

Abstract
Although the social, economic, and political dimensions of the HIV/AIDS epidemic have been studied in considerable depth, the relationship between HIV/AIDS and its environmental causes and consequences remains largely unexplored. We reviewed the evidence of interactions between ecosystem health and the HIV/AIDS pandemic. We hypothesized a syndemic between environmental degradation and HIV/AIDS; they exhibit bidirectional, self-reinforcing interactions. We have presented a syndemic framework detailing multiple synergistic relationships. This framework hinges on the vulnerability of populations as the linchpin between the pandemic and environmental health. A coherent research and practice agenda for addressing the syndemic that focuses on the 2 issues as not only concurrent but also intertwined phenomena is urgently needed.
The devastating impact of HIV/AIDS is unprecedented, with more than 33 million individuals now infected globally.1 In addition to 2 million deaths occurring annually as a result of HIV/AIDS, its regional economic, health, and social impacts have been well documented. The pandemic continues to affect the livelihoods of individuals, families, and communities, especially in sub-Saharan Africa.
In regions of the world most affected by HIV/AIDS, the pandemic is occurring in the context of massive environmental and societal changes. Global climate change, human industry, and shifting patterns of migration because of poverty, inequality, and conflict are dramatically altering the social and natural environment of those regions most affected and may play a key role in driving and sustaining the pandemic. However, the effects of HIV/AIDS on the environment and, conversely, those of climate and environmental changes on the spread of the virus have not been adequately explored.
Despite a number of studies and reviews that have addressed various facets of the relationships between the HIV/AIDS epidemic and the environment—including natural resource use,2–8 workforce considerations,7,9–11 effects of climate change,12–16 food and livelihoods connections,17–21 and gender issues related to both phenomena,5,20,22–24—to date, no authoritative review synthesizes the complex, bidirectional, self-reinforcing interactions between environment and HIV/AIDS. No comprehensive framework for conceptualizing the connections between the phenomena exists.
We hypothesized a syndemic between the HIV/AIDS epidemic and ecosystem degradation. A syndemic can be defined as “two or more afflictions interacting synergistically, contributing to excess burden of disease in a population.”25 In epidemiological and public health contexts, a syndemic orientation has been applied to co-occurring health problems and pathogen–pathogen interactions but has also been used to more generally express the interactions between diseases and social conditions.26 Singer characterizes this broader definition as follows:
A syndemic, in short, involves a set of enmeshed and mutually enhancing health problems that, working together in a context of deleterious social and physical conditions that increase vulnerability, significantly affect the overall disease status of a population.26(p15)
It is this more general conception of syndemic that we use to frame the discussion of the interactions between HIV/AIDS and the environment. We proposed that the “determinant importance of social conditions in the health of individuals and populations”27(p428) that Singer postulates in describing syndemics can and should be extended to broader environmental conditions.
The concurrent, intertwined, and mutually reinforcing relationships between impoverished ecosystem services and HIV/AIDS infections and their sequelae reflect the synergies inherent to syndemics. It is not just the colocation of environmental pressures and HIV/AIDS in regions most affected but rather the complex ways these factors interact that contributes to excess burden of disease, poverty, and depleted resources in vulnerable areas. We have presented evidence of the syndemic from the literature and from qualitative information provided by key informants. Furthermore, we have presented a conceptual framework to depict the complex, reinforcing relationships that form the syndemic.
Applying a syndemic lens to the intertwined relationships between HIV/AIDS and ecosystems degradation allows researchers, practitioners, and policymakers to address the 2 phenomena in an integrated fashion. Adopting a syndemic framework paves the way for developing a body of evidence regarding these relationships as well as for piloting integrated interventions that address the phenomena as intertwined and for identifying best practices for scaling up.
REVIEWING THE EVIDENCE
We reviewed the scientific literature on links between HIV/AIDS and the environment to determine whether sufficient data exist to conduct a formalized systematic review of the evidence. If adequate high-quality qualitative and quantitative data from the literature were not available, our objective was to develop a conceptual framework to serve as a theoretical basis for focusing additional research and to help public health practitioners interpret the relationships between the phenomena.
In the literature review, we focused on reports from East and Southern Africa, regions that are heavily afflicted by the HIV/AIDS epidemic and that have experienced major changes in the environment. We searched for articles in PubMed and ISI Web of Science, combining the medical subject headings or keywords HIV or AIDS and Africa or developing countries with any 1 of the following: agriculture, biodiversity, climate, conservation of natural resources, cost of illness, edible plants, emigration and immigration, environment, environmental and ecological phenomena, environmental health, environmental medicine, family characteristics, farming, fish, food, food supply, food habits, forest, health expenditures, nutrition, rural populations, sanitation, socioeconomic factors, vulnerable populations, water. In addition, we searched the Web sites of a number of government and nongovernmental agencies and reviewed the references of published articles for additional source material. We also contacted authors and program managers for additional documents, including program reports and workshop proceedings.
The database queries and other search methods identified approximately 6500 references for possible inclusion in the review. After reviewing titles, we excluded most of these references on the basis of title alone, as they did not address some aspect of both the HIV/AIDS epidemic and environmental issues. We reviewed the abstracts of 914 articles, after which we excluded 445 references. We reviewed the full text of 469 references, after which we excluded 227. We ultimately conducted a qualitative review of 242 documents.
Our review did not identify sufficient randomized trials and well-controlled studies to enable a traditional systematic review under our a priori conditions. We determined that a traditional systematic review—including thorough evaluation of the quantity and quality of rigorously controlled data on the multiple connections between HIV/AIDS and the environment—would not sufficiently address the complexity or the significance of the interrelationships we discovered in the literature. Because of significant gaps in research, the lack of a coherent conceptual or theoretical framework, and the multiple, overlapping, bidirectional relationships, we did not conduct a traditional systematic review.
Given the literature gaps and weaknesses, we determined that the best alternative was to synthesize the evidence in a subjective fashion with the goal of framing a conceptual model that could be tested under conditions of well-conducted trials. This might encourage further research and could provide a starting point for further discussion and hypothesis generation regarding the links between the epidemic and degradation of ecosystem services.
