

Abstract
Objective
Premature ejaculation (PE) has been reported as the most common male sexual dysfunction with global prevalence rates estimated at approximately 30%. The neurobiogenesis of ejaculation is very complex and involves the serotoninergic (5-hydroxytryptamine, 5-HT) system. Recently, genetic polymorphisms located on SLC6A4 gene codifying for 5-HT transporter (5-HTT), the major regulator of serotonic neurotransmission, have been linked with the pathogenesis and risk of PE. Apparently studies of this type of polymorphism in PE have show conflicting results.
Methods
A meta-analysis was performed that are available in relation with 5-HTT gene-linked promoter region (5-HTTLPR) polymorphism and the risk of lifelong PE (LPE) in men to clarify this relationship. We searched Pubmed and Embase (last search updated on Aug 2012) using ‘premature ejaculation’, ‘polymorphism or variant’, ‘genotype’, ‘ejaculatory function’, and ‘rapid ejaculation’ as keywords and reference lists of studies corresponded to the inclusion criteria for meta-analysis. These studies involved the total number of 481 LPE men and 466 health control men subjects. Odds ratio (OR) and 95% confidence intervals (CIs) were used to evaluate this relationship.
Results
In the overall analysis, significant associations between LPE risk and 5-HTTLPR polymorphism were found (L-allele vs. S-allele OR = 0.86, 95% CI = 0.79–0.95, P = 0.002; LL vs. SS: OR = 0.80, 95% CI = 0.68–0.95, P = 0.009; LS vs. SS: OR = 0.85, 95% CI = 0.76–0.97, P = 0.012 and LL+LS vs. SS: OR = 0.88, 95% CI = 0.81–0.95, P = 0.002). Moreover, in subgroup analysis based on ethnicity, similar significant associations were detected. The Egger’s test did not reveal presence of a publication bias.
Conclusions
Our investigations demonstrate that 5-HTTLPR (L>S) polymorphism might protect men against LPE risk. Further studies based on larger sample size and gene-environment interactions should be conducted the role of 5-HTTLPR polymorphism and LPE risk.
Introduction
Premature ejaculation (PE) is one of the most common male sexual complaints [1]–[2]. In addition to adversely influencing sexual relationships, PE significantly impacts the emotional well being and overall quality of life of both men and their partners [3]. In clinical practice, PE is generally distinguished as primary (lifelong), occurring and persisting from the first sexual intercourse and secondary (acquired), occurring after a period of normal control of ejaculatory function [4].
Lifelong PE (LPE) is defined as a male sexual dysfunction characterized by ejaculation that always or nearly always occurs prior to or within about 1 minute of vaginal penetration, the inability to delay ejaculation on all or nearly all vaginal penetrations, and with negative personal consequences, such as distress, bother, frustration, and/or the avoidance of sexual intimacy [5].
The complete etiology of PE is largely unknown. PE has historically been considered a psychological disorder. However, besides psychological, environmental, and contextual aspects, several published articles have focused on neurobiological, endocrine, and genetic causative factors [6]–[8]. Around 30% of the etiology in PE is due to genetic effects [9].
The successful use of selective serotonin reuptake inhibitors (SSRIs) in the treatment of PE indicates that the classical psychological view of PE is no longer tenable as the only possible pathogenetic theory behind PE, and that serotonin (5-hydroxytryptamine, 5-HT) plays a role in the ejaculation process [10]. These findings suggest that the serotonin transporter (5-HTT) gene is a good candidate for genetic studies of PE.
The 5-HTT functioning is moderated by a polymorphism in the 5-HTT promoter region of the serotonin transporter (SERT) gene (SCL6A4), which encodes for the SERT (5-hydroxytryptamine transporter-linked promoter region [5-HTTLPR]) [11], [12]. The 5-HTTLPR gene has two variant alleles: a short (S) and a long (L) allele. The short allele has 44 base pairs (bps) less than the L allele [13]. The transcriptional activity of the L allele has been reported to be twice as high as the S allele [14]. In vitro studies of the functional effects of this polymorphism show that the long variant is associated with a 3-fold increase in transcriptional activity. It has also been found that levels of serotonin transporter mRNA and serotonin uptake capacity are reduced in lymphoblastoid cell lines that are derived from individuals with one or two copies of the short allele [15].
Several epidemiologic studies have examined associations between 5-HTTLPR gene polymorphism with potential functional significance and risk of LPE [16]–[21]. However, results have been inconsistent across these studies. Some studies reported this gene polymorphism was a risk factor for LPE, however, different opinions were published that this polymorphism was a protect factor or had no relationship for LPE risk. The objective of our study was to examine associations between 5-HTTLPR gene polymorphism and risk of LPE in larger samples by meta-analysis.
