.0 between the Discharge and Outpatient Registers.
Table 1.
Registration of Drug Abuse Between the 5 Registers Used in the Study
| Odds Ratio (95% CI) |
||||
|---|---|---|---|---|
| Hospital Discharge | Outpatient | Primary Health Care | Drug Prescription | |
| Crime | 32.9 (32.2–33.4) | 65.2 (63.9–66.5) | 47.4 (41.8–53.7) | 5.6 (5.3–5.9) |
| Hospital discharge | 118.0 (115.7–120.4) | 69.8 (61.8–78.7) | 20.9 (20.2–21.7) | |
| Outpatient | 94.4 (83.5–106.8) | 29.6 (28.5–30.8) | ||
| Primary health care | 37.9 (30.9–46.4) | |||
Misidentification of paternity was expected to be rare in our sample. Since 1958, all children born in Sweden must have a registered father. A public declaration of paternity is required and if there is uncertainty, blood tests for traditional genotyping (or after 1993, DNA testing) are required.
GENETIC RISK SCORE
We used the following variables in biological parents and/or biological siblings, measured during the entire life course: DA, hospitalization owing to alcoholism (identified in the Swedish Hospital Discharge Register according to the following codes: ICD-8 codes for alcoholism [303] and alcoholic psychosis [291]; ICD-9 codes for alcoholic psychoses [291] and alcohol dependence syndrome [303]; and ICD-10 codes for mental and behavioral disorders owing to the use of alcohol [F10]); hospitalization owing to psychiatric illness (identified in the Swedish Hospital Discharge Register according to the following codes: ICD-8 codes 295–302 and 305–307; ICD-9 codes 295–298, 300–302, 306–309, 311, and312; and ICD-10 codes F20–F25, F28–F34, F38–F45, F48, F50–F54, F59–F69, and F99); and criminality (ever identified in the Swedish Crime Register). Among parents, at least 1 parent had to be defined according to the criteria just described. For siblings, we created a weighted score from the number of full and half siblings, with the former weighted twice as much as the latter to reflect their genetic relatedness to the adopted child.
In parents, we considered educational attainment as a proxy for socioeconomic status. To control for cohort effects, we defined low- and high-educational attainment as less than or greater than the 75th percentile of the distribution of years of education in the appropriate decade of birth for the entire Swedish population. We also considered divorces among biological mothers (if there was no biological mother identified or the marital status for the mother was missing, then the father's status was used) during their entire life. Finally, we considered the mother's age at birth. If a mother's age was missing, the biological father's age was used.
ENVIRONMENTAL RISK SCORE
A broad array of factors reflecting dysfunction in the family of origin increase the risk for subsequent use and abuse of illicit substances.10–15 Therefore, we used a range of available variables in adoptive parents from first cohabitation with adoptive parents until the adopted child was aged 20 years to index potential environmental risk: DA, hospitalization owing to alcoholism, criminality, and divorce. We added hospitalization for any medical problem and psychiatric illness (from the Swedish Hospital Register) and death (from the Mortality Register). We also considered education as a proxy for socioeconomic status, using the highest education of the adoptive mother or father. We also considered the age of the adoptive mother at the time of adoption.
The following variables, which were chosen to reflect both general family dysfunction and possible exposure for the siblings in the household to deviant peer networks, were considered among adoptive siblings and were measured during their entire life: DA; hospitalization owing to alcoholism, psychiatric illness, or other medical problems; and criminality. We created a score weighted according to the number of siblings.
ENVIRONMENTAL AND GENETIC RISK SCORES
We performed a logistic regression on the entire sample of 18 115 adopted children and modeled DA as a function of numerous factors associated with an increased risk for DA. All variables linked with biological parents/siblings and associated with DA (P<.10) in univariate analyses were included in the genetic risk score. When 2 predictors were strongly correlated, 1 was excluded from the model. Finally, we obtained the predicted probabilities (ie, genetic risk scores) for each adopted child and categorized them into 10 groups by deciles and used these variables as continuous variables in the final analysis. The same procedure was performed for all variables linked with adoptive parents/siblings to create an environmental risk score.
STATISTICAL ANALYSIS
Our key dependent variable, DA, is dichotomous. We initially used logistic regression and modeled DA as a function of the genetic risk score, the environmental risk score, sex of the adopted child, and AFCAP. However, a key a priori goal of these analyses was to determine whether genetic and environmental risk factors interacted in the etiology of DA. We have previously argued that the scale of raw probabilities, rather than the logistic scale, is more appropriate for such analyses.16 Therefore, for our analyses of gene × environment interaction, we used SAS Proc GENMOD (SAS Institute)17 with the identity link and we specified the variance to be binomial. We specified the effects of the explanatory variables (and the interaction term) to be additive on the scale of probabilities. All P values are reported as 2-tailed.