Our synthesis and conceptual framework rely on the scholarly articles, white and gray literature, and other reports we reviewed as well as on substantial subjective experiential and theoretical knowledge. In 2010, we conducted approximately 30 informal individual and small group discussions with academics, program managers, and implementers in Kenya and the United States and conducted site visits with multiple community groups and nongovernmental organizations working with HIV/AIDS or the environment in Kenya.
Because empirical data on the interactions between HIV/AIDS and the environment are scant, our review was exclusively qualitative, and emerging findings in the literature guided our analysis. We performed thematic content analysis, coding salient themes in the literature and in extensive notes from field visits. We then refined and narrowed these codes through discussion and comparison to ensure that they were not redundant and that they represented the source documents fairly. A number of themes emerged from this literature review and from qualitative discussions with partners. We have presented evidence of several of the primary connections between the HIV/AIDS epidemic and environmental health.
RELATIONSHIPS BETWEEN HIV/AIDS AND THE ENVIRONMENT
The conceptual framework addresses the complexity of the multiple relationships between HIV/AIDS and the environment. Because of the range of evidence we discovered regarding these topics and because of their centrality to the syndemic framework, 3 issues merit further introduction: vulnerabilities and coping, global climate change, and workforce effects.
Vulnerabilities and Coping
Because HIV/AIDS disproportionately affects individuals during their most productive wage-earning and reproductive period (between 18 and 45 years), its resultant illness and mortality often result in a labor shortage at the household and community levels.28–31 Livelihoods dependent on physical labor, such as agriculture, pastoralism, and fisheries, may therefore be jeopardized when a family member becomes HIV infected.
In the agricultural sector, transitions to lower labor-intensity farming techniques, to increases in the leasing or sharecropping of land, and even to increased fallowing of productive land have been observed as a result of increasing HIV/AIDS prevalence in sub-Saharan Africa.32,33 Untreated HIV-infected tea pickers in Kenya earned 17% less than did their uninfected coworkers in the 2 years before their termination, and they used significantly more leave time.34 Increased adult mortality is negatively correlated with the amount of land cultivated at the community level and with total crop output.31,35,36 Farmers may also be more focused on short-term rather than long-term concerns, as the household’s demand for “quick cash” or food today outweighs future considerations—including sustainable land management—in the face of what may seem to be imminent mortality. Changes in inheritance patterns and land tenure for widows of HIV-positive men have also been observed. Land fragmentation and land “grabbing,” especially from orphans and widows, have been noted in Kenya, South Africa, and elsewhere.37,38 Women’s rights to land, although often officially codified in law, are not always protected in practice.37
Studies have documented that families affected by HIV/AIDS sell off household goods such as livestock as a buffer against lost wages or lower productive value from farm products and livestock as a result of diminished labor capacity.28,39 The subsequent erosion of household assets leaves families more vulnerable to further economic and health deterioration30,32 and has been described as resulting in a “downward spiral” of livelihood degradation.6,29 Even after starting antiretroviral therapy and physical recovery, many families are unable to recover socially and economically from the devastating effects of lost labor because of HIV morbidity.40 Individuals may resort to other erosive coping mechanisms, such as commercial sex work and the frequently described but largely unquantified phenomenon of bartering “fish for sex.”30,32 Erosive coping strategies further undermine the resilience of the household by diminishing its ability to absorb or recover from hazards.41
Livelihood insecurity may also result in food insecurity. Food insecurity is a linchpin between HIV/AIDS and the environment. Malnourished individuals are more susceptible to HIV infection,17,42 and to feed themselves or their families, they may be more likely to engage in risk behaviors that increase their exposure to the virus.43,44 Among HIV-infected individuals, antiretroviral therapy may be less effective in persons with inadequate nutrition.13,17 Low body mass index (defined as weight in kilograms divided by height in meters squared) is an independent predictor of death after antiretroviral therapy initiation, and food insecurity is a documented risk factor for noncompliance in antiretroviral therapy treatment.45 At a national level, average daily calorie consumption has been negatively associated with HIV/AIDS prevalence in an ecological study of 33 African countries.46
The relationship between food insecurity and HIV infection is circular; households affected by HIV/AIDS are subsequently less able—because of lost labor productivity—to ensure adequate supplies of food47 and are more likely to consume fewer nutrient-rich foods,48 increasing levels of malnutrition at the household level. Up to 5% of food insecurity in sub-Saharan Africa has been attributed to HIV/AIDS.49
Poverty is an important correlate and confounder of the relationships among HIV/AIDS, food insecurity, and natural resource use. Although the poor are not necessarily at higher risk for being exposed to or infected with HIV, they are differentially affected in terms of its sequelae and the ability to deal with its economic and social consequences.50 HIV-affected households are often likely to be impoverished and food insecure,28,39 and thus they are more likely to depend on natural resources as a safety net.30,32 Vulnerable households gather a number of natural products from the local environment, including wild foods (plants and animals), water, fuel wood, traditional medicinal products, timber, and raw materials for craft making. Natural resource collection is sometimes less labor intensive than is agriculture and requires little start-up capital.28 In at least 2 studies, in South Africa and in multiple sites in Malawi and Mozambique, households affected by adult mortality were observed to be up to 3.3 times more likely to collect firewood than were unaffected households.6,19
Anecdotal evidence suggests that increased dependence on natural resources of families affected by HIV/AIDS will lead to overharvesting of certain species and decreased biodiversity and ecosystem health. The quality, availability, predictability, and accessibility of natural resources have been observed to decline with increased use.11,19,51 As with selling off household assets, relying on natural resources can be seen as an erosive coping strategy if those resources are quickly depleted. By contrast, increased use of natural resources may not necessarily be detrimental to ecosystems if the resources are available in sufficient supply. Increased reliance of households affected by HIV/AIDS may then be seen as a livelihood diversification strategy that improves household resilience to threats and distributes risk.6 Few articles have addressed the environmental impacts of increased use of natural resources owing to HIV/AIDS, and quantification of the availability, use, and impact of natural resource use because of HIV/AIDS morbidity and mortality remains conspicuously absent.
Many groups, including women, orphans, and those affected by conflict and migration, appear to be particularly burdened by the syndemic between HIV/AIDS and ecosystem degradation. Because of their unique positions in both the epidemic and changing environments, these vulnerable populations represent a critical link between the 2 phenomena. The vulnerabilities of these populations lead both to increased HIV/AIDS risk and to more severe environmental consequences (e.g., erosive coping strategies, changes in livelihoods, and increased reliance on natural resources).
