

Abstract
Purpose: We compare patient populations attending chiropractors in the field to those in teaching clinics to allow educational institutions to determine if students are exposed to a similar case mix. The purpose of our study was to describe and compare descriptively the clinical case mix of a recently opened community-based teaching clinic to previously published practice data. Methods: A retrospective descriptive cross-sectional study was conducted using new patient records completed at a clinic. Data were extracted using a specifically designed abstraction form. Results: We manually abstracted 649 files. A total of 580 new patient files was included in the analysis, among which 57.7% included female patients with a mean age of 43 years (SD 18), and 42.1% presented with a chief complaint of more than one year in duration. The vast majority of patients complained of spinal pain (81.4%), most commonly low back pain. Almost 92% of the diagnoses were classified as simple (sprain/strain). The average number of visits per patient was 7.4 (SD 11.3); 54.7% received spinal manipulation on their first visit. The majority of patients were referred by the treating intern (64.8%) and about 24% of patients were local residents. Conclusions: Our study contributed to the few studies detailing patients attending chiropractic academic teaching clinics. It provided benchmark demographic and clinical data that may be used for operational planning. Our study suggested that the case mix of this teaching clinic provides interns with appropriate learning opportunities to achieve entry to practice competencies.
Key Indexing Terms: Ambulatory Care Facilities, Chiropractic, Demography
INTRODUCTION
“To study the phenomena of disease without books is to sail an uncharted sea, while to study books without patients is not to go to sea at all.” William Osler
An important outcome of a chiropractic clinical internship program is to ensure graduates are proficient diagnosticians and experts in therapeutic management of patients with neuromusculoskeletal conditions. In part, this is achieved by providing educational experiences designed to simulate “real life” clinical practice. Thus, the intern's clinical experience becomes the driving force for new and higher order learning. Schultz et al. found that in medical training, ambulatory clinics having an adequate number and variety of patients were highly sought after by final year medical students and residents.1 Bleakley and Bligh suggested that for patient encounters to be meaningful the undergraduate medical education curricula must offer early and real-time exposure to a variety of patients, rather than use paper-based cases and simulations.2
In an effort to determine the nature of an intern's patient encounter and their readiness to transition to private practice, Waalen et al studied the patient population at the Canadian Memorial Chiropractic College (CMCC) teaching clinic.3 They found that the teaching clinic patient population was younger, presented commonly with neck pain, and received fewer visits compared to those generally seen by chiropractors in private practice.3 Similar studies have been conducted in other jurisdictions, such as in Australia,4,5 United States,6–8 and New Zealand.9 For example, in the Australian study, it was noted that interns' learning opportunities were limited due to their inadequate exposure to patients with complaints of short duration (one day) and to pediatric patients compared to private clinics.4 The New Zealand study noted that a significant number of new patients presenting to the teaching clinic were asymptomatic.9 Nyiendo et al. studied six chiropractic college teaching clinics on the west coast of the United States.6 They found that clinic location was important in attracting patients of differing socioeconomic characteristics; however, there were no significant differences in the types of presenting health complaints. Morschauser et al. found that the inner city chiropractic teaching clinic had extremity complaints outnumbering back complaints, the patients were racially diverse, there were fewer “multiple complaints.” and a large percentage of patients were 65 years of age and older in comparison with 13 other clinical sites of four participating chiropractic colleges.7 Most of these studies raised questions about the appropriateness of the interns' experience in contrast to that which they'll experience once in private practice.
In preparing students for the challenges of private practice, understanding the characteristics of patients they will encounter also is important. Recent Ontario, Canada-based chiropractic practice studies suggested that the proportion of male-to-female patients was about equal and that 34% of the patients were adults 35–49.9 years old, with those older than 65 years comprising the smallest subgroup of patients followed by those less then 20 years of age (14%). Low back pain was the most common complaint (34% of males and 26% of females) followed by neck pain (17% of males and 23% of females), while thoracic spine and non-spinal areas accounted for just below 10% each. Chronic/recurrent conditions were twice as likely to be reported as acute complaints.10,11
Knowing the patient population served by chiropractors in the field and contrasting this with that in teaching clinics, allows the educational institutions to determine if students are being exposed to an appropriate case mix. Therefore, the purpose of our study was to describe the clinical case mix of a recently opened community-based teaching clinic and compare it descriptively to previously published provincial practice data.