RESULTS
GENERAL DESCRIPTION
The general characteristics of our study sample are outlined in Table 2. In the 18 115 adopted children, whose average (SD) age at last available information was 46.2 (8.5) years, the prevalence of DA was 4.5% (95% CI, 4.2–4.8) compared with 2.9% in all of Sweden from the same birth years. Compared with their adoptive parents, the biological parents had higher rates of DA, hospitalization for psychiatric illness and alcoholism, criminal convictions, low education, and divorce. Similar differences were seen between the adoptive and biological full and half siblings of the adopted children. The mean AFCAP was 4.4 years.
Table 2.
Descriptive Statistics for Adopted Children and Biological and Adoptive Relatives
| % |
||||||
|---|---|---|---|---|---|---|
| Biological Parents | Adoptive Parents | Biological Full Siblings | Biological Half Siblings | Adoptive Siblings | Adopted Child | |
| Adopted children with at least 1 of this type of relative, No. | 18 115 | 18 115 | 3524 | 14 884 | 8597 | 18 115 |
| Relatives with information, No. | 27 241 | 36 230 | 7301 | 43 537 | 14 978 | |
| Drug abuse | 5.8 | 1.0 | 6.3 | 5.4 | 3.4 | 4.5 |
| Adoptive child's sex (male) | 52.2 | |||||
| Hospitalization owing to psychiatric disease | 18.8 | 3.1 | 19.0 | 20.8 | 8.4 | |
| Hospitalization owing to alcoholism | 15.9 | 0.9 | 11.6 | 10.6 | 3.7 | |
| Convictions | 41.3 | 9.4 | 61.3 | 62.8 | 36.8 | |
| Maternal age, mean, y | 24.4 | 37.5 | ||||
| Maternal divorce | 38.7 | 6.8 | ||||
| Education | ||||||
| High (≥75th percentile) | 23.5 | 57.2 | ||||
| Low (<75th percentile) | 76.5 | 42.8 | ||||
We examined the prevalence of DA as defined in this study by decade of birth (ie, 1950–59, 1960–69, 1970–79, and 1980–1993). In the entire Swedish population, this varied slightly, with no monotonic trends, between 2.8% and 3.1%. However, among the adopted children, prevalence rates of DA increased consistently across these 4 cohorts: 4.1%, 4.6%, 5.0%, and 6.5%. Therefore, we controlled for year of birth in all subsequent analyses.
DRUG ABUSE IN BIOLOGICAL AND ADOPTIVE RELATIVES OF PARENTS AND ADOPTED CHILDREN WITH DA
The risk for DA among children given for adoption by biological parents, at least 1 of whom had DA, was 8.6%, which was substantially and significantly elevated over that seen in children given for adoption when neither biological parent had DA (4.2%)(Table 3) (OR, 2.09; 95% CI, 1.66–2.62; ; P<.001). Among adopted children, those who had none, 1, and both biological parents with DA had a prevalence of DA of 4.2%, 8.2%, and 11.9%, respectively (; P<.001). The risk for DA among adopted children of biological fathers and mothers with DA was 9.9% and 8.2%, respectively. The risk for DA was increased in both biological full siblings and biological half siblings of adopted children with DA (10.7% and 7.4%, respectively) vs without DA (6.1% and 5.3%, respectively) (OR, 1.84; 95% CI, 1.28–2.64; ; P<.001; and OR, 1.41; 95% CI, 1.19–1.67; ; P=.001, respectively).
Table 3.
Rates of Drug Abuse in Adopted Children of Biological Parents, Adoptive Offspring of Adoptive Parents, and Biological and Adoptive Siblings of Adopted Children With and Without Drug Abuse
| % (95% CI) |
|||
|---|---|---|---|
| Proband | Relative | Rate of Drug Abuse in Relative When Proband Has Drug Abuse | Rate of Drug Abuse in Relative When Proband Does Not Have Drug Abuse |
| Biological parent (any) | Adopted away biological offspring | 8.6 (7.0–10.4) | 4.2 (4.0–4.6) |
| Biological father | Adopted away biological offspring | 9.9 (7.2–12.1) | 4.4 (4.1–4.7) |
| Biological mother | Adopted away biological offspring | 8.2 (6.3–10.5) | 4.4 (4.1–4.7) |
| Adoptive parent (any) | Adoptive offspring | 6.8 (3.6–11.6) | 4.5 (4.2–4.8) |
| Adopted child | Biological full sibling | 10.7 (7.6–14.5) | 6.1 (5.6–6.7) |
| Adopted child | Biological half sibling | 7.4 (6.3–8.5) | 5.3 (5.1–5.5) |
| Adopted child | Adoptive sibling | 6.2 (4.5–8.1) | 3.2 (3.0–3.5) |
The risk for DA in adopted children raised by 1 or more adoptive parents with vs without DA was not significantly increased (6.8% vs 4.5%; OR, 1.55, 95% CI, 0.86–2.80; ; P=.15). However, adoptive siblings of adopted children with vs without DA had a significantly increased risk for DA (6.2% vs 3.2%; OR, 1.95; 95% CI, 1.43–2.65; ; P<.001).