Gender inequality places girls and women at high risk for HIV infection by limiting the ability of women and girls to cope with economic, psychosocial, physical, or environmental difficulties. Girls and women worldwide have differential access to education, employment, credit, health services, and information52 and have a heavier burden of health problems and safety and security issues. They are more susceptible to the direct health effects that stem from living in poverty; inadequate access to water, sanitation, and health care differentially affects women.53 Female economic dependence on male partners is a major influence on the risk behaviors they undertake.50 The power differential in sexual relationships, coercion, and expectations that they be passive and ignorant in sexual matters may further endanger girls and women,54 as does their differential biological susceptibility to HIV infection. Meanwhile, women tend to carry the majority of the labor burden in household activities, childcare, and caring for the ill.30 In sub-Saharan Africa, women make up 70% of the agricultural workforce, and so livelihoods may be disproportionately affected by female illness and death.28 Discriminatory “traditional” practices such as widow inheritance, genital cutting, and early marriage also contribute to women’s vulnerability.37 Women’s risky sexual behavior appears to be more strongly associated with poverty than does men’s; impoverished women were more likely to have earlier ages for sexual debut and report more concurrent partnerships than were impoverished men.55 Food-insecure women have been documented to be more likely to engage in unprotected sex and to report less power in relationships than have men.43,44 Female heads of households are more likely than are male heads to be HIV infected,56 and households suffering female illness and mortality are more likely to suffer food insecurity.57
The intergenerational effects of the HIV/AIDS epidemic on the environment are striking and are not limited to mother to child transmission of the virus. More than 11.6 million children in sub-Saharan Africa have been orphaned by HIV/AIDS since the beginning of the pandemic.1 Orphans and vulnerable children are less likely to have been the beneficiaries of knowledge transfer. Gaps in traditional knowledge of farming techniques, natural resources management, and identification, collection, and use of natural products (including medicinal products) have been observed among orphans and vulnerable children.5,58,59 For instance, children orphaned because of HIV/AIDS in Tanzania were 10 times more likely to collect natural products such as wild orchids for consumption than were nonorphaned children.60 Additionally, like women, orphans and vulnerable children are more prone to land “grabbing” and are extremely vulnerable in terms of their livelihoods.37,61
Conflict and migration also contribute to interactions between HIV/AIDS and the environment. Rural to urban and seasonal migrants are at increased risk of HIV infection because of enlarged sexual networks, partner concurrency, increased substance abuse, higher population-level virus prevalence, social disruption, and higher rates of casual and commercial sex.33,51,62,63 At the same time, urban to rural reverse migration of the HIV infected puts additional demand on relatives—in terms of labor and care—and on the environment—in terms of natural resource utilization and increased pressure on ecosystems services.32,33 In South Africa, people who moved to rural areas in the previous year were 28% more likely to die than were more permanent rural residents in 2009 and were 79% more likely to die from AIDS.64
Two special cases of migration might further link the environment and HIV/AIDS risk. “Climate” refugees are forced out of their homes to migrate because of untenable land conditions, natural disasters, and climate change.65,66 “Conservation” refugees are forced to migrate because they live in conservation or protected areas.67 Both types of refugees might be at increased risk for HIV infection when their livelihoods and social networks are disrupted and they move to urban or periurban settings.
Conflict does not automatically translate to increased HIV/AIDS incidence or prevalence or to environmental degradation. Lack of privacy, decreased mobility, increased protection, and accessibility of health care and other services in refugee camps may actually shield some populations from HIV incidence in times of war.28–31 Nonetheless, a number of factors associated with armed conflict, such as lack of income, breakdown of social structures, sexual violence, drug use, and destruction of health and educational infrastructure, can lead to increased transmission.41,44,50,51 Conflict can lead to increased HIV/AIDS vulnerability both by increasing contact between uninfected and infected populations and by increasing the probability of HIV-transmitting events.37,38 HIV prevalence in armed forces across Africa has been documented to be as high as 27%.68
Likewise, the effects of conflict on ecosystem health are not unidirectional; conflict may preserve large tracts of land if people stay away because of fear of violence, but there is evidence of substantial environmental degradation because of armed conflict.69,70
The Impact of Global Climate Change
Natural resource availability and agricultural land productivity are intimately linked to climate factors, including temperature and precipitation. Global climate change appears to be contributing to environmental variability via higher risk of extreme weather events (e.g., droughts, floods, heat waves, and cold spells).14,71 This may lead to increased poverty, migration, and livelihood instability, which contribute to increased vulnerability and impaired coping ability, thus contributing to the syndemic. Degraded environments produce fewer crops, contributing to malnutrition and all its negative effects on health and the immune system.13,72 Global climate change may also result in changes in markets, food prices, or supply chain infrastructure.73
Environmental changes may foster conditions that are favorable for disease transmission, including many infections that affect people living with HIV/AIDS (e.g., malaria and diarrheal disease). Increased distances to reach water and decreased water quality threaten an increase in diarrheal pathogens.15 In addition, each 2°C to 3°C increase in ambient environmental temperature increases malaria transmission by 3% to 5%.74 Infection with malaria and other coinfections lead to significant increases in the amount of circulating virus in the blood of HIV-infected individuals, which may increase the rate of HIV disease progression and transmission.75
Decreased plant diversity and species loss may limit access to valuable plants, including some identified as having medicinal or anti-HIV properties.76 The Joint United Nations Programme on HIV/AIDS and the United Nations Environment Programme produced a joint working paper on HIV/AIDS and climate change in 2008 in which they present an “HIV/AIDS–climate change complex.”77 Food security, patterns of infectious disease, effects of pollution and heat stress on the immune system, and issues of governance, policy, and conflict are major points of interaction between climate change and the epidemic. Mojola et al. identify the eutrophication, pollution, and deforestation of the areas surrounding Lake Victoria as disruptive processes, which disturbed not only the local ecosystem but also the primary industry—fishing—and thereby the economy and the structure of sexual, domestic, and social partnerships.78 This ecological or “ecostructural” degradation is a potential root cause of increased HIV transmission.78
A Note on Workforce and Human Capacity
An additional facet of the relationship between the HIV/AIDS pandemic and ecological health is related to the impact of the epidemic on the workforce of conservation and environmental organizations. Conservation workers might be at increased risk of HIV infection because of their jobs, as they are often placed at remote locations far from their families; large populations of mobile men, isolated from their families and with access to cash incomes, have been documented to access commercial sex more frequently and to be at increased risk for HIV acquisition.11,61,77,79 Consequently, environmental institutions have observed the effects of HIV/AIDS morbidity and mortality, including increases in absenteeism, demand for employee assistance programs, medical or other support provided by the employer, and a decline in productivity and morale.