Materials and Methods
Search Strategy
We searched the Pubmed and Embase databases for all articles on the association between 5-HTTLPR gene polymorphism and LPE risk up to Aug, 2012. The medical subject headings and key words used for search were ‘premature ejaculation’, ‘polymorphism or variant’, ‘genotype’, ‘ejaculatory function’, and ‘rapid ejaculation’. The electronic searching was supplemented by checking reference lists from the identified articles and reviews for additional original reports.
Inclusion and Exclusion Criteria
Eligible studies had to meet the following criteria: (1) study was designed using the methodology of a case-control study; (2) the association between 5-HTTLPR gene polymorphism and LPE risk was explored; (3) LPE was operationally defined as the lifelong presence of an intravaginal ejaculation latency time (IELT) of 1 minute or less after vaginal penetration occurring an more than 90% of occasions of sexual intercourse with complaints of inability to delay ejaculation and feelings of frustration about it. The major exclusion criteria were: (1) duplicate data, (2) abstract, comment, review and editorial, (3) no sufficient data were reported and (4) The patients with erectile dysfunction and other sexual problems, such as decreased libido, a history of sexual abuse, chronic prostatitis and infravesical obstruction.
Data Abstraction
The following items were collected: first author’s last name, year of publication, country of origin, ethnicity, source of control (hospital-based, HB and population-based, PB) and Hardy–Weinberg equilibrium (HWE) of control group, total number and genotype distributions in cases/controls and the L-allele frequency of control groups.
Statistical Analysis
The strength of the association between the 5-HTTLPR gene polymorphism and LPE risk was measured by odds ratios (ORs) with 95% confidence intervals (CIs). Pooled ORs were obtained from combination of single studies by allelic contrast (L-allele vs. S-allele), homozygote comparison (LL vs. SS), heterozygote comparison (LS vs. SS), and dominant model (LL+LS vs. SS), respectively. The heterogeneity among the studies was checked by using the chisquare based Q statistic and considered statistically significant at P<0.05 [22]. When P>0.05, the pooled OR of each study was calculated by using the fixed-effects model (the Mantel-Haenszel method, which weights the studies by the inverse of the variance of estimates); otherwise, the random-effects model (the DerSimonian and Laird method) was used [23], [24]. The significance of the pooled OR was determined by the Z-test, and P<0.05 was considered statistically significant. The departure of frequencies of 5-HTTLPR gene polymorphism from expectation under HWE was assessed by the chi-square test in controls and a P<0.05 was considered as significant disequilibrium. Publication bias was diagnosed with Egger’s linear regression method and funnel plot. The P-value less than 0.05 in Egger’s linear regression indicated the presence of potential publication bias [25]. All statistical tests for this meta-analysis were performed with Stata software, version 10.0 (STATA Corp., College Station, TX, USA), and all tests were two-sided.
Results
Studies Characteristics
A total of 23 articles were achieved by literature search from the Pubmed and Embase, using different combinations of key terms. As shown in Fig. 1 , seventeen eligible studies were retrieved for abstract review. We excluded six studies: one article type was letter; five were not about polymorphism and LPE. After that, eleven potentially relevant studies were left for full article review. Also six studies were excluded: four were about other genes and/or other SNPs [dopamine transporter gene (SLC6A3, DAT1), serotonic (2C, 1B) receptor gene]; one was not case-control study. In only study by Safarinejad et al. [16], the author further divided the L-allele into LA and LG variants. In our study, we combined these two variants together as L-allele. Finally, six studies with 481 LPE cases and 466 health controls were retrieved based on the search criteria. Characteristics of studies in this meta-analysis are included in Table 1 . Of these studies, only one was conducted on Asian descendants and five on Caucasian descendants. All studies used the same genotyping method: polymerase chain reaction-based restriction fragment length polymorphism (PCR-RFLP). With the exception of two studies [16], [20], the distribution of genotypes in the controls was consistent with the HWE.
Figure 1. Flow chart of selection of studies and specific reasons for exclusion from the meta-analysis.