PREDICTORS OF GENETIC AND ENVIRONMENTAL RISK FOR DA AND THEIR INTERRELATIONSHIP
We created indices of genetic and environmental risks for DA from available characteristics of the adopted children's biological parents and siblings and their adoptive parents and siblings. As seen in Table 2, genetic risk for DA in the adopted child was indexed by a range of features including biological parental low-educational attainment and divorce, and a parental or sibling history of DA, criminal activity, and treatment for psychiatric or alcohol problems. Environmental risk for DA was predicted by a diverse set of characteristics including an adoptive parental history of divorce, premature death, criminal activity, and hospitalization for medical or alcohol problems, and an adoptive sibling history of DA and hospitalization for psychiatric, alcohol, or medical problems.
Examined individually in logistic regression (Table 4), where the genetic and environmental risk indices were divided into 10 deciles, both risk scores were strongly predictive of DA: OR (per decile), 1.13 and 1.10, respectively. Thus, the ORs for DA between individuals at the lowest and highest decile of genetic and environmental risk equal 1.1310 or 3.39 and 1.1010 or 2.59, respectively. The correlation between risk scores was small (plus 0.11) but significant (P<.001). Examined individually, DA in adopted children was also significantly predicted by male sex, younger AFCAP, and a later birth year.
Table 4.
Creation of Genetic and Environmental Risk Scores for Adopted Children
| Odds Ratio (95% CI) |
||||
|---|---|---|---|---|
| Adaptive Relations (Environmental Risk Score) |
Biological Relations (Genetic Risk Score) |
|||
| Univariate Analyses | Multivariate Analysis | Univariate Analyses | Multivariate Analysis | |
| Parents | ||||
| Drug abuse | 1.55 (0.86–2.80) | 2.09 (1.66–2.63)a | 1.44 (1.11–1.85)b | |
| Psychiatric disease | 1.25 (0.86–1.80) | 1.58 (1.34–1.85)a | 1.26 (1.06–1.50)b | |
| Alcoholism | 1.89 (1.09–3.29)c | 1.33 (0.76–2.36) | 1.76 (1.49–2.08)a | 1.36 (1.13–1.64)b |
| Convictions | 1.42 (1.15–1.76)b | 1.25 (1.00–1.56)c | 1.49 (1.30–1.72)a | 1.22 (1.04–1.42)b |
| Maternal age | 0.97 (0.96–0.98)a | 0.98 (0.97–0.99)a | 0.99 (0.98–1.00)d | 0.99 (0.98–1.00) |
| Maternal divorce | 1.51 (1.19–1.92)a | 1.31 (1.03–1.68)c | 1.24 (1.08–1.43)b | 1.15 (1.00–1.33)d |
| Education (low vs high) | 0.92 (0.80–1.06) | 1.29 (1.08–1.54)b | 1.19 (1.00–1.43)d | |
| Medical hospitalization | 1.30 (1.13–1.50)a | 1.17 (1.01–1.35)c | ||
| Death | 1.29 (1.02–1.63)c | 1.37 (1.08–1.73)b | ||
| Siblings | ||||
| Drug abuse | 2.29 (1.61–3.27)a | 1.76 (1.16–2.67)b | 1.66 (1.05–2.61)c | 1.02 (0.60–1.72) |
| Psychiatric disease | 1.57 (1.16–2.11)b | 1.16 (0.83–1.62) | 1.65 (1.13–2.41)b | 1.31 (0.86–1.99) |
| Alcoholism | 1.89 (1.26–2.84)b | 1.27 (0.80–2.01) | 1.65 (1.01–2.72)c | 1.28 (0.73–2.24) |
| Convictions | 0.99 (0.85–1.14) | 1.21 (0.95–1.55) | ||
| Medical hospitalization | 1.25 (1.09–1.44)b | 1.12 (0.97–1.30) | ||
P < .001.
P < .01.
P < .05.
P < .10.