METHODS
A retrospective cross-sectional study was conducted using clinic records of all new patients who attended the CMCC Bronte Harbour Chiropractic Clinic (Bronte clinic) between July 1, 2006 and July 31, 2008. Inclusion criteria included all new patients who had not been transferred to the Bronte clinic from another CMCC teaching clinic.
Study Variables
Data were extracted using a specifically designed abstraction form. The Chiropractic Patient Record Extraction Form (Form) is a three-page paper-pencil survey comprised of dichotomous and short answer questions pertaining to the specific study variables. Study variables were selected after reviewing the standard clinic intake forms, documentation requirements for patients presenting to CMCC clinics, as well as related published literature.
No personal identifying information (e.g., patient's name, address, or phone numbers) was collected. Each patient was uniquely identified using a randomly assigned study identification (ID) number. This assigned study ID number was allocated during the process of file selection and was referenced to the patient's original file number. The unique referenced ID number was recorded in a separate master file code book that was stored securely in a locked file cabinet, accessible only to the principal investigator.
The first three characters of the six character postal code were recorded to help identify the location of the patient's neighborhood and borough. Diagnoses were captured on the data extraction form in free text form. The diagnoses subsequently were collapsed into seven diagnostic categories (joint sprain [cartilage/disc], muscle strain, muscle and joint sprain/strain, ligament and capsule, vertebrae and bones, and nerve [cord, nerve root, peripheral]). These categories were derived from the ICD-9 code book and sorted into generic groups of conditions most commonly presenting to Ontario chiropractors as reported in the literature.3,10
Where necessary and appropriate, variable categories were collapsed to facilitate analysis. For example, inconsistency in the identification of various joint-related diagnoses resulted in collapse of the joint category to include ligament and capsule. The vertebrae and bones category was redefined as vertebral fracture. Occupation was captured in free text and classified subsequently according to previously reported categories.3 Missing data were recorded as missing and were not imputed.
Analysis
Data were analyzed descriptively, including frequencies, means, medians, and standard deviations. Nonparametric testing also was used to determine relationships between demographic variables and clinical characteristics. All missing data points were not included in the final analysis. Level of significance, where appropriate, was set at p < .05. Analyses were conducted using SPSS statistical package (Version 14; SPSS, Inc, Chicago, IL). Access to patient information was approved by the Associate Dean, Clinical Education. Ethics approval was granted by the Research Ethics Board of the Canadian Memorial Chiropractic College.
RESULTS
A total of 649 files was manually abstracted. Of these files 580 met the inclusion criteria. The excluded files had been categorized as regular patient files (n = 42), CMCC student files (19), and CMCC alumni files (8).
The majority of new patients presenting to the Bronte Clinic were female (57.7%). The mean age of the sample was 43 years (SD 18), with a range of 6 months to 92 years and median of 38 years. About three-quarters of the patients were between the ages of 21 and 60 years, and were distributed similarly between the sexes (Fig. 1). The percentage of single and married patients was distributed evenly.
Figure 1.
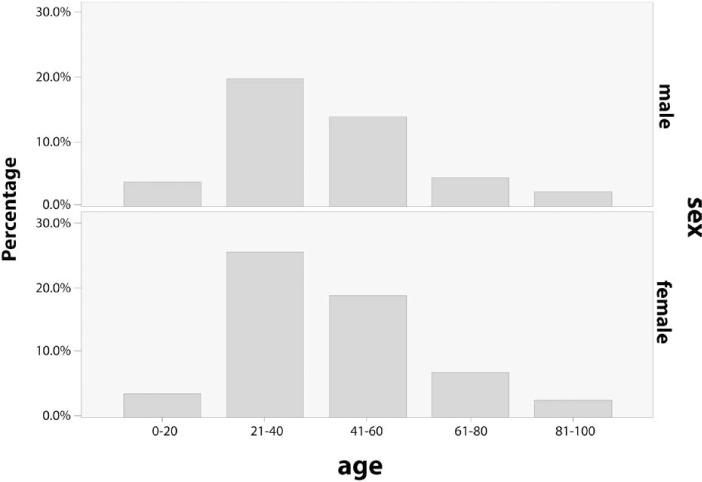
Age distribution by sex (22 files [3.8%] had missing data).