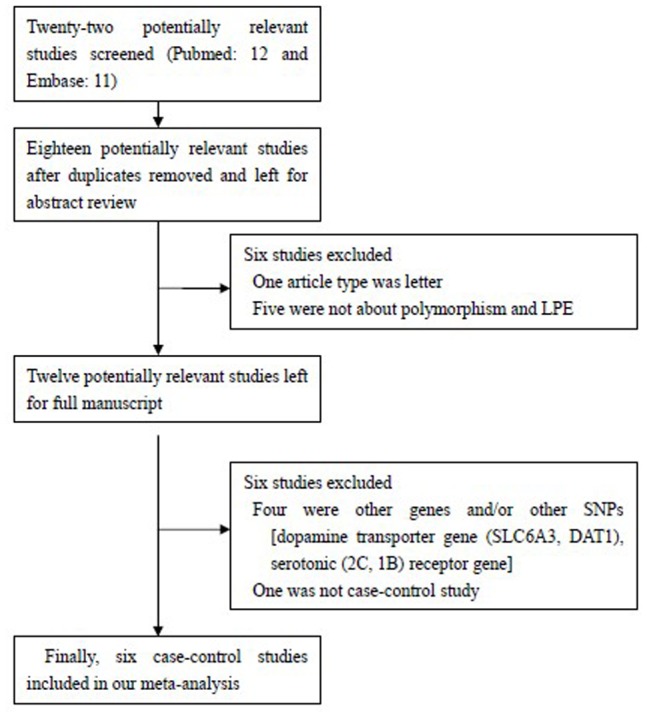
Table 1. Characteristics of studies of 5-HTTLPR polymorphism included in this meta-analysis.
| First author/Year | Country | Ethnicity | Source of control | Cases/Controls | Cases | Controls | ||
| LL/LS/SS | LL/LS/SS | HWE | L% | |||||
| Safarinejad/2009 | Iran | Caucasian | PB | 82/82 | 24/29/29 | 35/30/17 | No | 0.61 |
| Janssen/2009 | the Netherlands | Caucasian | HB | 89/92 | 27/43/19 | 27/41/24 | Yes | 0.52 |
| Luo/2011 | China | Asian | HB | 119/90 | 24/34/61 | 25/31/34 | No | 0.45 |
| Ozbek/2009 | Tukey | Caucasian | PB | 69/69 | 11/21/37 | 12/37/20 | Yes | 0.44 |
| Zuccarello/2012 | Italy | Caucasian | PB | 89/100 | 22/49/18 | 33/51/16 | Yes | 0.59 |
| Jern/2012 | Finland | Caucasian | PB | 33/33 | 13/15/5 | 12/16/5 | Yes | 0.61 |
Meta-analysis
In the overall analysis, significantly decreased associations could be observed between LPE risk and the 5-HTTLPR gene polymorphism in different genetic models: allelic contrast (OR = 0.86, 95% CI = 0.79–0.95, P heterogeneity = 0.086, P = 0.002), homozygote comparison (OR = 0.80, 95% CI = 0.68–0.95, P heterogeneity = 0.240, P = 0.009), heterozygote comparison (OR = 0.85, 95% CI = 0.76–0.97, P heterogeneity = 0.047, P = 0.012), and dominant genetic model (OR = 0.88, 95% CI = 0.81–0.95, P heterogeneity = 0.020, P = 0.002) ( Table 2 ).
Table 2. Stratified analyses of 5-HTTLPR gene polymorphism on LPE risk.
| Variables | Na | Cases/Controls | Allelic contrast | Homozygote comparison | Heterozygote comparison | Dominant genetic model |
| OR(95%CI) P b/P | OR(95%CI) P b/P | OR(95%CI) P b/P | OR(95%CI) P b/P | |||
| Total | 6 | 481/466 | 0.86(0.79–0.95)0.086/0.002 | 0.80(0.68–0.95)0.240/0.009 | 0.85(0.76–0.97)0.047/0.012 | 0.88(0.81–0.95)0.020/0.002 |
| Ethnicity | ||||||
| Asian | 1 | 119/90 | 0.64(0.43–0.96)−/0.029 | 0.54(0.27–1.08)−/0.080 | 0.61(0.32–1.16)−/0.133 | 1.47(0.77–2.78)−/0.067 |
| Caucasian | 5 | 362/376 | 0.88(0.80–0.98)0.086/0.015 | 0.83(0.70–1.00)0.228/0.046 | 0.88(0.77–1.00)0.040/0.043 | 0.90(0.83–0.98)0.024/0.015 |
| Source of control | ||||||
| HB | 2 | 208/182 | 0.91(0.78–1.06)0.039/0.229 | 0.87(0.66–1.15)0.077/0.339 | 0.93(0.75–1.15)0.083/0.518 | 0.93(0.80–1.07)0.032/0.294 |
| PB | 4 | 273/284 | 0.83(0.74–0.93)0.213/0.002 | 0.76(0.61–0.93)0.395/0.008 | 0.81(0.70–0.94)0.056/0.006 | 0.85(0.77–0.94)0.042/0.001 |
In the stratified analysis by ethnicity subgroup, significantly decreased associations were also found between LPE risk and 5-HTTLPR gene polymorphism in Caucasians not Asians: allelic contrast (OR = 0.88, 95% CI = 0.80–0.98, P heterogeneity = 0.086, P = 0.015), homozygote comparison (OR = 0.83, 95% CI = 0.70–1.00, P heterogeneity = 0.228, P = 0.046, Fig. 2 ), heterozygote comparison (OR = 0.88, 95% CI = 0.77–1.00, P heterogeneity = 0.040, P = 0.043), and dominant genetic model (OR = 0.90, 95% CI = 0.83–0.98, P heterogeneity = 0.024, P = 0.015, Fig. 3 ) (Table 2). Similarly, obvious relationships were detected between LPE risk and 5-HTTLPR gene polymorphism in PB source of controls groups ( Table 2 ).