Next, we examined the genetic and environmental indices jointly with sex, AFCAP, and birth year (Table 5). The predictive power of both indices declined slightly as would be expected given their low intercorrelation. Sex remained predictive but not AFCAP or birth year.
Table 5.
Prediction of Drug Abuse in Adopted Children From the Genetic and Environmental Risk Scores by Logistic Regression Analysis
| Odds Ratio (95% CI) |
||
|---|---|---|
| Univariate Analysis | Multivariate Analysisa | |
| Genetic risk score | 1.13 (1.10–1.16)b | 1.12 (1.09–1.15)b |
| Environmental risk score | 1.10 (1.07–1.12)b | 1.09 (1.06–1.12)b |
| Sex of adopted child (male vs female) | 1.45 (1.26–1.67)b | 1.44 (1.24–1.66)b |
| AFCAP from census data | 0.96 (0.93–0.98)c | 1.00 (0.96–1.02) |
| Birth year of adopted child | 1.02 (1.01–1.02)c | 0.99 (0.98–1.00) |
Abbreviation: AFCAP, age at first cohabitation with adoptive parents.
Multivariate model includes adopted children's genetic and environmental risk scores, sex, AFCAP, and birth year.
P < .001.
P < .01.
We then explored whether the sexes differed in their sensitivity to genetic or environmental risk factors. Adding these interactions one at a time to the model depicted in Table 4 showed no significant interaction between sex and environmental risk (P=.91), but there was modest evidence that males were more sensitive to the impact of genetic risk factors for DA (P=.03).
Finally, we analyzed these predictor variables on the scale of raw probabilities without and with an interaction between the genetic and environmental risk scores (Table 6). The interaction was significant, showing that the impact of an adverse environment on risk for DA was substantially greater in those with a high vs low genetic liability to DA (Figure).
Table 6.
Prediction of Drug Abuse Among Adopted Children From the Genetic and Environmental Risk Scores and Their Interaction on the Scale of Raw Probabilities
| Beta (95% CI) |
||
|---|---|---|
| Multivariale Analysis Without an Interaction Term | Multivariate Analysis With an Interaction Term | |
| Genetic risk score | 0.0049 (0.0038 to 0.0060)a | 0.0028 (0.0010 to 0.0048)b |
| Environmental risk score | 0.0036 (0.0024 to 0.0048)a | 0.0015 (−0.0006 to 0.0036) |
| Sex adoptive child (male vs female) | 0.0151 (0.0091 to 0.0212)a | 0.0152 (0.0091 to 0.0213)a |
| AFCAP from census data | −0.0003 (−0.0017 to 0.0010) | −0.0005 (−0.0018 to 0.0009) |
| Birth year of adopted child | −0.0004 (−0.0008 to 0.0001) | −0.0004 (−0.0008 to 0.0001) |
| Interaction term (genetic × environmental risk scores) | 0.0005 (0.0001 to 0.0008)b | |
Abbreviation: AFCAP, age at first cohabitation with adoptive parents.
P < .001.
P < .05.
Figure.
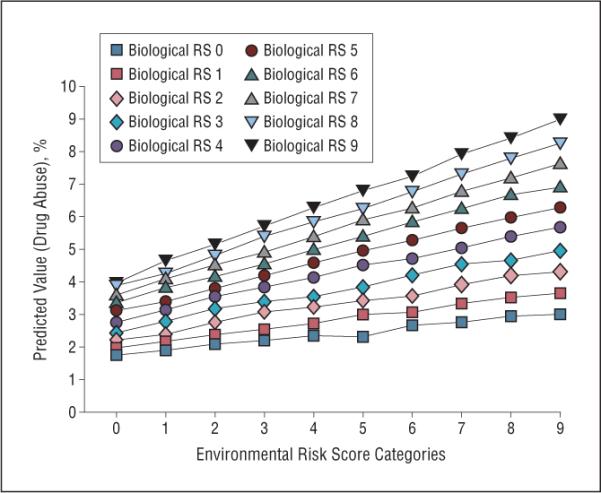
Predicted values for the risk for drug abuse in adopted children from the multivariate analysis of the genetic and environmental risk scores (RS) and the interaction between them on the scale of raw probabilities using an identity link in a generalized linear model. The 10 categories of increasing environmental risk (from 0 to 9) are depicted on the x-axis and the predicted risk for drug abuse on the y-axis. The lines depict the predicted risk for drug abuse as a function of the level of increasing genetic risk (from 0 to 9).