The loss of skilled professionals—many of whom are “investments” in terms of the education and on-the-job training they have received—has negative financial and programmatic effects on the functioning of the organization. In the environmental sector specifically, loss of workforce has led to decreased patrolling of protected areas and national parks,79 which may contribute to higher levels of poaching and unregulated natural resource harvesting in or near parks. These effects are consequential, but they have been addressed elsewhere and are not the focus of this review.11,51,58,63,66,80–83
TOWARD A SYNDEMIC FRAMEWORK
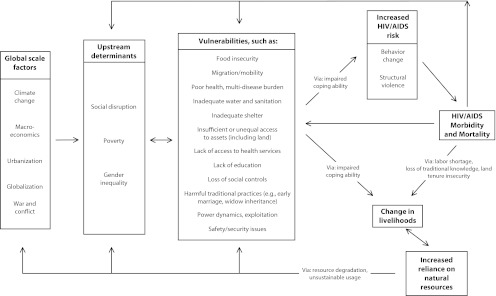
The conceptual framework is the consolidation of the literature review as well as a qualitative, subjective assessment of potential relationships between HIV/AIDS and the environment. It outlines the most important links between HIV/AIDS and the environment, reflecting the mutually reinforcing relationships and feedbacks between vulnerability, HIV/AIDS, and environmental degradation (Figure 1). Because of the scarcity of empirical data, not every aspect of this framework is supported by well-controlled studies. It is based on our assessment and weighing of the evidence as well as on our experiential and theoretical understandings of the relationships discussed.
FIGURE 1—

The syndemic framework for HIV/AIDS and the environment.
Note. The syndemic framework depicts the multiple, bidirectional, self-reinforcing relationships between the HIV/AIDS pandemic and ecosystem degradation. The syndemic framework is driven by global scale and upstream factors and is mediated by individual- and population-level vulnerabilities.
Several major global scale issues affect all aspects of the synergy between HIV/AIDS and environmental change. Global scale forces such as climate change, pollution, macroeconomic trade and aid policies, urbanization, conflict, and globalization set the stage for the challenging conditions in many of the nations of sub-Saharan Africa, yet they are forces over which Africans have little control at the household and community levels. Since the end of the colonial period, pervasive poverty, inequalities, conflict, and oppression have undermined community and household resilience. These interconnected factors have contributed to the emergence of structural violence and have placed communities in sub-Saharan Africa in a situation of both extensive ecosystem destruction and increased spread of HIV/AIDS.
Vulnerability has 2 aspects: stresses that people are subjected to (external) and their capacity to cope (internal) with those stresses.41,84,85 Global scale forces and upstream determinants increase both internal and external vulnerability at the household and community level. The increased pressures wrought on people by global and upstream factors make them more vulnerable to threats of all kinds and less likely to be able to cope with these threats. That is, people affected by poverty, food insecurity, landlessness, lack of access to resources and services, oppression, pervasive inequalities, and the atrocities of war are in every way less able to deal with problems of every sort.
In the framework depicted in Figure 1, vulnerability is the linchpin mediating between the upstream determinants and the downstream effects of HIV infection, changes in livelihoods, increased reliance on natural resources, and ecological degradation. Vulnerabilities limit the ability and opportunities of individuals or households to cope with short- and long-term challenges. Substantial evidence exists regarding vulnerabilities related to food security, livelihoods, HIV/AIDS, and natural resource use as well as the particular vulnerabilities of women, children, migrants, and those affected by conflict, which make them disproportionately burdened by the HIV/AIDS–ecosystem degradation syndemic.
The Syndemic
The syndemic interaction between HIV/AIDS and ecological health hinges on the feedback loop in Figure 1. The upstream determinants of poverty, gender inequality, and social disruption influence this cycle, and it begins and ends with vulnerability.
Internal and external vulnerability and decreased coping ability increase the risk of HIV infection through changed behavioral and nonbehavioral risk factors such as malnutrition or infection with sexually transmitted diseases. HIV/AIDS in turn leads to income insecurity and increased dependence on natural resources, as households lose labor force, land tenure, and traditional knowledge and are less able to maintain their previous livelihoods. This increased reliance on natural resources in turn makes communities even more vulnerable, as they become increasingly more exposed to the vagaries of nature, weather, and availability of resources. Infection with HIV/AIDS itself also increases vulnerability, which may lead both to more behavior that increases HIV transmission and to changes in behavior, such as erosive coping, which also increase natural resource use. The cycle is self-reinforcing and reciprocal.
Figure 1 illustrates how the burden of HIV/AIDS feeds back into the upstream determinants, thereby reinforcing a continued cycle of vulnerability and risk. HIV infection feeds back by generating more social disruption as institutions continue to erode, contributing to increased poverty and reinforcing gender inequality. Women are overrepresented among the HIV infected and the HIV affected. Children orphaned by AIDS are often left with few resources, compounding the effect of intergenerational poverty in this feedback loop.
Most of the pathways in Figure 1 have multiple divergence points; there is no single path that all households, communities, or individuals follow. Figure 2 illustrates a possible pathway that starts with land degradation owing to global climate change. Land degradation initiated by global climate change (e.g., shifting rain patterns, extended droughts) decreases food production. Food insecurity decreases coping abilities through hunger or the need to find food for children at any cost, which leads to erosive behavioral changes. If these changes result in transactional or forced sexual contact, the risk of HIV infection increases. Illness associated with HIV/AIDS infection decreases the ability to successfully work or farm, which can lead to increased use of natural resources to fill the gap, which results in an additive, deleterious cycle or feedback loop by further degrading the land.