Figure 2 illustrates graphically the occupations of male and female subjects. The top three patient occupation categories were professionals (24.4%), students (16.5%), and skilled workers (12.9%), while retired patients comprised of 11.7% of the sample. Further assessment of the student category revealed that less than 1% was comprised of CMCC students.
Figure 2.
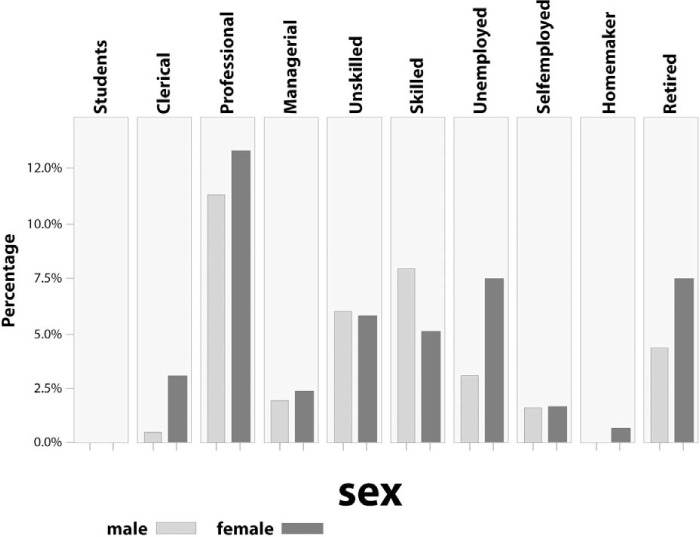
Occupational status by sex of patient.
Referral Patterns
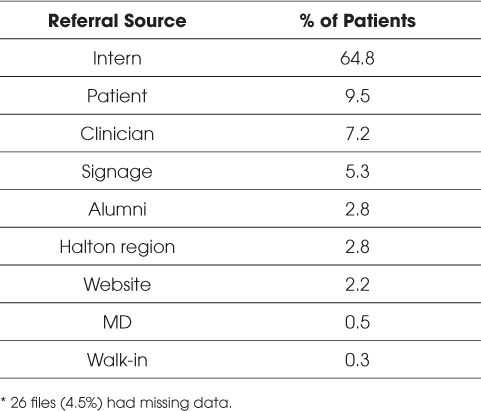
The majority of patients were referred by the treating intern (64.8%, Table 1). The combination of referrals from existing patients, clinician, and signage comprised 22% of the sample. Approximately one-quarter of the sample (22.9%) were family members of interns. Referred patients were 21–40 years old. Such patients were more than four times as likely to be referred by the intern compared to all other referral sources (36.6% vs. 8.2%).
Table 1.
Referral sources for chiropractic clinic patients. *
Based on the postal code, 24% of patients were local residents (e.g., Town of Oakville). More specifically, 12.3% of the patients lived within a 1 km radius of the clinic. Patients living in neighboring cities accounted for 22.1% (Mississauga), 13.6% (Hamilton), 11.3% (Burlington), and 6.1% (Toronto) of the sample.
About 25% of the patients had consulted another chiropractor for the same presenting complaint before attending the Bronte Clinic. On the other hand, 20.7% of patients had first consulted a physician before attending for care. Approximately a third (36.2%) reported not having consulted another health care practitioner at all. However, there was no statistically significant association between the duration of the chief complaint (e.g., greater than 6 months' duration) and having previously consulted a physician (X2 = .708, df = 1, p = .4).