COMMENT
From these analyses, 5 results are noteworthy. First, we replicated in a large national full-adoption design results from 4 large-sample general population twin studies performed in Australia and the United States5,7–9 showing a strong contribution of genetic factors to the etiology of DA. While our study used registry data, diagnoses of DA in these twin studies were all based on personal interviews. Our results are also consistent with findings from a small-sample US adoption study that examined 197 adopted children of parents selected for alcohol abuse, DA, or antisocial behavior from hospital and prison records and matched control subjects.18,19 Because we had full population information, we could use in the same cohort both standard adoption designs. Beginning with biological parents with DA, their adopted away children had more than a 2-fold increased risk for DA. Beginning with adopted children with DA, their biological full and half siblings had a 1.8- and 1.4-fold increased risk for DA, respectively.
Twin and adoption studies are both quasi-experimental methods, each with potentially significant methodological limitations. Therefore, our confidence in the etiologic role of genes in DA, which has hitherto been based largely on results from twin studies, should be strengthened by our findings in a large, representative adoption cohort where diagnoses were based on objective records and not susceptible to self-report bias.
Second, when pregnant, biological mothers could have abused substances that might have increased their off-spring's risk for DA via intra-uterine effects.20 We could rule out this possibility because of the greater risk for DA in the adopted away children of biological fathers vs mothers with DA.
Third, DA in adopted children was predicted not only by DA in their biological relatives, but also by a history of alcohol and psychiatric or criminal problems. These results replicate prior findings that genetic risks for DA are partly shared with other externalizing traits and disorders.18,19,21–23
Fourth, a range of environmental features of the adoptive family predicted risk for DA in adopted children. Unlike prior studies in intact families, the causal chain between these risk factors and DA is not confounded by genetic relationships between family members. These diverse risk factors include disruption of the marital and parent-child bonds through death or divorce, alcohol problems in the adoptive parents or siblings, and criminal behavior and medical hospitalization in the adoptive parents. We would speculate that the causal processes here might include increased marital tension, poorer parent-child relationships, and reduced parental monitoring. Interestingly, risk for DA in adopted children was more strongly predicted by DA in the adoptive siblings than adoptive parents. Our results suggest that social influences (eg, peer deviance and drug availability) shared with adoptive siblings are more potent environmental risks for DA than direct psychological transmission of DA from parent to child.24 Evidence from this study for robust shared environmental effects on DA is at variance with results from some6,7,9 but not all5,8 adult twin studies examining lifetime drug abuse/dependence. Prior twin studies of drug use typically found strong shared environmental effects in adolescence25,26 that largely disappeared in adulthood. However, our findings confirm prior results from a US study that found significant resemblance in 246 adoptive adolescent same-sex sibling pairs for substance use disorders.27
Fifth, we found evidence for gene-environment interaction in the etiology of DA. Adopted children at high genetic risk were more sensitive to the pathogenic effects of adverse family environments than those at low genetic risk. In other words, genetic effects on DA were less potent in low-risk than in high-risk environments. These results are consistent with prior twin studies suggesting that genetic influences on psychoactive substance use in adolescence are enhanced in high-risk environments characterized by low parental monitoring,28 easy substance availability,29 and the presence of substance-using friends,29–32 as well as consistent with molecular genetic studies showing that risk variants may interact positively with familial environmental adversity in the prediction of DA.33
METHODOLOGICAL LIMITATIONS
These results should be interpreted in the context of 3 potentially important methodologic limitations. First, we identified subjects with DA from medical, legal, and pharmacy records. While this method has the important advantage of not requiring accurate respondent recall and reporting, it could produce both false negative (individuals with DA who never had medical or legal attention) and false positive diagnoses (individuals arrested or treated for a drug problem without having DA or being treated for chronic pain with very high doses of opiates). Our construct of DA may be broader than the definition of drug dependence operationalized in DSM-IV.34 We cannot precisely estimate our biases in the definition of DA as no large epidemiologic study has reported rates of DA in Sweden. However, such a survey done in neighboring Norway, which has similar rates of drug use and abuse,35,36 found lifetime prevalence rates of DSM-III-R37 DA and dependence of 3.4%,38 relatively close to the 2.7% we detected in all of Sweden.
Second, nonrandom placement of adopted children can bias adoption studies. Prior studies of Swedish adoptions noted modest selective placement (eg, plus 0.14 correlation in educational attainment between biological and adoptive parents).39,40 Our indices of genetic and environmental risks for DA were also intercorrelated (plus 0.11) but the magnitude was too small to substantially influence our findings.