FIGURE 2—
A synergistic relationship between land degradation, food insecurity, and HIV/AIDS.
Several factors differentiate HIV/AIDS effects from other threats to households or livelihoods. Health care costs for AIDS-related deaths have been shown to be more than are those for non–AIDS-related deaths in Zimbabwe, and AIDS-related deaths were more likely to be heads of household.22 AIDS-related deaths were also more likely to result in dissolution of the household and out-migration. Gender bias, stigma, household clustering, and staging of HIV/AIDS infection differentiate HIV-related illness and mortality from other household shocks.58,62,68,77 Kinship and community safety nets are already overstressed because of excess mortality.86
It is also important to note, however, that this cycle can be completed without ever involving HIV infection. As illustrated in Figure 1, a direct path from the global and upstream determinants, through vulnerabilities, can lead directly to livelihood insecurity and increased reliance on the natural environment, bypassing HIV infection, and can create a second self-reinforcing loop.
Applying the Syndemic Framework
Framing the HIV/AIDS epidemic in the context of a syndemic with ecosystem degradation has a number of advantages. At a practical level, the syndemic orientation facilitates interdisciplinary and cross-sector strategic partnerships, bidirectional mainstreaming of HIV/AIDS and ecological considerations across sectors, and the development of a multifaceted approach to addressing the multiple determinants of the syndemic. For researchers, applying a syndemic lens provides new avenues for addressing risk factors. The focus of most HIV/AIDS research and programs has been on prevention and treatment, with an emphasis on behavior modification. This narrow focus excludes the broader context of the disease and ignores some of the more ultimate, rather than proximate causes of the epidemic. A syndemic framework acknowledges the multifaceted nature of the HIV/AIDS epidemic, which can lead to more successful approaches for combating it. Singer synthesizes the benefits of syndemic research:
[It] focuses simultaneously on distal and proximal causes of disease, specific mechanisms and directionalities of interaction, broader patterns and contexts of vulnerability and risk, and consequences of disease synergies that increase the overall health burden of a population.26(p15)
However, challenges remain in moving forward with research and intervention agendas targeted at maximizing public health environment cobenefits. A disciplinary tension between public health and the environmental sector means that priorities in the public health sector may differ from, and even conflict with, those of environmental organizations. For instance, the public health literature glows about the benefits of wild foods as nutritional supplements for people living with HIV/AIDS, whereas the environmental literature worries about the biodiversity effects of wild food collection. What one field sees as an opportunity, another may perceive as a threat. This difference in perception is illustrated by an experience at Lake Victoria in Kenya. Upon arrival at the lakeshore, one author noted the entrepreneurial energy of various individuals vigorously washing cars, trucks, and buses, thus increasing their incomes and fostering resiliency. Another author noted that Lake Victoria is already an ecological disaster because of invasive species and bemoaned the addition of gasoline, oils, and other toxic materials to the lake from the activity. Neither immediately noticed yet another local health issue: the high rates of infection with schistosomiasis among the car washers.
Challenges for integrative HIV/AIDS environmental projects include limited evidence on their effectiveness, funding issues and sustainability of projects, and developing capacity for integrative responses at the local level.87 Mainstreaming at the institutional and policy levels, using evidence-based research, and using monitored and evaluated interventions to document the added value of integration should be prioritized. The orientation of funding streams toward vertically applied, disease-specific programming should be reevaluated to accommodate integrated projects.
A coherent research and intervention agenda for addressing the HIV/AIDS and environment syndemic is urgently needed, as are more longitudinal, controlled, and comparative data. There has been a clear surge in enthusiasm, activity, and momentum for work on the links between HIV/AIDS and ecosystem integrity. Nonetheless, the vast majority of the evidence remains anecdotal or unreplicated, and specific evidence of the successfulness of integrated interventions is scant.
Specific research needs include further quantification of the impact of HIV/AIDS on natural resource use and livelihoods in a variety of settings and over time. Additionally, both poverty and food insecurity may confound the relationship between HIV infection and increased use of natural resources, and studies that tease out their differential effects will be important. Additional data on indicators of ecological health, such as status and trends of species and indicators of biodiversity, are warranted. Additional quantification and characterization of the impact of HIV/AIDS on conservation workforces are also needed. Furthermore, the relationship between global climate change and the HIV/AIDS pandemic needs further exploration; much of the speculation on how climate change might affect the epidemic is more conjectural than scientific. Continued documentation of actual and potential risks of climate change to health (including HIV/AIDS), livelihoods, and vulnerability is needed.
CONCLUSIONS
HIV/AIDS is inextricably linked to the global effects of environmental change, social disruption, and macroeconomics. HIV/AIDS issues should be incorporated into environmental analyses. Simultaneously, public health research and interventions must consider the many ways HIV/AIDS is tied to ecological health.
A syndemic approach is of use to both researchers and public health practitioners in investigating and crafting a response to the 2 intertwined phenomena. The global effort to address the HIV/AIDS pandemic must widen the lens through which HIV/AIDS is studied, evaluated, and mitigated to include its relationship to ecological health to maximize the benefits of decreased HIV/AIDS risk and improved ecosystem health. As Singer eloquently puts it,
This means advancing past narrowly conceived efforts toward an understanding of the broader socially and environmentally contextualized epidemiological patterns of a specific disease to prevent or control it.26(p15–16)
Adopting a syndemic framework when examining HIV/AIDS and ecosystem health will provide benefits to affected individuals and to the environment much beyond addressing the issues in isolation.
Acknowledgments
This work was made possible by financial support from the Eastern and Southern Africa Regional Office of the International Union for the Conservation of Nature and the International Planned Parenthood Federation Africa Regional Office. Additional support was provided by the University of Washington Department of Global Health and the School of Forest Resources.
Special thanks are due to Tom Hinckley, Ben Piper, Judy Wasserheit, Richard Fenske, Joachim Voss, Adam Akullian, Lawrence Oteba, Jonathan Davies, Claire Ogali, Ben Wandago, and Francis Mwaura for their involvement in every phase of this project, from proposal to article editing.
Human Participant Protection
These activities were conducted in the process of ongoing programmatic planning and evaluation, and because there was no human participants research, no protocol review was required.
