

Abstract
TAPSE measurement during echocardiography is a well known measure of right heart systo-diastolic function. Low TAPSE means reduced cranio-caudal excursion of tricuspidal annulus, sign of both reduced ejection fraction and reduced distensibility of right ventricle. It is a good prognostic index for cardiac mortality risk in CHF patients, adding significant prognostic information to NYHA stadiation.
Nephrologists do not always fully aware of right ventricular function in their patients affected by chronic renal failure (CRF), even if this datum is probably crucial in vascular access policy.
Our study was designed to study right ventricle function and TAPSE on 202 patients affected by moderate chronic renal failure, free from overt pulmonary hypertension. TAPSE, PAPs, right chambers diameters, classical Framingham factors, estimated glomerular filtration rate were recorded.
TAPSE was reduced (<23 mm) in 43% of patients enrolled, while dilated right chambers were present in 24%. PAPs exceeded 30 mmHg in 29% of patients. Echocardiographic signs of left ventricular hypertrophy were found in 36% of patients. The ejection fraction was normal in all patients. Statistical analysis showed a significant indirect correlation between TAPSE and PAPs and between TAPSE and tele-diastolic diameters and volumes of the right ventricle, while a direct correlation was observed between TAPSE and Framingham score.
TAPSE showed a bimodal distribution, with a subpopulation “low TAPSE – high PAPs”, next to a population characterized by normal values ??for both parameters.
A reduction in compliance and systolic function of the right heart chambers is quite early and frequent in course of CKD, a fact that the nephrologist should take in due consideration, managing blood volume or planning vascular access for hemodialysis.
Keywords: Echocardiography, Right ventricle, Chronic renal failure, TAPSE
Sommario
La misurazione dell'indice TAPSE nel corso di un esame ecocardiografico rappresenta un parametro ben codificato per la studio della funzione sisto – diastolica del cuore destro.
Bassi valori di TAPSE indicano una ridotta escursione cranio – caudale dell'anulus tricuspidale, a sua volta indice di ridotta frazione d’eiezione e distensibilità del ventricolo destro.
Al tempo stesso rappresenta un buon indice prognostico per il rischio di mortalità cardiovascolare in pazienti affetti da malattia renale cronica e conferisce ulteriore valore prognostico alla sola stadiazione NYHA.
I nefrologi non sono ancora del tutto consapevoli dell’importanza dello studio della funzione ventricolare destra nei pazienti affetti da malattia renale cronica (CKD) anche se il dato sembra essere cruciale soprattutto in vista di una buona politica riguardante il confezionamento dell’accesso vascolare per emodialisi.
Il nostro studio è stato progettato per valutare la funzione ventricolare destra e la TAPSE in 202 pazienti affetti da Malattia Renale Cronica di grado moderato senza segni clinici evidenti di ipertensione polmonare.
Sono stati presi in considerazione i seguenti parametri: TAPSE, PAPs, diametri delle sezioni cardiache di destra, fattori di rischio di Framingham e stima della frazione di filtrazione glomerulare.
I valori di TAPSE erano ridotti (<23 mm) nel 43% dei pazienti arruolati, mentre il 24% dei pazienti esaminati presentava dilatazione delle camere cardiache di destra con PAPs superiori ai 30 mmHg nel 29% dei pazienti. Segni ecocardiografici di ipertrofia ventricolare sinistra sono stati riscontrati nel 36% dei pazienti. La frazione di eiezione era normale in tutti i pazienti studiati.
L’analisi statistica dei dati ha evidenziato una significativa correlazione indiretta tra TAPSE e PAPs e tra TAPSE e diametri/volumi del ventricolo destro, mentre una correlazione diretta è stata trovata tra TAPSE e punteggio di Framingham.
I valori di TAPSE si sono distribuiti in maniera bimodale con una sottopopolazione “a bassi valori di TAPSE ed alti valori di PAPs” vicina ad un’altra caratterizzata dalla presenza di valori normali per entrambi i parametri.
Una riduzione della compliance e della funzione sistolica delle sezioni cardiache destre rappresenta un elemento precoce e frequente in corso di CKD, elemento che va tenuto in considerazione dai nefrologi allo scopo di controllare in maniera ottimale lo stato d’idratazione dei pazienti e pianificare una buona politica di allestimento di un accesso vascolare per emodialisi.
Introduction
Nephrologists usually need to have notion of a large number of parameters in the management of chronic renal diseases. Despite their efforts, they rarely have confidence with right heart functionality, even if this datum appears often crucial to hemodialysis vascular access policy and volumes management [1,2].
Tricuspid annulus plane systolic excursion (TAPSE) echocardiographic measurement is a well known, quick method of analysis of right heart systo-diastolic function. It does not require particular skill and has high reproducibility between operators [3].
TAPSE is not only an affordable index of right ventricle diastolic function, but it is easy to obtain in echocardiography, using a basic ultrasound system.
Low TAPSE means reduced cranio-caudal excursion of tricuspid annulus, sign both of reduced ejection fraction end reduced distensibility of right ventricle. It is a good prognostic index for cardiac mortality risk in CHF patients, adding significant prognostic information to NYHA stadiation.