Third, bias can also arise in adoption studies from extensive contact between the adopted children and biological parents prior to adoption. We had to approximate AFCAP from census records available every 5 years. We know that at least 70.9% of adopted children were living with their adoptive parents by age 5 years. However, during the years of our study, adopted children were typically removed shortly after birth from the biological mother and placed in a special nursery home.39,40 Often prior to formal adoption, the child would be placed for trial periods in foster homes. Thus, prior to placement in the adoptive home, adopted children in our sample were more likely to be in the special nursery or foster homes than with their biological parents.
We could assess this possible bias in 3 ways. First, if sustained contact with biological parents occurred and increased the risk for DA in the adopted child, then AFCAP should be significant and positively associated with DA. Instead, the correlation was negative. Second, delayed placement in the adoptive home could attenuate the impact of the adoptive environment. This would predict that AFCAP should negatively interact with the environmental risk score to predict DA. No such interaction was found (P=.88). Finally, we repeated our analyses in the subsample (n=12 783) where AFCAP was 5 years or less. The broad pattern of results was unchanged.
CONCLUSIONS
To our knowledge, this is the first large-scale, comprehensive adoption study of DA that has confirmed and extended prior studies showing that DA is etiologically complex with important genetic and shared-environmental influences. Both the genetic and the familial environmental influences on DA are themselves multifaceted. Risk for DA in adopted children is increased by a history in biological parents and siblings not only of DA but also of alcoholism, major psychiatric illness, and criminal convictions. Risk for DA in adopted children is increased by disruption in the adoptive parent–adopted child bond by death or divorce but also by a range of indices of a disturbed adoptive home environment and deviant peer influences such as parental alcoholism and sibling drug abuse, respectively. Finally, the genetic factors that influence liability to DA act not only by directly increasing the risk for illness but also by increasing the pathogenic effects of adverse environmental experiences.
Acknowledgments
Funding/Support: This study was funded by grant RO1 DA030005 from the National Institute of Drug Abuse, grants 2008-3110 and 2008-2638 from the Swedish Research Council, and a project grant from ALF, Lund, Sweden.
Role of the Sponsors: The sponsors were not involved in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review or approval of the manuscript.
Footnotes
Financial Disclosure: None reported.
REFERENCES
- 1.World Health Organization . Atlas on Substance Use (2010): Resources for the Prevention and Treatment of Substance Use Disorders. World Health Organization; Geneva, Switzerland: 2010. [Google Scholar]
- 2.Rounsaville BJ, Kosten TR, Weissman MM, Prusoff B, Pauls D, Anton SF, Merikangas K. Psychiatric disorders in relatives of probands with opiate addiction. Arch Gen Psychiatry. 1991;48(1):33–42. doi: 10.1001/archpsyc.1991.01810250035004. [DOI] [PubMed] [Google Scholar]
- 3.Merikangas KR, Stolar M, Stevens DE, Goulet J, Preisig MA, Fenton B, Zhang H, O'Malley SS, Rounsaville BJ. Familial transmission of substance use disorders. Arch Gen Psychiatry. 1998;55(11):973–979. doi: 10.1001/archpsyc.55.11.973. [DOI] [PubMed] [Google Scholar]
- 4.Bierut LJ, Dinwiddie SH, Begleiter H, Crowe RR, Hesselbrock V, Nurnberger JI, Jr, Porjesz B, Schuckit MA, Reich T. Familial transmission of substance dependence: alcohol, marijuana, cocaine, and habitual smoking: a report from the Collaborative Study on the Genetics of Alcoholism. Arch Gen Psychiatry. 1998;55(11):982–988. doi: 10.1001/archpsyc.55.11.982. [DOI] [PubMed] [Google Scholar]
- 5.Tsuang MT, Lyons MJ, Eisen SA, Goldberg J, True W, Lin N, Meyer JM, Toomey R, Faraone SV, Eaves L. Genetic influences on DSM-III-R drug abuse and dependence: a study of 3,372 twin pairs. Am J Med Genet. 1996;67(5):473–477. doi: 10.1002/(SICI)1096-8628(19960920)67:5<473::AID-AJMG6>3.0.CO;2-L. [DOI] [PubMed] [Google Scholar]