Presenting Complaints
The regional distributions of presenting complaint for male and female patients are illustrated in Figure 3. The majority of the patients presented with a chief complaint of spinal pain (81.4%). The cervical category included head pain, whereas the lumbar category included pelvic complaints. Upper and lower extremity chief complaints were similar in frequency of presentation, 13.9% and 13.7%, respectively. The shoulder was the most commonly cited upper extremity complaint and the knee was the most commonly cited in the lower extremity. In 42.1% of patients, the duration of the presenting complaint was more than one year, compared to up to one month in 25.5%, 1–6 months in 19.2%, and 6–12 months in 13.2%.
Figure 3.

Distribution of presenting complaints by sex of patient.
Perceived neck and back disability was assessed during the first patient visit using standard outcome measures. However, the frequency of their application varied, with 25% of patients completing the Neck Disability Index (NDI) and 40% completing the Revised Oswestry Low Back Pain and Disability Index (RODQ). The average disability scores for patients completing the NDI and the RODQ were 22% (SD 18%) and 28% (SD 19), respectively, representing moderate perceived disability.12,13
Table 2 delineates the diagnoses given to patients on their first visit. In the teaching clinic environment, the process of assigning diagnoses for presenting complaints typically is a discussion at various stages of the intake between the intern and clinician. The intern is expected to present a list of differential diagnoses following the history, which then is refined following a physical examination and is finally signed off by the clinician before commencing a with a plan of management.
Table 2.
Diagnosis documented on the first patient visit.

Almost 92% of the diagnoses were re-classified as simple (i.e., sprain/strain) with less than 6% considered complicated (e.g., radiculopathy and fractures). At first visit, 18.5% of patients presented with plain film x-rays; while only 2.2% were referred for an x-ray subsequent to their initial consultation. Only a small percentage of patients reported having had an MRI (5.7%), of whom 61.1% were males.
Visit Characteristics
More than half (54.7%) of the patients received spinal manipulation on their first visit. The most common adjunctive therapies provided during the visit included soft tissue therapies (32.1%), exercise prescription (29.8%), and electro-modalities (12.1%). Only 3.8% of patients had not received any form of treatment on their first visit.
The average number of subsequent visits per patient was 7.4 (SD 11.3) with a median of 4. However, the actual number of treatments attributed to the chief complaint on initial visit could not be ascertained because patients' files also contained new complaints reported subsequent to the initial visit date, but that were not captured in this chart abstraction. A further analysis of frequency of patient visits revealed that 22.3% of patients did not return to the clinic following their first visit, with the majority (61.7%) being female. Almost three-quarters (73.3%) of these non-returning patients were referred by interns. An additional 8.8% only attended for two visits and 18.3% attended three times. The reasons for not returning to the clinic could not be identified.
All data collected were presented in aggregate form to assure confidentiality. Reliability of data entry was assessed descriptively by randomly selecting and completing 10 reports. The data in each of the 10 Forms were compared simultaneously and found to be the same. No further analysis was done.
DISCUSSION
Chiropractic academic teaching clinics have a very important role in the four-year chiropractic program. CMCC interns are provided opportunity to manage patients in seven different teaching clinics. The Bronte Clinic is the most recent addition to the list of CMCC external teaching clinics. Opened in 2006, it is located in a busy retail area in the heart of the Oakville community. It was established to represent a typical chiropractic clinic in Ontario. Interns are divided into two, three-day clinic schedules, allocated over one of six-month rotations and provided the opportunity to treat patients at the Bronte Clinic.
The findings in our study suggested that the general demographic and clinical characteristics of new patients presenting to the Bronte clinic are similar to those reported attending private practice chiropractors in Ontario, Canada. Waalen and Mior, using administrative billing data for the 2000–2001, found that one-third of the patients were between 35 and 49.9 years of age.10 Mior and Laporte, using Ontario-specific data from the National Population Health Survey (Statistics Canada, 1996–1997) and the Canadian Community Health Survey (Statistics Canada, 2000–2001), found that women were slightly more likely to visit a chiropractor (approximately 4.0% more), approximately 30% were seeking care for back pain, and the greatest distribution of patients (approximately 45%) were between 35 and 54 years old.11 Bronte interns also were most commonly assessing and treating working age adult patients with a slight predominance toward female gender.