Figure 2. Forest plot of LPE risk associated with the 5-HTTLPR gene polymorphism (LL vs. SS) by ethnicity subgroup.
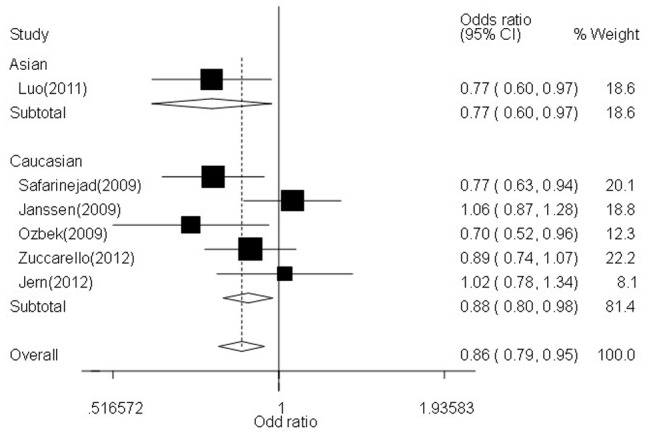
The squares and horizontal lines correspond to the study-specific OR and 95% CI. The area of the squares reflects the weight (inverse of the variance). The diamond represents the summary OR and 95% CI.
Figure 3. Forest plot of LPE risk associated with the 5-HTTLPR gene polymorphism (LL +LS vs. SS) by ethnicity subgroup.
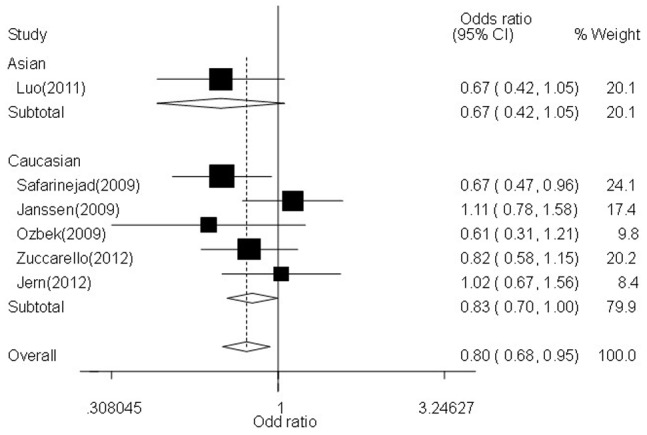
The squares and horizontal lines correspond to the study-specific OR and 95% CI. The area of the squares reflects the weight (inverse of the variance). The diamond represents the summary OR and 95% CI.
Sensitivity Analysis and Publication Bias
Sensitivity analysis was performed to assess the influence of each individual study on the pooled OR by sequential removal of individual studies. Although the genotype distributions in two studies [16], [20] did not follow the HWE, the corresponding overall summary OR was not significantly altered with/without including the study (data not shown). The results suggested that no individual study significantly affected the overall OR dominantly. The Begg’s funnel plot and Egger’s test were performed to assess publication bias. As shown in Table 3, the shapes of the funnel plots did not reveal any obvious asymmetry in any of the comparison models. Then, the Egger’s test was used to provide statistical evidence of funnel plot symmetry. The results still did not suggest any evidence of publication bias (allelic contrast, t = −0.74, P = 0.501, homozygote comparison, t = −0.76, P = 0.491; heterozygote comparison, t = −1.94, P = 0.124, and dominant genetic model, t = −2.22, P = 0.091, Table 3 ).
