

Abstract
Serous bursae consist of a synovial membrane enveloping a film of liquid. They are located at interfaces between moving structures where friction must be reduced. The bicipitoradial bursa lies between the distal tendon of the biceps brachii, which it surrounds, and the radial tuberosity. It is a relatively large bursa, with dimensions ranging from 2.4 to 3.9 cm. It sometimes presents septation. It does not communicate with the joint cavity, but it may communicate with the interosseous bursa of the elbow. Regardless of its cause, bicipitoradial bursitis presents as a mass in the cubital fossa and/or with neurological symptoms (sensorial and/or motorial) caused by compression of the radial nerve. On ultrasonography, the inflamed bursa is visualized as an anechoic formation surrounding the distal biceps tendon. In addition to its role in diagnosing the bursitis, sonography can provide information about radial nerve injury (in the presence of macroscopic damage), and it can also be used for guidance during intrabursal injections.
Keywords: Bicipitoradial bursa, Distal tendon of the biceps brachii, Ultrasonography
Sommario
Le borse sierose sono costituite da membrana sinoviale che circonda un film liquido; sono localizzate dove è necessario ridurre la frizione tra strutture in movimento.
La borsa bicipito-radiale è posta tra il tendine distale del bicipite, che avvolge, ed il tubercolo radiale. È una borsa discretamente voluminosa, che può raggiungere dimensioni tra 2,4 e 3,9 cm.
Può essere settata, non comunica con la cavità articolare, può comunicare con la borsa interossea.
Indipendentemente dall’eziologia, la borsite si presenta come massa a livello della fossa cubitale, o con sintomi sensitivi e/o motori legati alla compressione del nervo radiale, o in entrambi i modi.
Ecograficamente si presenta come formazione anecogena, che circonda il tendine distale del bicipite. Oltre alla diagnosi di borsite, l’ecografia consente di valutare la sofferenza del nervo radiale, quando sono presenti danni macroscopici, e infiltrazioni guidate della borsa.
Introduction
Serous bursae consist of a synovial membrane enveloping a film of liquid. They are located at interfaces between moving structures, where friction must be reduced [1–3]. They are therefore found between tendons and bones or between two tendons (subtendinous bursae); between muscles and tendons, bones, or ligaments (submuscular bursae); between aponeuroses and bones (subfascial bursae); and between cutaneous/subcutaneous tissues and bone, muscles, or tendons (subcutaneous bursae). They can also develop in areas where friction occurs (adventitial bursae) [1]. The so-called constant bursae develop in utero and are therefore genetically determined, although mechanical factors are important in their evolution. Some of these bursae are continuations of the articular cavity; others form the synovial sheaths surrounding tendons.
Inflammation of a bursa is often caused by bleeding secondary to acute traumatic injury or repetitive microtrauma [1,3]. In acute post-traumatic forms, the blood irritates the thin synovial membrane, provoking an abundant serohematic effusion. Forms caused by repeated microtraumatic injury are typically associated with a synovial effusion and uniform thickening of the walls of the bursal sac. Other causes of bursitis include infection (tuberculosis, etc.); seropositive or seronegative arthropathy (rheumatoid arthritis and psoriatic arthritis, respectively); villonodular synovitis; osteochondromatosis; and amyloidosis. In these cases, typical findings are synovial effusion and marked thickening of the bursal walls (caused in part by proliferation of the synovial membrane and in part by stromal hypertrophy and hyperemia), which often appear irregular owing to the presence of nodules or foci of villonodular proliferation.
The bicipitoradial bursa
The bicipitoradial bursa lies between the distal tendon of the biceps brachii (anterior), which it surrounds (Fig. 1), and the radial tuberosity (posterior). The bursa surrounds the distal biceps tendon during supination of the forearm; during forearm pronation the bursa is compressed between the radial tuberosity, which becomes posterior, and the distal tendon of the biceps [1,3–5]. It is a fairly large bursa, with dimensions ranging from 2.4 to 3.9 cm. It sometimes presents septation; it does not communicate with the joint cavity, but it may communicate with the interosseous bursa of the elbow [4].
Figure 1.
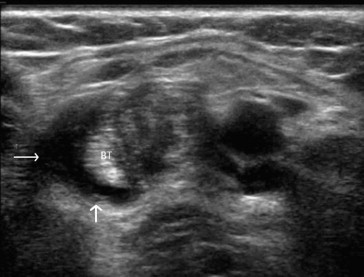
Bicipitoradial bursitis. Sonography reveals an anechoic formation (arrow) surrounding the distal tendon of the biceps (BT).
The most common causes of bicipitoradial bursal effusions are partial (Fig. 2) or complete (Fig. 3) tears of the distal biceps tendon [4,6,7], microtrauma, and rheumatoid arthritis [1,3,4]. The bursitis is manifested clinically by a mass in the cubital fossa, or by sensorial and/or motorial symptoms related to compression of the radial nerve (Fig. 4), or by a combination of the two. In most cases the swelling is clinically evident, and the neurological symptoms are associated with local pain [4].