Comparable to field practitioners, Bronte interns did not have a great deal of exposure to a pediatric population. The identification of this gap in age distribution would suggest a possible lack of awareness of the role of chiropractic in managing conditions in this age group, particularly in consideration of the prevalence of adolescent back pain and the reported favorable response to chiropractic care.14 For example, at the Anglo-European College of Chiropractic (AECC) in Bournemouth, England, increased community awareness has resulted in a increase in pediatric cases, thereby providing their interns with valuable clinical experiences unique to young children (personal communication with Dr Joyce Miller on May 6, 2007). A recent three-year retrospective study of pediatric case files at AECC found that chiropractic manipulation produced very few adverse effects and no serious complications were observed in patients younger than three years, with 85% of the parents reporting improvement.15
At the other end of the age spectrum, the retired status of the Bronte new patient sample was more than double than that found in an earlier study of CMCC clinics (11.7% vs. 4.2%).3 This may be due to the demographic of the Bronte area of Oakville. The clinic is situated among a number of seniors' residences within walking distance for those who are more active and able to access the clinic by foot. Despite this, the over 60 years age group still represented a relatively small percentage of the total sample. However, this is not unlike that seen among field chiropractors (about 12%);10 this highlights an opportunity for the clinic to be more proactive in educating the public and participating in health-related activities with seniors, in light of the potential benefits of chiropractic care. 11
Although spinal complaints were the most common reasons for consulting Ontario chiropractors as well as interns at the Bronte Clinic, there were some notable differences between these study populations. Almost half (48%) of the women presenting to the Bronte Clinic reported multiple site spinal pain compared to one-third of those attending Ontario chiropractors (30%).10 As we did in our study, Waalen and Mior found that men and women reported similar rates of back pain; however, neck pain complaints were twice as common in patients of field practitioners as those attending a teaching clinic.10 One possible explanation for the variation in presenting neck complaints is the increased scrutiny of chiropractic treatment of neck pain as a result of a highly publicized Ontario public inquiry into the death of a patient following a visit to a chiropractor.16 Perhaps patients may be less comfortable or are more apprehensive to report cervical spine complaints to novice interns versus field practitioners as there may be a perception that interns lack the experience to manipulate/adjust the cervical spine safely.
Thoracic spinal pain appeared to be the least commonly reported area of presenting complaints. This is not unusual as the lifetime prevalence of thoracic pain has been reported to be 15.6–19.5% compared to a low back pain lifetime prevalence of approximately 84% and neck pain lifetime prevalence of 66.7%.17–19 Unlike the findings of similar thoracic complaint rates for Ontario chiropractors and the earlier CMCC study (9% and 11.2%, respectively), the percentage of thoracic complaints was much smaller (5.3% of males and 2.1% of females).3,10 However, thoracic complaints may be underreported given the high rate of multiple site pain seen in the Bronte clinic sample. Overall, it appears that the Bronte interns are receiving sufficient exposure to all spinal level complaints. Men presenting to the Bronte teaching clinic were twice as likely (18% versus 8%) to report a chief complaint of extremity pain and women were three times more likely (21% versus 7%) compared to patients presenting to field practitioners.10 This relatively high presentation of extremity complaints (most commonly knee and shoulder) may contribute to an increased case mix, which in turn may provide more varied learning opportunities for interns. Martinez et al., in their study of a Mexican chiropractic college public clinic, found that extremity pain (most commonly knee) was the second most reported complaint (28%) behind lumbar pain (29.2%).20 They indicated that this coincided with the high percentage of traumatic etiology (46.6%). Unfortunately, the etiology variable was not captured in the data extraction form for our study.