References
- 1.Joint United Nations Programme on HIV/AIDS Global Report: UNAIDS Report on the Global AIDS Epidemic. Geneva; 2010 [Google Scholar]
- 2.Barany M, Hammett AL, Sene A, Amichev B. Nontimber forest benefits and HIV/AIDS in sub-Saharan Africa. J Forestry. 2001;99(12):36–41 [Google Scholar]
- 3.Ellis F, Allison E. Livelihood Diversification and Natural Resource Access. Norfolk, UK: Food and Agriculture Organization: Livelihood Support Program; 2004 [Google Scholar]
- 4.Hammarskjöld M. The Environment, Natural Resources and HIV/AIDS. Stockholm: Swedish International Development Cooperation Agency; 2003 [Google Scholar]
- 5.Oglethorpe J, Gelman N. AIDS, women, land, and natural resources in Africa: current challenges. Gend Dev. 2008;16(1):85–100 [Google Scholar]
- 6.Hunter LM, Twine W, Johnson A. Adult mortality and natural resource use in rural South Africa: evidence from the Agincourt health and demographic surveillance site. Soc Nat Resour. 2011;24(3):256–275 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hunter LM, De Souza RM, Twine W. The environmental dimensions of the HIV/AIDS pandemic: a call for scholarship and evidence-based intervention. Popul Environ. 2008;29(3–5):103–107 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ternström I. HIV/AIDS—the true tragedy of the commons? Exploring the effects of HIV/AIDS on management and use of local natural resources. Paper presented at the Workshop on Infectious Disease at the Ecological and Environmental Economics Programme. The Abdus Salam International Centre for Theoretical Physics; Trieste, Italy; April 11–15, 2005.
- 9.Oglethorpe J, Gelman N. HIV/AIDS and the Environment: Impacts of AIDS and Ways to Reduce Them: Fact Sheet for the Conservation Community: Joint United Nations Programme on HIV/AIDS. Washington, DC: World Wildlife Fund; 2006 [Google Scholar]
- 10.Cash JA, McCool SF. Meeting the Challenges of HIV/AIDS in Conservation Agency Workforces: A Technical Guide. Missoula: Consortium of International Protected Area Management, University of Montana; 2007 [Google Scholar]
- 11.Dwasi J. HIV/AIDS and Natural Resource Management in Africa: Findings From Kenya, Namibia, South Africa, and Uganda (Draft). Washington, DC: Africa Biodiversity Collaborative Group; 2002 [Google Scholar]
- 12.Ahmed SA, Diffenbaugh NS, Hertel TW. Climate volatility deepens poverty vulnerability in developing countries. Environ Res Lett. 2009;4(3):1–8 [Google Scholar]
- 13.Bloem MW, Semba RD, Kraemer K. Castel Gandolfo Workshop: an introduction to the impact of climate change, the economic crisis, and the increase in the food prices on malnutrition. J Nutrition. 2010;140(1):132S–135S [DOI] [PubMed] [Google Scholar]
- 14.Costello A, Abbas M, Allen Aet al. Managing the health effects of climate change. Lancet. 2009;373(9676):1693–1733 [DOI] [PubMed] [Google Scholar]
- 15.Baker L. Feeling the Heat: Child Survival in a Changing Climate. London: International Save the Children Alliance; 2009 [Google Scholar]
- 16.Drimie S. AIDS, agriculture and climate change in Southern Africa. Epidemiology. 2009;20(6):S256 [Google Scholar]
- 17.Anema A, Vogenthaler N, Frongillo EA, Kadiyala S, Weiser SD. Food insecurity and HIV/AIDS: current knowledge, gaps, and research priorities. Curr HIV/AIDS Rep. 2009;6(4):224–231 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ambrus JL Sr, Ambrus JL., Jr Nutrition and infectious diseases in developing countries and problems of acquired immunodeficiency syndrome. Exp Biol Med (Maywood). 2004;229(6):464–472 [DOI] [PubMed] [Google Scholar]
- 19.Barany M, Holding-Anyonge C, Kayambazinthu D, Sitoe A. Firewood, food, and medicine: interactions between forests, vulnerability, and rural responses to HIV/AIDS. Paper presented at the International Food Policy Research Institute Conference: HIV/AIDS and Food and Nutrition Security. Durban, South Africa; April 14–16, 2005.
- 20.Allison EH, Seeley JA. HIV and AIDS among fisherfolk: a threat to ‘responsible fisheries’? Fish Fisheries. 2004;5(3):215–234 [Google Scholar]
- 21.Hunter SS, Bulirwa E, Kisseka E. AIDS and agricultural production. Report of a land utilization survey, Masaka and Rakai districts of Uganda. Land Use Policy. 1993;10(3):241–258 [DOI] [PubMed] [Google Scholar]
- 22.Bassett MT, Mhloyi M. Women and AIDS in Zimbabwe: the making of an epidemic. Int J Health Serv. 1991;21(1):143–156 [DOI] [PubMed] [Google Scholar]
- 23.Bene C, Merten S. Women and fish-for-sex: transactional sex, HIV/AIDS and gender in African fisheries. World Dev. 2008;36(5):875–899 [Google Scholar]
- 24.Gibbs A. Gender, famine and HIV/AIDS: rethinking new variant famine in Malawi. Afr J AIDS Res. 2008;7(1):9–17 [DOI] [PubMed] [Google Scholar]
- 25.Centers for Disease Control and Prevention. Definition: Syndemic; 2008. Available at: http://www.cdc.gov/syndemics. Accessed June 15, 2011.