Table 3. Publication bias tests (Begg’s funnel plot for publication bias test).
| Genetic type | Coefficient | Standard error | t | P value | 95%CI of intercept |
| Allelic contrast | −2.437 | 3.300 | −0.74 | 0.501 | (−11.599,6.726) |
| Homozygote comparison | −1.812 | 2.394 | −0.76 | 0.491 | (−8.457,4.834) |
| Heterozygote comparison | −3.589 | 1.846 | −1.94 | 0.124 | (−8.715,1.536) |
| Dominant genetic model | −4.313 | 1.946 | −2.22 | 0.091 | (−9.715,1.089) |
Discussion
The overall goal of meta-analysis is to combine the results of previous studies to arrive at summary conclusions about a body of research. It is most useful in summarizing prior research when individual studies are small, and when they are individually too small to yield a valid conclusion. To the best of our knowledge, this is the first meta-analysis to explore the association between 5-HTTLPR gene polymorphism and LPE risk, involving about 481 LPE individuals and 466 healthy controls. The main finding of this study is that LL genotype and/or L-allele in 5-HTTLPR gene polymorphism could protect individuals against LPE risk in Caucasian populations.
While our study provided convincing evidence that this polymorphism played a part in ejaculatory function in humans, it only explains a fraction of the etiological variance in LPE, because the neurobiogenesis of ejaculation is very complex [26], [27]. Waldinger et al. first postulated that the persistent short IELT in men with PE was associated with diminished serotonin neurotransmission, hyperfunction of 5-HT1A receptors, and a hypofunction of 5-HT2C receptors [28]. The function of 5-HT in the central nervous system are controlled by many factors including the 5-HTT, the major regulator of serotonergic neurotransmission, responsible for the active clearance of synaptic 5-HT and then regulation of presynaptic and postsynaptic 5-HT receptor stimulations [8]. The expression rate of 5-HTT is controlled by the 5-HTTLPR polymorphism [29].
The current most popular pharmacotherapeutic approach to treat PE is ‘off-label’ administration of SSRIs (e.g. paroxetine, fluoxetine, sertraline, citalopram, and escitalopram), which are reported to be effective for treating PE [30]–[32]. It was previously suggested that the response to SSRIs is partly under genetic control [33]. It has been shown that the 5-HTTLPR also influences the effectiveness of SSRIs in patients with depression. White L-allele carriers demonstrated higher response rates when treated with various SSRIs antidepressants [34]. Patients with the 5-HTTLPR SS and/or SL genotype have a higher risk of SSRI non-response [33]. Moreover, previous studies have revealed an association between the occurrence of adverse events during SSRIs treatment and different serotonin transporter genotypes [35], [36]. Evidence suggests that 5-HTTLPR gene polymorphism moderates the relationships between affective outcomes and major life events [37]. It is known that the S-allele induces lower 5HTT expression and 5HT reuptake activity than the L-allele [38].
Several epidemiological studies have investigated the association between 5-HTTLPR gene polymorphism and PE/LPE, but the results were inconclusive. Janssen et al. [17] reported that no association was found between this polymorphism and LPE, however, men carried SS or SL genotype had longer ejaculation time that LL genotype. Similarly, Zuccarello et al. [19] also reported that no statistically significant differences were found in the frequency of 5-HTTLPR gene polymorphism in LPE patients vs. controls. In contrast, two studies [18], [20] suggested the SS genotype was significantly higher in patients with PE than in the controls (P<0.01), however, the LS genotype was more prevalent in the control group (P<0.01). Our study showed partly similar conclusions with above two studies. However, two included studies [16], [18] have previously been criticized for potential methodological limitations that the populations of both studies were not in HWE. [39]–[41]. While this criticismis obviously potentially valid, however, it should be pointed out that deviation from HWE is not necessarily indicative of sampling inadequacy or neglect, since neither allele nor genotype frequencies are free from disturbing influences in nature [42]. For example, non-randommating, migration and natural selection will distort allele (and thus genotype) frequencies in populations [43].