Waalan and Mior found male and female patients to have a chronic/recurrent-to-acute ratio of approximately 2:1; however, the definition of acute and chronic was not provided.10 The Bronte sample of new patients also was heavily skewed toward the chronic stage (pain greater than six months in duration). If acute pain is defined as pain with duration of one month or less, than the Bronte sample comprised of one-quarter of the patients with recent onset pain. These findings are in keeping with data from other chiropractic college teaching clinics.4,7,8
Our study found that the majority of patients were referred by the interns. This scenario has positive and negative implications for the intern and the teaching clinic. From a business perspective, the skills of patient recruitment are learned during the interns' formative clinical education year. Our study found that 36.5% of the patients referred by the intern attended the clinic three times or less. This was found to be statistically significant compared to other referral sources (X2 = 8.889, df = 1, p = .003). It is unclear from the data if this is a function of meeting graduation requirements or patients improving over that particular time because they may present with uncomplicated clinic conditions despite the finding that 40.4% of this sample reported pain of more than six months in duration. Future research could help delineate the reasons for this lower average number of visits.
To have a substantial practice that is going to stabilize over time, there must be a significant amount number of files within the clinic that will generate new patient referrals from existing active patients and inactive patients coming back with new complaints.21 Given the large unstable patient base created by intern referrals, it becomes important to generate patients from the surrounding community to provide sufficient learning opportunities and appropriate case mix for interns. Thus, developing and maintaining a patient base for the clinic is important to ensure sustained clinical learning experiences for interns. Such a base is achieved most likely by emphasizing a clinician-based model of care, as clinicians add more stability than interns rotating through the clinic.
Mior and Waalen reported on personal and practice predictors associated with income of Ontario chiropractors.21 They found that the number of new patients seen by field practitioners was related inversely to the average cost per visit, suggesting patients consider cost before accessing care. Therefore, one of the benefits of having teaching clinics across communities is not only to provide educational opportunity for interns but also to provide care to patients who otherwise would not be able to afford it.7,8
As study analysis evolved, the narrow referral trend was becoming clear. In an effort to offset this trend, Bronte clinicians developed a joint partnership between regional social services to provide assessment and treatment of musculoskeletal conditions to qualifying clients at no cost to them. This partnership provides care to patients of lower socioeconomic status who normally could not afford chiropractic care, and increases the case mix and complexity seen by interns. These patients present a challenge for interns as these all were patients with longstanding musculoskeletal complaints. Further, such partnerships also decrease the reliance on intern referrals.
Although Nyiendo et al.6 noted that historically teaching clinics provided service for lower income populations, it does not appear to be the case at the Bronte clinic as the greatest number of patients were classified as professionals. This may in part be due to location, as Oakville is considered to be an affluent community. Similarly, interns are studying to be health professionals and may be socializing in circles with other professionals who are part of their cohort. Additional research is needed to ascertain if the interns actually are getting the experience that they should be getting in managing these patients.
Treatment procedures of Ontario chiropractors were described by Waalen and Mior.10 They found that high velocity, low amplitude spinal manipulation, or adjustment, was the primary form of treatment used by 85% of practitioners. Spinal adjustment also was the most common treatment modality used by chiropractic interns at the Bronte clinic, documented in over half of the treatment plans in case files (54.7%). Field practitioners additionally provide adjunctive treatment procedures, most commonly ultrasound or other electrotherapy modalities (29%).10 Bronte interns also used adjunctive treatments; however, soft tissue therapies and active exercise prescription were cited most commonly. This is consistent with evidence suggesting that the addition of exercise to manual therapy has better clinical outcomes for low back pain.22
Study Limitations
One of the main limitations of our study is its cross-sectional retrospective design. This design does not allow for causal inferences to be made.23 The data are simply a snapshot in time and may not account for inherent variations encountered over time or as the clinic's base increases. Our study also did not compare the findings at Bronte to those at the other CMCC teaching clinics nor field practitioner clinics. Rather, it relied on previously reported teaching clinic data that may not truly represent the current distribution of patients or their characteristics. However, in consideration of similar published reports, the findings reported herein may not be so different.