- 26.Singer M. Pathogen–pathogen interaction: a syndemic model of complex biosocial processes in disease. Virulence. 2010;1(1):10–18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Singer M, Clair S. Syndemics and public health: reconceptualizing disease in bio-social context. Med Anthropol Q. 2003;17(4):423–441 [DOI] [PubMed] [Google Scholar]
- 28.Barany ME. Non-Timber Forest Products in the Livelihood and Coping Strategies of Households and Communities Afflicted by HIV/AIDS [MS thesis] Blacksburg, VA: M.S. Forest Products Marketing and Management, Virginia Polytechnic Institute and State University; 2003 [Google Scholar]
- 29.Parker DC, Jacobsen KH, Komwa MK. A qualitative study of the impact of HIV/AIDS on agricultural households in Southeastern Uganda. Int J Environ Res Public Health. 2009;6(8):2113–2138 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Torell E, Tobey J, Thaxton Met al. Examining the linkages between AIDS and biodiversity conservation in coastal Tanzania. Ocean Coast Manag. 2006;49(11):792–811 [Google Scholar]
- 31.Mason NM, Jayne TS, Chapoto A, Myers RJ. A test of the new variant famine hypothesis: panel survey evidence from Zambia. World Dev. 2010;38(3):356–368 [Google Scholar]
- 32.Andrew M, Ainslie A, Shackleton C. Land Use and Livelihoods. Cape Town, South Africa: Programme for Land and Agrarian Studies, School of Government, University of the Western Cape; 2003 [Google Scholar]
- 33.Ngigi MM. A Geographical Study on the HIV/AIDS Pandemic in Kenya [PhD dissertation] Tsukuba, Japan: Graduate School of Life and Environmental Sciences, University of Tsukuba; 2006 [Google Scholar]
- 34.Fox MP, Rosen S, MacLeod WBet al. The impact of HIV/AIDS on labour productivity in Kenya. Trop Med Int Health. 2004;9(3):318–324 [DOI] [PubMed] [Google Scholar]
- 35.Jayne T, Villarreal M, Pingali P, Hemrich G. Interactions Between the Agricultural Sector and the HIV/AIDS Pandemic: Implications for Agricultural Policy. Rome: Agricultural and Development Economics Division, Food and Agriculture Organization of the United Nations; 2004. ESA Working Paper No. 04-06 [Google Scholar]
- 36.Barnett T, Tumushabe J, Bantebya Get al. The social and economic impact of HIV/AIDS on farming systems and livelihoods in rural Africa: some experience and lessons from Uganda, Tanzania and Zambia. J Int Dev. 1995;7(1):163–176 [Google Scholar]
- 37.Kiai W, Mwangi W, Bosire E. The Impact of HIV/AIDS on the Land Issue in Kenya. Nairobi, Kenya: Forest Action Network; 2002 [Google Scholar]
- 38.Drimie S. HIV/AIDS and land: case studies from Kenya, Lesotho, and South Africa. Dev South Afr. 2003;20(5):647–658 [Google Scholar]
- 39.Murphy LL, Harvey P, Silvestre E. How do we know what we know about the impact of AIDS on food and livelihood insecurity? A review of empirical research from rural sub-Saharan Africa. Hum Org. 2005;64(3):265–275 [Google Scholar]
- 40.Kaler A, Alibhai A, Kipp W, Rubaale T, Konde-Lule J. “Living by the hoe” in the age of treatment: perceptions of household well-being after antiretroviral treatment among family members of persons with AIDS. Aids Care. 2010;22(4):509–519 [DOI] [PubMed] [Google Scholar]
- 41.Drimie S, Casale M. Multiple stressors in Southern Africa: the link between HIV/AIDS, food insecurity, poverty and children’s vulnerability now and in the future. Aids Care. 2009;21(suppl 1):28–33 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Rollins N. Food insecurity—a risk factor for HIV infection. PLoS Med. 2007;4(10):e301 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Weiser SD, Leiter K, Bangsberg DRet al. Food insufficiency is associated with high-risk sexual behavior among women in Botswana and Swaziland. PLoS Med. 2007;4(10):e260 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Oyefara JL. Food insecurity, HIV/AIDS pandemic and sexual behaviour of female commercial sex workers in Lagos metropolis, Nigeria. SAHARA J. 2007;4(2):626–635 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Koethe JR, Heimburger DC. Nutritional aspects of HIV-associated wasting in sub-Saharan Africa. Am J Clin Nutr. 2010;91(4):1138S–1142S [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Stillwaggon E. HIV/AIDS in Africa: fertile terrain. J Dev Stud. 2002;38(6):1–22 [Google Scholar]
- 47.Kaschula SA. Wild foods and household food security responses to AIDS: evidence from South Africa. Popul Environ. 2008;29(3–5):162–185 [Google Scholar]
- 48.Onyango AC, Walingo MK, Othuon L. Food consumption patterns, diversity of food nutrients and mean nutrient intake in relation to HIV/AIDS status in Kisumu district Kenya. Afr J AIDS Res. 2009;8(3):359–366 [DOI] [PubMed] [Google Scholar]
- 49.Misselhorn AA. What drives food insecurity in southern Africa? A meta-analysis of household economy studies. Glob Environ Change. 2005;15(1):33–43 [Google Scholar]
- 50.Gillespie S, Kadiyala S, Greener R. Is poverty or wealth driving HIV transmission? AIDS. 2007;21(suppl 7):S5–S16 [DOI] [PubMed] [Google Scholar]
- 51.Mauambeta DDC. HIV/AIDS Mainstreaming in Conservation: The Case of Wildlife and Environmental Society of Malawi. Imbe, Malawi: Wildlife and Environmental Society of Malawi; 2003 [Google Scholar]
- 52.Torell E, Kalangahe B, Thaxton Met al. Guidelines for Mitigating the Impacts of HIV/AIDS on Coastal Biodiversity and Natural Resource Management. Washington, DC: Population Reference Bureau; 2007 [Google Scholar]
- 53.Stillwaggon E. Race, sex, and the neglected risks for women and girls in sub-Saharan Africa. Fem Econ. 2008;14(4):67–86 [Google Scholar]
- 54.Erulkar AS. The experience of sexual coercion among young people in Kenya. Int Fam Plan Perspect. 2004;30(4):182–189 [DOI] [PubMed] [Google Scholar]
- 55.Dodoo FNA, Zulu EM, Ezeh AC. Urban–rural differences in the socioeconomic deprivation—Sexual behavior link in Kenya. Soc Sci Med. 2007;64(5):1019–1031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Shisana O, Davids A. Correcting gender inequalities is central to controlling HIV/AIDS. Bull World Health Organ. 2004;82(11):812. [PMC free article] [PubMed] [Google Scholar]
- 57.Gill TB. Modeling the impact of HIV/AIDS upon food security of diverse rural households in Western Kenya. Agric Syst. 2010;103(5):265–281 [Google Scholar]
- 58.Oglethorpe J, Gelman N. HIV/AIDS and Conservation: What Can the Conservation Sector Do? Washington, DC: World Wildlife Fund, African Biodiversity Collaborative Group, International Union for the Conservation of Nature [Google Scholar]
- 59.Topouzis D, Okong’o M, Tumushabe J. Strategy Paper on HIV/AIDS for East and Southern Africa. Rome: International Fund for Agricultural Development; 2001 [Google Scholar]
- 60.Challe JF, Price LL. Endangered edible orchids and vulnerable gatherers in the context of HIV/AIDS in the southern highlands of Tanzania. J Ethnobiol Ethnomed. 2009;5(1):41–68 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Drimie S. The Impact of HIV/AIDS on Rural Households and Land Issues in Southern and Eastern Africa: A Background Paper Prepared for the Food and Agricultural Organization, Sub-Regional Office for Southern an Eastern Africa. Pretoria, South Africa: Integrated Rural & Regional Development, Human Sciences Research Council; 2002 [Google Scholar]
- 62.Voeten H, Vissers DCJ, Gregson Set al. Strong association between in-migration and HIV prevalence in urban sub-Saharan Africa. Sex Transm Dis. 2010;37(4):240–243 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Ball AM. Making the connections: AIDS and water. Can J Public Health. 2006;97(1):56–59 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Welaga P, Hosegood V, Weiner R, Hill C, Herbst K, Newell ML. Coming home to die? The association between migration and mortality in rural South Africa. BMC Public Health. 2009;9:193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Bremner J. Links Between HIV and … the Environment? Population Reference Bureau; 2009. Available at: http://prbblog.org/?p=69. Accessed June 15, 2012.