Easily measured in all patients irrespective of heart rate and rhythm, it requires commonly available technology and it can therefore be currently extended to those patients in whom tachycardia or atrial fibrillation limits the analysis of mitral valve Doppler velocity curve.
Our study measured the prevalence of right ventricle dysfunction in moderate chronic renal failure patients, registering systematically TAPSE, right chambers diameters and volumes and estimated pulmonary pressures.
Materials and methods
202 patients (56 ± 12 years, 123 females, 79 males), affected by mild chronic renal disease (CKD-Epi estimated GFR between 60 and 15 ml/min) without overt heart disease, underwent conventional mono-, two-dimensional and Doppler echocardiogram, with a 3.5-MHz sectorial transducer and harmonic fusion detection. All echocardiographic examinations were made from two different operators, using the same methodology, using a GE Logiq 3 and a Pro-Logiq 7 (General Electrics©) ultrasound systems.
All images were recorded and stored on digital support. Measurements were obtained by averaging three cardiac cycles. Left ventricular end-diastolic volume, end-systolic volume, and ejection fraction (EF) were assessed using the modified biplane Simpson's equation.
Right Ventricle End Diastolic Diameter was recorded averaging measures obtained on M-mode from parasternal long-axis projection and on B-mode from an apical view.
TAPSE measurement was obtained from an apical approach, with an M-mode section of tricuspidal annulus, on the external side of atrial floor, measuring the distance (in mm) between the highest and the lowest point of annulus plan excursion.
Transmitral velocities were recorded in pulsed Doppler modality from the apical 4-chamber view by placing the sample volume at the tips of mitral leaflets.
All laboratory tests (blood urea nitrogen, creatinine, sodium, potassium, glucose, total cholesterol, HDL, triglycerides, blood count), weight, medical history and personal details were recorded directly from the electronic file in use in outpatient clinic (Gepadial, Traccia, Italy).
eGFR was calculated using CKD-Epi equation.
Statistical analysis was performed using Mystat 12.0 (Systat Software Inc.).
Results
TAPSE resulted mildly depressed (<18 mm) in 44.5% (90 subjects) of enrolled patients, while it was moderately reduced (<15 mm) only in 10.3% (21 patients) of them.
Right ventricle end-diastolic diameter > 22 mm was reported in 88 subjects (43%), while values >26 mm were reported in 107 patients (52.9%), and values >30 mm only in 6 of them (14.8%).
PAPs exceeded 30 mmHg in 28.7% of patients (58 patients), overcoming 40 mmHg in 5% of them (10 patients).
Left ventricular mass index overcame 140 g/mq in 36% of patients (72 subjects), with only a 16% of them exceeding 160 g/mq. Ejection fraction was normal in all enrolled patients (57 ± 5% of mean, median 56%).
Framingham traditional risk factors were distributed according to a Gaussian model, as reported in Fig. 3.
Figure 3.
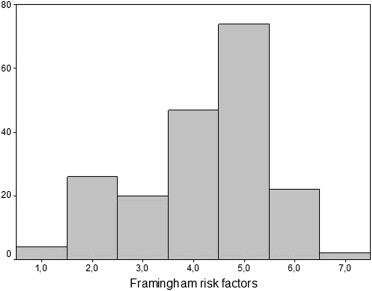
Distribution of Framingham classical risk factors.
Significant inverse correlations were observed between TAPSE and PAPs (β = −0.47, p < 0.005) (Fig. 1), right end-diastolic volumes (β = −0.198, p < 0.005) (Fig. 2), Framingham score (β = −0.17, p < 0.005) (Fig. 3), age (β = −0.19, p < 0.005). TAPSE was significantly lower in smokers with respect to non smokers. No significant differences were observed between diabetics and normoglycaemic patients.
Figure 1.
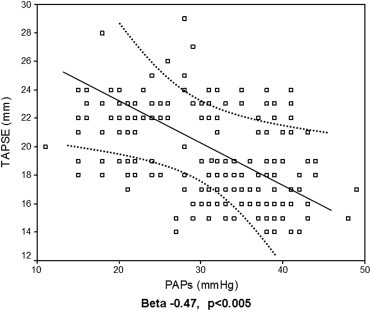
Simple correlation between TAPSE and PAPs.
Figure 2.
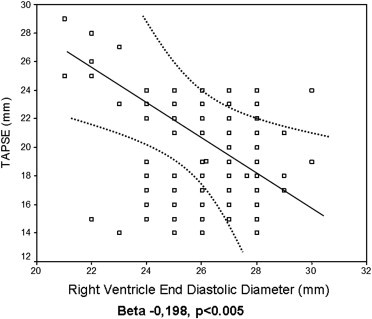
Simple correlation between TAPSE and Right Ventricle End Diastolic Diameter.
No correlations have been observed between eGFR, PTH, blood pressure levels and TAPSE or PAPs.