Another potential limitation is the chosen clinic site for data abstraction. The Bronte clinic is a newly established teaching clinic, hence the presenting case mix may change with time and the data presented in our study may be significantly different in a few years. In addition, the significant intern referral frequency also may bias the population under investigation and skew the findings. However, we felt our data could provide excellent benchmark information that could be used effectively in strategic planning for the clinic.
The Data Abstraction Form was developed specifically for our study. It was a complicated survey tool that attempted to capture many different variables and its psychometric properties were not measured formally. However, a random selection of 10 cases were compared to the original survey sheets and found that they were exactly the same. This provides some confidence that the data entered were usable.
CONCLUSION
Our study contributed to the few studies detailing patients attending chiropractic educational clinics, furthering the seminal work of Nyiendo et al.6 It also provided important data of patient demographic and clinical characteristics for the Bronte Clinic. In general, the Clinic's patient profile appears similar to that of practicing chiropractors. However, severity of condition and referral sources may suggest important differences between the patient populations. Such differences may impact upon the interns' training experience. Future research should expand the patient data gathering to other CMCC teaching clinics to compare effectively case mix as well as intern experiences. As suggested by Nyeindo et al., understanding the case mix of each clinic may allow the possibility of conducting cooperative studies using patients from various clinics and pooling the data.6
Our study provided important benchmark data for strategic planning to ensure intern exposure to an appropriate case mix during their clinical year practice. Our study suggested that the Bronte clinic's case mix provided interns with appropriate learning opportunities to achieve competencies necessary for practice. Our results could be used to target different patient populations to ensure sustainability and enhancement of the clinic's patient teaching base.
Footnotes
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare.
REFERENCES
- 1.Schultz KW, Kirby J, Delva D. 2004. Medical Students' and Residents' preferred site characteristics and preceptor behaviours for learning in the ambulatory setting: a cross-sectional survey. BMC Med Educ. 2004;4:12. doi: 10.1186/1472-6920-4-12. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bleakley A, Bligh J. Students learning from patients: let's get real in medical education. Adv Health Sci Educ Theory Pract. 2008;13:89–107. doi: 10.1007/s10459-006-9028-0. [DOI] [PubMed] [Google Scholar]
- 3.Waalen DP, White TP, Waalen JK. Demographic and clinical characteristics of chiropractic patients: a five year study of patients treated at the Canadian Memorial Chiropractic College. J Can Chiropr Assoc. 1994;38(2):75–82. [Google Scholar]
- 4.Walsh MJ, Jamison JR. A comparison of patients and patient complaints at chiropractic teaching clinics and private clinics. Chiropr J Aust. 1992;22:87–91. [Google Scholar]
- 5.Walsh MJ. A study of patients and patient complaints at chiropractic teaching clinics. Chiropr J Aust. 1992;22:61–64. [Google Scholar]
- 6.Nyiendo J, Phillips RB, Meeker WC, Konsler G, Jansen R, Menon M. A comparison of patients and patient complaints at six chiropractic teaching clinics. J Manipulative Physiol Ther. 1989;12(2):79–85. [PubMed] [Google Scholar]
- 7.Morschhauser E, Long CR, Hawk C. Do chiropractic colleges' off-campus clinical sites offer diverse opportunities for learning? A preliminary study. J Manipulative Physiol Ther. 2003;26:70–6. doi: 10.1067/mmt.2003.21. et al. [DOI] [PubMed] [Google Scholar]