We first analyzed the overall association between 5-HTTLPR gene polymorphism and LPE: LL genotype or L-allele was a protect factor for LPE. Because of the coupled and complementary association between L-allele and S-allele, in contrast, SS genotype and/or S-allele were risk factors of LPE. Then, we analyzed the association stratified analysis by ethnicity, the similar conclusion was found in Asians not Caucasians, which can be explained that the prevalence of PE is different in distinct geographic locations and ethnicities. The Global Study of Sexual Attitudes and Behaviors (GSSAB) reported a PE prevalence ranging from 12% in the Middle East to 30% in Southeast Asia among men 40–80 years of age [44]. In a separate study of men between the ages of 18 and 59 years in the United States, the overall prevalence of PE was 21%, which comprised 19% of Caucasian men, 27% of Hispanic men, and 34% of African-American men [45]. Finally, in case-control studies whose controls were from PB, significant association was also found. Our study may help scientists to detect this SNP in 5-HTTLPR gene in healthy men and to find high-risk group of PE in the future.
Although, we have put considerable efforts and resources into testing possible association between 5-HTTLPR gene polymorphism and LPE risk, there are still some limitations inherited from the published studies. First, although we collected all the eligible studies, the sample size of the included studies was not large enough, which could increase the likehood of type I and type II errors. Second, gene-gene and gene-environment interactions were not analyzed. It is possible that specific environmental and lifestyle factors may alter those associations between gene polymorphism and LPE. Third, the distribution of genotypes in the controls of two studies [16], [20] was not consistent with the HWE, which would affect the power of our conclusions. In spite of these, our meta-analysis also had four advantages. First, publication bias was not detected in all genetic models, suggesting that the results were relatively stable and powerful. Second, the quality of case–control studies included in the current meta-analysis was satisfactory based on our selection criteria. Third, the control groups were all healthy men. Fourth, the included studies were published from 2009 to 2012 and quite neoteric.
Conclusions
In summary, in the present, our meta-analysis showed the evidence that 5-HTTLPR gene polymorphism was associated with significantly decreased risk for LPE risk in Caucasians. Therefore, further well designed large studies, particularly referring to gene–gene and gene–environment interactions are warranted. These future studies should lead to better and comprehensive understanding of the association between the 5-HTTLPR gene polymorphism and development of LPE.
Funding Statement
This study was supported by the National Nature Science Foundation of China (Grant No.81272831), Nature Science Foundation of Jiangsu Province (NO.BK2010577) and Jiangsu Province’s Outstanding Medical Academic Leader program (RC201178). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1. Althof SE, Abdo CH, Dean J, Hackett G, McCabe M, et al. (2010) International Society for Sexual Medicine’s guidelines for the diagnosis and treatment of premature ejaculation. J Sex Med 7: 2947–2969. [DOI] [PubMed] [Google Scholar]
- 2. Rowland D, McMahon CG, Abdo C, Chen J, Jannini E, et al. (2010) Disorders of orgasm and ejaculation in men. J Sex Med 7: 1668–1686. [DOI] [PubMed] [Google Scholar]
- 3. Rosen RC, Althof S (2008) Impact of premature ejaculation: the psychological, quality of life, and sexual relationship consequences. J Sex Med 5: 1296–1307. [DOI] [PubMed] [Google Scholar]
- 4. Godpodinoff ML (1989) Premature ejaculation: clinical subgroups and etiology. J Sex Marital Ther 15: 130–134. [DOI] [PubMed] [Google Scholar]
- 5. McMahon CG, Althof SE, Waldinger MD, Porst H, Dean J, et al. (2008) An evidence-based definition of lifelong premature ejaculation: report of the International Society for Sexual Medicine (ISSM) ad hoc committee for the definition of premature ejaculation. J Sex Med 5: 1590–1606. [DOI] [PubMed] [Google Scholar]