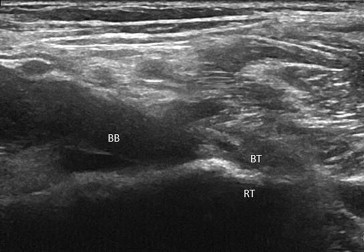
Figure 2.

Partial tear of the distal biceps tendon (BT). In addition to the partial tear involving the distal tendon at the level of its insertion on radial tuberosity (RT), the sonogram reveals an effusion within the bicipitoradial bursa (BB).
Figure 3.
Complete tear of the distal biceps tendon (BT). The sonographic image reveals the distal stump of the tendon (BT) at the level of its insertion on the radial tuberosity (RT) and an effusion within the bicipitoradial bursa (BB).
Figure 4.
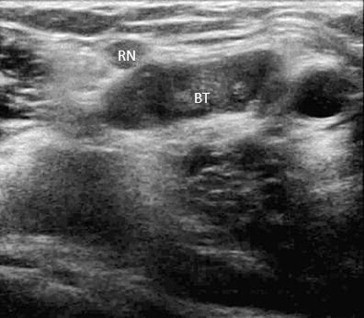
Bicipitoradial bursitis. Sonography reveals an anechoic formation surrounding the distal tendon of the biceps (BT), which is exerting pressure on the radial nerve (RN). The nerve itself is enlarged and hypoechoic.
The bursa itself cannot be sonographically explored unless it is distended by fluid. It can be located using the biceps as a landmark. At the level of the forearm, the biceps muscle lies superficial to the brachialis muscle, while the position of the tendon shifts from lateral to medial and from superficial to deep. Moving distally along the course of the biceps, the fluid-distended bicipitoradial bursa can be recognized surrounding the distal portion of the tendon. The examination is generally carried out during forced supination of the forearm, through the short axis relative to the muscle and tendon. Sonography is remarkably sensitive in identifying bursitis. It also allows assessment of macroscopic radial nerve damage and provides guidance for intrabursal injections of steroids and other therapeutic agents [8].
Conclusions
The bicipitoradial bursa allows the distal biceps tendon, which has no synovial sheath, to curl around the radial tuberosity without encountering friction. Inflammation of this bursa, which is usually the result of distal biceps tendon tears, microtrauma, or rheumatoid arthritis, results in swelling [1,3,4], which causes friction and pain and in some cases neurological symptoms related to radial nerve compression. Ultrasonography is useful for the diagnosis of this bursitis and for guiding intrabursal injections of therapeutic agents [8].
Conflict of interests
The authors have no conflicts of interest to declare relative to this article.
Appendix. Supplementary data
The following are the supplementary data related to this article:
References
- 1.Bianchi S., Martinoli C. Springer–Verlag; 2007. Ultrasound of the musculoskeletal system. 349–407. [Google Scholar]
- 2.Draghi F., Danesino G.M., de Gautard R., Bianchi S. Ultrasound of the elbow: examination technique and US appearance of the normal and pathologic joint. J Ultrasound. 2007;2:1–9. doi: 10.1016/j.jus.2007.04.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Draghi F. Ecografia; Athena: 2010. Il gomito. 77–85. [Google Scholar]
- 4.Skaf A.Y., Boutin R.D., Dantas R.W., Hooper A.W., Muhle C., Chou D.S. Bicipitoradial bursitis: MR imaging findings in eight patients and anatomic data from contrast material opacification of bursae followed by routine radiography and MR imaging in cadavers. Radiology. 1999 Jul;212(1):111–116. doi: 10.1148/radiology.212.1.r99jl49111. [DOI] [PubMed] [Google Scholar]
- 5.Bak B. Bicipitoradial bursitis. Ugeskr Laeger. 2008 Sep 29;170(40):3123–3124. [PubMed] [Google Scholar]
- 6.Sanal H.T., Chen L., Negrao P., Haghighi P., Trudell D.J., Resnick D.L. Distal attachment of the brachialis muscle: anatomic and MRI study in cadavers. AJR Am J Roentgenol. 2009 Feb;192(2):468–472. doi: 10.2214/AJR.08.1150. [DOI] [PubMed] [Google Scholar]
- 7.Chew M.L., Giuffrè B. Disorders of the distal biceps brachii tendon. Radio Graphics. 2005;25:1227–1237. doi: 10.1148/rg.255045160. [DOI] [PubMed] [Google Scholar]
- 8.Sofka C.M., Adler R.S. Sonography of cubital bursitis. AJR Am J Roentgenol. 2004 Jul;183(1):51–53. doi: 10.2214/ajr.183.1.1830051. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.