- 8.Stevens GL. Demographic and referral analysis of a free chiropractic clinic servicing ethnic minorities in the Buffalo, NY area. J Manipulative Physiol Ther. 2007;30:573–77. doi: 10.1016/j.jmpt.2007.07.016. [DOI] [PubMed] [Google Scholar]
- 9.Hold KR, Beck RW. Chiropractic patients presenting to the New Zealand College of Chiropractic teaching clinic: a short description of patients and patient complaints. Chiropr J Aust. 2005;35:122–4. [Google Scholar]
- 10.Waalen JK, Mior SA. Practice patterns of 692 Ontario chiropractors (2000–2001) J Can Chiropr Assoc. 2005;49(1):21–31. [PMC free article] [PubMed] [Google Scholar]
- 11.Mior SA, Laporte A. Economic and resource status of the chiropractic profession in Ontario, Canada: A challenge or an opportunity. J Manipulative Physiol Ther. 2008;31:104–114. doi: 10.1016/j.jmpt.2007.12.007. [DOI] [PubMed] [Google Scholar]
- 12.Baker D, Pynsent PB, Fairbank JCT. The Oswestry disability index revisited: its reliability, repeatability, and validity, and a comparison with St. Thomas' disability index. In: Roland M, Jenner JR, editors. Back Pain. New Approaches to Rehabilitation and Education. Manchester: Manchester University Press; 1989. pp. 174–186. [Google Scholar]
- 13.Vernon H, Mior S. The Neck Disability Index: a study of reliability and validity. J Manipulative Physiol Ther. 1991;14(7):409–415. [PubMed] [Google Scholar]
- 14.Hayden JA, Mior SA, Verhoef MJ. Evaluation of chiropractic management of pediatric patients with low back pain: A prospective cohort study. J Manipulative Physiol Ther. 2003;26(1):1–8. doi: 10.1067/mmt.2003.11. [DOI] [PubMed] [Google Scholar]
- 15.Miller JE, Benfield K. Adverse effects of spinal manipulative therapy in children younger than 3 years: a retrospective study in a chiropractic teaching clinic. J Manipulative Physiol Ther. 2008;31(6):419–423. doi: 10.1016/j.jmpt.2008.06.002. [DOI] [PubMed] [Google Scholar]
- 16.Office of the Chief Coroner of Ontario, Province of Ontario, 2004. http://www.mcscs.jus.gov.on.ca/English/pub_safety/office_coroner/verdicts_and_recs/2004%20Inquests/LEWIS%20verdict.pdf. Accessed May 16, 2010.
- 17.Briggs AM, Smith AL, Straker LM, Bragge P. Thoracic spine pain in the general population: prevalence, incidence and associated factors in children, adolescents and adults. A systematic review. BMC Musculoskelet Disord. 2009;10:77. doi: 10.1186/1471-2474-10-77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Cassidy JD, Carroll LJ, Côté P. The Saskatchewan health and back pain survey. The prevalence of low back pain and related disability in Saskatchewan adults. Spine. 1998;23(17):1860–6. doi: 10.1097/00007632-199809010-00012. [DOI] [PubMed] [Google Scholar]
- 19.Côté P, Cassidy JD, Carroll L. The Saskatchewan Health and Back Pain Survey. The prevalence of neck pain and related disability in Saskatchewan adults. Spine. 1998;23(15):1689–1698. doi: 10.1097/00007632-199808010-00015. [DOI] [PubMed] [Google Scholar]
- 20.Martinez DA, Rupert RL, Ndetan HT. A demographic and epidemiological study of a Mexican chiropractic college public clinic. Chiropr Osteopath. 2009;17:4. doi: 10.1186/1746-1340-17-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Mior S, Waalan J. Personal and practice predictors associated with the income of Ontario Chiropractors. J Manipulative Physiol Ther. 2008;31:277–284. doi: 10.1016/j.jmpt.2008.03.001. [DOI] [PubMed] [Google Scholar]
- 22.Lawrence DJ, Meeker W, Branson R. Chiropractic management of low back pain and low back-related leg complaints: a literature synthesis. J Manipulative Physiol Ther. 2008;31(9):659–674. doi: 10.1016/j.jmpt.2008.10.007. et al. [DOI] [PubMed] [Google Scholar]
- 23.Mann CJ. Observational research methods. Research design II: cohort, cross sectional, and case-control studies. Emerg Med J. 2003;20:54–60. doi: 10.1136/emj.20.1.54. [DOI] [PMC free article] [PubMed] [Google Scholar]