- 6. Corona G, Jannini EA, Mannucci E, Fisher AD, Lotti F, et al. (2008) Different testosterone levels are associated with ejaculatory dysfunction. J Sex Med 5: 1991–1998. [DOI] [PubMed] [Google Scholar]
- 7. Jern P, Santtila P, Witting K, Alanko K, Harlaar N, et al. (2007) Premature and delayed ejaculation: genetic and environmental effects in a population-based sample of Finnish twins. J Sex Med 4: 1739–1749. [DOI] [PubMed] [Google Scholar]
- 8. Waldinger MD (2002) The neurobiological approach to premature ejaculation. J Urol 168: 2359–2367. [DOI] [PubMed] [Google Scholar]
- 9. Jern P, Santtila P, Johansson A, Varjonen M, Witting K, et al. (2009) Evidence for a genetic etiology to ejaculatory dysfunction. Int J Impot Res 2009 21: 62–67. [DOI] [PubMed] [Google Scholar]
- 10. Waldinger MD, Hengeveld MW, Zwinderman AH, Olivier B (1998) Effect of SSRI antidepressants on ejaculation: a double-blind, randomized, placebo-controlled study with fluoxetine, fluvoxamine, paroxetine, and sertraline. J Clin Psychopharmacol 18: 274–281. [DOI] [PubMed] [Google Scholar]
- 11. Smith GS, Lotrich FE, Malhotra AK, Lee AT, Ma Y, et al. (2004) Effects of serotonin transporter promoter polymorphisms on serotonin function. Neuropsychopharmacology 29: 2226–2234. [DOI] [PubMed] [Google Scholar]
- 12. Smits KM, Smits LJ, Schouten JS, Stelma FF, Nelemans P, et al. (2004) Influence of SERTPR and STin2 in the serotonin transporter gene on the effect of selective serotonin reuptake inhibitors in depression: a systematic review. Mol Psychiatry 9: 433–441. [DOI] [PubMed] [Google Scholar]
- 13. Heils A, Teufel A, Petri S, Stöber G, Riederer P, et al. (1996) Allelic variation of human serotonin transporter gene expression. J Neurochem 66: 2621–2624. [DOI] [PubMed] [Google Scholar]
- 14. Lesch KP (2004) Gene-environment interaction and the genetics of depression. J Psychiatry Neurosci 29: 174–184. [PMC free article] [PubMed] [Google Scholar]
- 15. Waldinger MD, Hengeveld MW, Zwinderman AH (1994) Paroxetine treatment of premature ejaculation: a double-blind, randomized, placebo-controlled study. Am J Psychiatry 151: 1377–1379. [DOI] [PubMed] [Google Scholar]
- 16. Safarinejad MR (2009) Polymorphisms of the serotonin transporter gene and their relation to premature ejaculation in individuals from Iran. J Urol 181: 2656–2661. [DOI] [PubMed] [Google Scholar]
- 17. Janssen PK, Bakker SC, Réthelyi J, Zwinderman AH, Touw DJ, et al. (2009) Serotonin transporter promoter region (5-HTTLPR) polymorphism is associated with the intravaginal ejaculation latency time in Dutch men with lifelong premature ejaculation. J Sex Med 6: 276–284. [DOI] [PubMed] [Google Scholar]
- 18. Ozbek E, Tasci AI, Tugcu V, Ilbey YO, Simsek A, et al. (2009) Possible association of the 5-HTTLPR serotonin transporter promoter gene polymorphism with premature ejaculation in a Turkish population. Asian J Androl 11: 351–355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Zuccarello D, Ghezzi M, Pengo M, Forzan M, Frigo AC, et al. (2012) No Difference in 5-HTTLPR and Stin2 Polymorphisms Frequency Between Premature Ejaculation Patients and Controls. J Sex Med 9: 1659–1668. [DOI] [PubMed] [Google Scholar]
- 20. Luo SW, Wang F, Xie ZY, Huang XK, Lu YP (2011) Study on the correlation of the 5-HTTLPR polymorphism with premature ejaculation in Han Chinese population. Beijing Da Xue Xue Bao 43: 514–518. [PubMed] [Google Scholar]
- 21. Jern P, Eriksson E, Westberg L (2013) A Reassessment of the Possible Effects of the Serotonin Transporter Gene Linked Polymorphism 5-HTTLPR on Premature Ejaculation. Arch Sex Behav 42: 45–49. [DOI] [PubMed] [Google Scholar]
- 22. Higgins JP, Thompson SG (2002) Quantifying heterogeneity in a meta-analysis. Stat Med 21: 1539–1558. [DOI] [PubMed] [Google Scholar]
- 23. Mantel N, Haenszel W (1959) Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst 22: 719–748. [PubMed] [Google Scholar]
- 24. DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7: 177–188. [DOI] [PubMed] [Google Scholar]
- 25. Hayashino Y, Noguchi Y, Fukui T (2005) Systematic evaluation and comparison of statistical tests for publication bias. J Epidemiol 15: 235–243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Andrews PW, Thomson JA Jr, Amstadter A, Neale MC (2012) Primum non nocere: an evolutionary analysis of whether antidepressants do more harm than good. Front Psychol 3: 117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Patel K, Hellstrom WJ (2009) Central regulation of ejaculation and the therapeutic role of serotonergic agents in premature ejaculation. Curr Opin Investig Drugs 10: 681–690. [PubMed] [Google Scholar]