Distribution analysis of right heart parameters showed a bimodal distribution of many of them (Fig. 4 and Fig. 5), with a population at low TAPSE and high PAPs (41 patients), in front to a larger population characterized by normal values on both parameters.
Figure 4.
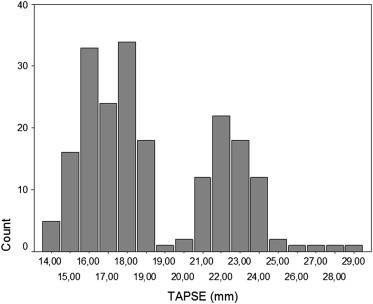
Distribution of TAPSE in whole population. Note bimodal distribution.
Figure 5.

Distribution of PAPs in whole population. Note bimodal distribution.
Conclusions
This study demonstrates an early right ventricular dysfunction, identified by reduced TAPSE and slightly increased PAPs, in a discrete quote of population affected by moderate chronic kidney disease (stage III according to National Kidney Foundation), in the absence of known heart disease.
It should be stressed that the inclusion criteria of this study have selected a population at low risk of pulmonary hypertension, because by definition free from respiratory disease, previous pulmonary embolism or thoracic surgery. It can be then assumed that “real” data about the presence of right ventricular dysfunction in the population of patients that crowd our clinics, is even more widespread.
This dysfunction was identified using a technique very reliable, economical, highly available, even in hospitals with low technological content, and above the direct reach of nephrologist sonographer.
Many nephrologists are often not accustomed to evaluate these variables, while on the other hand, many echocardiographers not systematically present measurements of TAPSE in their reports.
Nevertheless it's obtained with a simple measurement, fast and repeatable, which does not require the use of contrast media and is achievable even when the ultrasound acoustic windows are extremely reduced.
Even if this study cannot draw conclusions, it can formulate hypotheses, about the importance of early detection of right ventricular dysfunction in patients evaluated to plan a hemodialysis arterio-venous fistula, particularly in the more proximal forms of approach. In fact it is attractive the hypothesis that finding depressed TAPSE, in patients being studied for future vascular access, can somehow suggest caution in planning the use of brachial artery or of the first few centimeters of radial artery for native vascular accesses.
Such accesses, even if with the advantage of a better primary patency in “difficult” patients, involve the development of blood flow rates so high as to significantly increase the preload and the risk of pulmonary congestion. In patients with early congestion of the small circle, or initial, latent deficiency of the right ventricular pump, the packaging of such vascular access could lead to the development of pulmonary hypertension. In this case, patients could then manifest dyspnea, a usual symptom in clinical practice of the nephrologist, but this physician is accustomed to attribute it to other etiologies, particularly in patients with severe impairment of glomerular filtration rate. The diagnosis of pulmonary hypertension and of right ventricle failure then risks to be potentially hidden or delayed in ESRD patients.
The pathophysiology of the observed phenomenon is not clear, although this question goes beyond the scope and the objectives of an observational study.
We did not observe statistically significant relationships between the parameters of right heart function and glomerular filtration rate, PTH or blood pressure levels, while it was clear that cigarette smoking and age should be directly related to the presence of right dysfunction. The physiological aging and powerful oxidative stress elicited on the cardiovascular structures from smoking, seem to come right in the genesis of these phenomena.
In conclusion we suggest to all cardiologists and to nephrologists concerned to the execution of echocardiography to detect systematically TAPSE in all patients, especially if referred to a nephrological clinic, particularly when they go planning the packaging of a vascular access for hemodialysis.
It remains to be proven that the intervention of the nephrologist can interrupt the chain of events that leads to the genesis of the right ventricular dysfunction observed in nephropathic patients.
The results of this study seem suggest that much can be obtained from health education of patients, inducing them to abandon the habit of smoking, a risk factor now quite well defined, but unfortunately still spread.
Conflict of interest
Authors have no disclosure or conflict of interest to declare.
Footnotes
SIUMB Award for the Best Communication at the National SIUMB Congress 2011.
Appendix A. Supplementary data
References
- 1.Kjaergaard J., Iversen K.K., Akkan D., Møller J.E., Køber L.V., Torp-Pedersen C. Predictors of right ventricular function as measured by tricuspid annular plane systolic excursion in heart failure. Cardiovasc Ultrasound. 2009;7:51. doi: 10.1186/1476-7120-7-51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Meluzin J., Spinarová L., Hude P., Krejcí J., Dusek L., Vítovec J. Combined right ventricular systolic and diastolic dysfunction represents a strong determinant of poor prognosis in patients with symptomatic heart failure. Int J Cardiol. 2005;105(2):164–173. doi: 10.1016/j.ijcard.2004.12.031. [DOI] [PubMed] [Google Scholar]
- 3.Meluzin J., Spinarová L., Hude P., Krejcí J., Kincl V., Panovský R. Prognostic importance of various echocardiographic right ventricular functional parameters in patients with symptomatic heart failure. J Am Soc Echocardiogr. 2005;18(5):435–444. doi: 10.1016/j.echo.2005.02.004. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.