- 6.van den Bree MB, Johnson EO, Neale MC, Pickens RW. Genetic and environmental influences on drug use and abuse/dependence in male and female twins. Drug Alcohol Depend. 1998;52(3):231–241. doi: 10.1016/s0376-8716(98)00101-x. [DOI] [PubMed] [Google Scholar]
- 7.Kendler KS, Prescott CA. Cannabis use, abuse, and dependence in a population-based sample of female twins. Am J Psychiatry. 1998;155(8):1016–1022. doi: 10.1176/ajp.155.8.1016. [DOI] [PubMed] [Google Scholar]
- 8.Lynskey MT, Heath AC, Nelson EC, Bucholz KK, Madden PA, Slutske WS, Statham DJ, Martin NG. Genetic and environmental contributions to cannabis dependence in a national young adult twin sample. Psychol Med. 2002;32(2):195–207. doi: 10.1017/s0033291701005062. [DOI] [PubMed] [Google Scholar]
- 9.Kendler KS, Karkowski LM, Neale MC, Prescott CA. Illicit psychoactive substance use, heavy use, abuse, and dependence in a US population-based sample of male twins. Arch Gen Psychiatry. 2000;57(3):261–269. doi: 10.1001/archpsyc.57.3.261. [DOI] [PubMed] [Google Scholar]
- 10.Hawkins JD, Catalano RF, Miller JY. Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: implications for substance abuse prevention. Psychol Bull. 1992;112(1):64–105. doi: 10.1037/0033-2909.112.1.64. [DOI] [PubMed] [Google Scholar]
- 11.Newman K, Harrison L, Dashiff C, Davies S. Relationships between parenting styles and risk behaviors in adolescent health: an integrative literature review. Rev Lat Am Enfermagem. 2008;16(1):142–150. doi: 10.1590/s0104-11692008000100022. [DOI] [PubMed] [Google Scholar]
- 12.Wills TA, Dishion TJ. Temperament and adolescent substance use: a transactional analysis of emerging self-control. J Clin Child Adolesc Psychol. 2004;33(1):69–81. doi: 10.1207/S15374424JCCP3301_7. [DOI] [PubMed] [Google Scholar]
- 13.van den Bree MB, Pickworth WB. Risk factors predicting changes in marijuana involvement in teenagers. Arch Gen Psychiatry. 2005;62(3):311–319. doi: 10.1001/archpsyc.62.3.311. [DOI] [PubMed] [Google Scholar]
- 14.Steinberg L, Fletcher A, Darling N. Parental monitoring and peer influences on adolescent substance use. Pediatrics. 1994;93(6, pt 2):1060–1064. [PubMed] [Google Scholar]
- 15.Dube SR, Anda RF, Felitti VJ, Chapman DP, Williamson DF, Giles WH. Childhood abuse, household dysfunction, and the risk of attempted suicide throughout the life span: findings from the Adverse Childhood Experiences Study. JAMA. 2001;286(24):3089–3096. doi: 10.1001/jama.286.24.3089. [DOI] [PubMed] [Google Scholar]
- 16.Kendler KS, Gardner CO. Interpretation of interactions: guide for the perplexed. Br J Psychiatry. 2010;197(3):170–171. doi: 10.1192/bjp.bp.110.081331. [DOI] [PubMed] [Google Scholar]
- 17.SAS Institute Inc. SAS Online Doc Version 9.2. SAS Institute Inc; Cary, NC: 2007. [Google Scholar]
- 18.Cadoret RJ, Yates WR, Troughton E, Woodworth G, Stewart MA. Adoption study demonstrating two genetic pathways to drug abuse. Arch Gen Psychiatry. 1995;52(1):42–52. doi: 10.1001/archpsyc.1995.03950130042005. [DOI] [PubMed] [Google Scholar]
- 19.Cadoret RJ, Yates WR, Troughton E, Woodworth G, Stewart MA. An adoption study of drug abuse/dependency in females. Compr Psychiatry. 1996;37(2):88–94. doi: 10.1016/s0010-440x(96)90567-2. [DOI] [PubMed] [Google Scholar]
- 20.Frank DA, Rose-Jacobs R, Crooks D, Cabral HJ, Gerteis J, Hacker KA, Martin B, Weinstein ZB, Heeren T. Adolescent initiation of licit and illicit substance use: impact of intrauterine exposures and post-natal exposure to violence. Neurotoxicol Teratol. 2011;33(1):100–109. doi: 10.1016/j.ntt.2010.06.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kendler KS, Prescott CA, Myers J, Neale MC. The structure of genetic and environmental risk factors for common psychiatric and substance use disorders in men and women. Arch Gen Psychiatry. 2003;60(9):929–937. doi: 10.1001/archpsyc.60.9.929. [DOI] [PubMed] [Google Scholar]
- 22.Hicks BM, Krueger RF, Iacono WG, McGue M, Patrick CJ. Family transmission and heritability of externalizing disorders: a twin-family study. Arch Gen Psychiatry. 2004;61(9):922–928. doi: 10.1001/archpsyc.61.9.922. [DOI] [PubMed] [Google Scholar]