- 28. Waldinger MD, Berendsen HH, Blok BF, Olivier B, Holstege G (1998) Premature ejaculation and serotonergic antidepressants-induced delayed ejaculation: the involvement of the serotonergic system. Behav Brain Res 92: 111–118. [DOI] [PubMed] [Google Scholar]
- 29. Collier DA, Stöber G, Li T, Heils A, Catalano M, et al. (1996) A novel functional polymorphism within the promoter of the serotonin transporter gene: possible role in susceptibility to affective disorders. Mol Psychiatry 1: 453–460. [PubMed] [Google Scholar]
- 30. Safarinejad MR (2007) Safety and efficacy of escitalopram in the treatment of premature ejaculation: a double-blind, placebo-controlled, fixed-dose, randomized study. J Clin Psychopharmacol 27: 444–450. [DOI] [PubMed] [Google Scholar]
- 31. Safarinejad MR (2006) Hosseini SY. Safety and efficacy of citalopram in the treatment of premature ejaculation: a double-blind placebo-controlled, fixed dose, randomized study. Int J Impot Res 18: 164–169. [DOI] [PubMed] [Google Scholar]
- 32. Safarinejad MR (2006) Comparison of dapoxetine versus paroxetine in patients with premature ejaculation: a double-blind, placebo-controlled, fixed-dose, randomized study. Clin Neuropharmacol 29: 243–252. [DOI] [PubMed] [Google Scholar]
- 33. Smits KM, Smits LJ, Schouten JS, Stelma FF, Nelemans P, et al. (2004) Influence of SERTPR and STin2 in the serotonin transporter gene on the effect of selective serotonin reuptake inhibitors in depression: a systematic review. Mol Psychiatry 9: 433–441. [DOI] [PubMed] [Google Scholar]
- 34. Kirchheiner J, Nickchen K, Bauer M, Wong ML, Licinio J, et al. (2004) Pharmacogenetics of antidepressants and antipsychotics: the contribution of allelic variations to the phenotype of drug response. Mol Psychiatry 9: 442–473. [DOI] [PubMed] [Google Scholar]
- 35. Murphy GM Jr, Kremer C, Rodrigues HE, Schatzberg AF (2003) Pharmacogenetics of antidepressant medication intolerance. Am J Psychiatry 160: 1830–1835. [DOI] [PubMed] [Google Scholar]
- 36. Popp J, Leucht S, Heres S, Steimer W (2006) Serotonin transporter polymorphisms and side effects in antidepressant therapy–a pilot study. Pharmacogenomics 7: 159–166. [DOI] [PubMed] [Google Scholar]
- 37. Caspi A, Sugden K, Moffitt TE, Taylor A, Craig IW, et al. (2003) Influence of life stress on depression: moderation by a polymorphism in the 5-HTT gene. Science 301: 386–389. [DOI] [PubMed] [Google Scholar]
- 38. Lesch KP, Bengel D, Heils A, Sabol SZ, Greenberg BD, et al. (1996) Association of anxiety-related traits with a polymorphism in the serotonin transporter gene regulatory region. Science 274: 1527–1531. [DOI] [PubMed] [Google Scholar]
- 39. Waldinger MD, Janssen PK, Schweitzer DH (2009) Re: Polymorphisms of the serotonin transporter gene and their relation to premature ejaculation in individuals from Iran. J Urol 182: 2983–2984. [DOI] [PubMed] [Google Scholar]
- 40. Waldinger MD, Janssen PK, Schweitzer DH (2009) Hardy Weinberg equilibrium in genetic PE research remains critical to avoid misinterpretation. Asian J Androl 11: 524–525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Waldinger MD (2011) Toward evidence-based genetic research on lifelong premature ejaculation: a critical evaluation of methodology. Korean J Urol 52: 1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Griffiths AJF, Gelbart WM, Miller JH, Lewontin RC (2002). Moderngenetic analysis: Integrating genes and genomes (2nded.). New York: W. H. Freeman and Co. 102 p.
- 41. Wigginton JE, Cutler DJ, Abecasis GR (2005) A note on exact tests of Hardy-Weinberg equilibrium. Am J Hum Genet 76: 887–893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Laumann EO, Nicolosi A, Glasser DB, Paik A, Gingell C, et al. (2005) Sexual problems among women and men aged 40–80 y: prevalence and correlates identified in the Global Study of Sexual Attitudes and Behaviors. Int J Impot Res 17: 39–57. [DOI] [PubMed] [Google Scholar]
- 43. Laumann EO, Paik A, Rosen RC (1999) Sexual dysfunction in the United States: prevalence and predictors. JAMA 281: 537–544. [DOI] [PubMed] [Google Scholar]