- 66.Development Alternatives, Inc AIDS Toolkits: HIV/AIDS and Community-Based Natural Resource Management. Bethesda, MD: US Agency for International Development: Bureau for Africa; 2001 [Google Scholar]
- 67.Dowie M. Conservation refugees. Orion Magazine. Available at: http:orionmagazine.org/index.php/articles/161. Accessed June 15, 2012.
- 68.Iqbal Z, Zorn C. Violent conflict and the spread of HIV/AIDS in Africa. J Polit. 2010;72(1):149–162 [Google Scholar]
- 69.Draulans D, Van Krunkelsven E. The impact of war on forest areas in the Democratic Republic of Congo. Oryx. 2002;36(1):35–40 [Google Scholar]
- 70.Kanyamibwa S. Impact of war on conservation: Rwandan environment and wildlife in agony. Biodivers Conserv. 1998;7(11):1399–1406 [Google Scholar]
- 71.Myers SS, Patz JA. Emerging threats to human health from global environmental change. Annu Rev Environ Resour. 2009;2009(34):223–252 [Google Scholar]
- 72.Battisti DS, Naylor RL. Historical warnings of future food insecurity with unprecedented seasonal heat. Science. 2009;323(5911):240–244 [DOI] [PubMed] [Google Scholar]
- 73.Gregory PJ, Ingram JSI, Brklacich M. Climate change and food security. Philos Trans R Soc B-Biol Sci. 2005;360(1463):2139–2148 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.McMichael AJ, Campbell-Lendrum DH, Corvalán CFet al. Climate Change and Human Health: Risks and Responses. Geneva: World Health Organization, Department of Protection of the Human Environment; 2003 [Google Scholar]
- 75.Abu-Raddad LJ, Patnaik P, Kublin JG. Dual infection with HIV and malaria fuels the spread of both diseases. Science. 2006;314(5805):1603–1606 [DOI] [PubMed] [Google Scholar]
- 76.Ezeaku PI, Alaci D. Analytical situation of land degradation and sustainable management strategies in Africa. J Agric Soc Sci. 2008;4:42–52 [Google Scholar]
- 77.McMichael AJ, Butler CD, Weaver H. Climate Change and AIDS: A Joint Working Paper. Nairobi, Kenya: Joint United Nations Programme on HIV/AIDS; 2008 [Google Scholar]
- 78.Mojola SA. Fishing in dangerous waters: ecology, gender and economy in HIV risk. Soc Sci Med. 2011;72(2):149–156 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.United Nations Development Program Human Development Report 2007/2008: Fighting Climate Change: Human Solidarity in a Divided World. New York; 2007 [Google Scholar]
- 80.Rosen S, Hamazakaza P, Feeley F, Fox M. The impact of AIDS on government service delivery: the case of the Zambia Wildlife Authority. AIDS. 2007;21(suppl 3):S53–S59 [DOI] [PubMed] [Google Scholar]
- 81.Meier B. HIV/AIDS and the Environment: What Are the Linkages? Impacts on Conservation Capacity, an Institutional Perspective. KwaZulu Natal, South Africa: Ezemvelo KwaZulu Natal Wildlife. Human Resources Department Presentation. Available at: www.frameweb.org/adl/en-US/2319/file/220/default.aspx. Accessed October 2, 2012.
- 82.Ngoti PM, Baldus RD. HIV/AIDS and the Wildlife Sector in Tanzania. Dar Es Salaam: GTZ Wildlife Programme in Tanzania; 2004. Tanzania Wildlife Discussion Paper No. 38 [Google Scholar]
- 83.Zelothe J. HIV/AIDS Impacts on Conservation Capacity. Washington, DC: US Agency for International Development; 2008 [Google Scholar]
- 84.Chambers R. Editorial introduction: vulnerability, coping, and policy. IDS Bull. 1989;20(2):1–7 [Google Scholar]
- 85.Chambers RC. Sustainable Rural Livelihoods: Practical Concepts for the 21st Century. Brighton, UK: Institute of Development Studies; 1992. IDS Discussion Paper 296 [Google Scholar]
- 86.Baylies C. The impact of AIDS on rural households in Africa: a shock like any other? Dev Change. 2002;33(4):611–632 [Google Scholar]
- 87.Elsey H, Tolhurst R, Theobald S. Mainstreaming HIV/AIDS in development sectors: have we learnt the lessons from gender mainstreaming? Aids Care. 2005;17(8):988–998 [DOI] [PubMed] [Google Scholar]