- 23.Kendler KS, Aggen S, Knudsen GP, Roysamb E, Neale M, Reichborn-Kjennerud T. The structure of genetic and environmental risk factors for syndromal and subsyndromal common DSM-IV axis I and all axis II disorders. Am J Psychiatry. 2011;168:29–39. doi: 10.1176/appi.ajp.2010.10030340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bandura A. Social Foundations of Thought and Action: A Social Cognitive Theory. Prentice-Hall; Englewood Cliffs, NJ: 1986. [Google Scholar]
- 25.Pagan JL, Rose RJ, Viken RJ, Pulkkinen L, Kaprio J, Dick DM. Genetic and environmental influences on stages of alcohol use across adolescence and into young adulthood. Behav Genet. 2006;36(4):483–497. doi: 10.1007/s10519-006-9062-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kendler KS, Schmitt E, Aggen SH, Prescott CA. Genetic and environmental influences on alcohol, caffeine, cannabis, and nicotine use from early adolescence to middle adulthood. Arch Gen Psychiatry. 2008;65(6):674–682. doi: 10.1001/archpsyc.65.6.674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Buchanan JP, McGue M, Keyes M, Iacono WG. Are there shared environmental influences on adolescent behavior? evidence from a study of adoptive siblings. Behav Genet. 2009;39(5):532–540. doi: 10.1007/s10519-009-9283-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Dick DM, Viken R, Purcell S, Kaprio J, Pulkkinen L, Rose RJ. Parental monitoring moderates the importance of genetic and environmental influences on adolescent smoking. J Abnorm Psychol. 2007;116(1):213–218. doi: 10.1037/0021-843X.116.1.213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kendler KS, Gardner C, Dick DM. Predicting alcohol consumption in adolescence from alcohol-specific and general externalizing genetic risk factors, key environmental exposures and their interaction. Psychol Med. 2011;41(7):1507–1516. doi: 10.1017/S003329171000190X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Dick DM, Pagan JL, Holliday C, Viken R, Pulkkinen L, Kaprio J, Rose RJ. Gender differences in friends' influences on adolescent drinking: a genetic epidemio-logical study. Alcohol Clin Exp Res. 2007;31(12):2012–2019. doi: 10.1111/j.1530-0277.2007.00523.x. [DOI] [PubMed] [Google Scholar]
- 31.Harden KP, Hill JE, Turkheimer E, Emery RE. Gene-environment correlation and interaction in peer effects on adolescent alcohol and tobacco use. Behav Genet. 2008;38(4):339–347. doi: 10.1007/s10519-008-9202-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Legrand LN, McGue M, Iacono WG. Searching for interactive effects in the etiology of early-onset substance use. Behav Genet. 1999;29(6):433–444. doi: 10.1023/a:1021627021553. [DOI] [PubMed] [Google Scholar]
- 33.Enoch MA, Hodgkinson CA, Yuan Q, Shen PH, Goldman D, Roy A. The influence of GABRA2, childhood trauma, and their interaction on alcohol, heroin, and cocaine dependence. Biol Psychiatry. 2010;67(1):20–27. doi: 10.1016/j.biopsych.2009.08.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition Revised. American Psychiatric Association; Washington, DC: 2000. [Google Scholar]
- 35.Kraus L, Augustin R, Frischer M, Kümmler P, Uhl A, Wiessing L. Estimating prevalence of problem drug use at national level in countries of the European Union and Norway. Addiction. 2003;98(4):471–485. doi: 10.1046/j.1360-0443.2003.00326.x. [DOI] [PubMed] [Google Scholar]
- 36.Hibell B, Guttormsson U, Ahlstrom S, Balakireva O, Bjarnason T, Kokkevi A, Kraus L. The 2007 ESPAD Report: Substance Use Among Students in 35 European Countries. The Swedish Council for Information on Alcohol and Other Drugs; Stockholm, Sweden: 2007. [Google Scholar]
- 37.American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders, Third Edition Revised. American Psychiatric Association; Washington, DC: 1987. [Google Scholar]
- 38.Kringlen E, Torgersen S, Cramer V. A Norwegian psychiatric epidemiological study. Am J Psychiatry. 2001;158(7):1091–1098. doi: 10.1176/appi.ajp.158.7.1091. [DOI] [PubMed] [Google Scholar]
- 39.Bohman M. Adopted Children and Their Families: A Follow-up Study of Adopted Children, Their Background, Environment and Adjustment. Proprius; Stockholm, Sweden: 1970. [Google Scholar]
- 40.Björklund A, Lindahl M, Plug E. The origins of intergenerational associations: lessons from Swedish adoption data. Q J Econ. 2006;121:999–1028. doi:10.1162/qjec.121.3.999. [Google Scholar]