

Abstract
Introduction
Analogous to the business model of customer satisfaction and retention, patient satisfaction could serve as an innovative, patient-centered focus for increasing retention in HIV care and adherence to HAART, and ultimately HIV suppression.
Objective
To test, through structural equation modeling (SEM), a model of HIV suppression in which patient satisfaction influences HIV suppression indirectly through retention in HIV care and adherence to HAART.
Methods
We conducted a cross-sectional study of adults receiving HIV care at two clinics in Texas. Patient satisfaction was based on two validated items, one adapted from the Consumer Assessment of Healthcare Providers and Systems survey (“Would you recommend this clinic to other patients with HIV?) and one adapted from the Delighted-Terrible Scale, (“Overall, how do you feel about the care you got at this clinic in the last 12 months?”). A validated, single-item question measured adherence to HAART over the past 4 weeks. Retention in HIV care was based on visit constancy in the year prior to the survey. HIV suppression was defined as plasma HIV RNA <48 copies/mL at the time of the survey. We used SEM to test hypothesized relationships.
Results
The analyses included 489 patients (94% of eligible patients). The patient satisfaction score had a mean of 8.5 (median 9.2) on a 0- to 10- point scale. A total of 46% reported “excellent” adherence, 76% had adequate retention, and 70% had HIV suppression. In SEM analyses, patient satisfaction with care influences retention in HIV care and adherence to HAART, which in turn serve as key determinants of HIV suppression (all p<.0001).
Conclusions
Patient satisfaction may have direct effects on retention in HIV care and adherence to HAART. Interventions to improve the care experience, without necessarily targeting objective clinical performance measures, could serve as an innovative method for optimizing HIV outcomes.
Introduction
Over 1.1 million people in the United States (US) live with HIV infection [1]. Poor retention in HIV care and suboptimal adherence to highly active antiretroviral therapy (HAART) remain major barriers to maximizing the benefit of effective treatment. Only about 60% of patients who know their HIV status get regular care [2]. Furthermore, among North American patients who access care and receive HAART, only about 55% take their medicines as prescribed [3]. Subsequently, despite the wide availability of effective treatment in the US, only approximately 1 in 4 patients with HIV infection achieve suppression of HIV replication [4]. Suboptimal HIV suppression carries serious individual and public health consequences, including the emergence of drug resistance, increased HIV-related complications, increased infectivity and secondary transmission, and worse survival [5], [6]. Thus, there is an urgent need to optimize HIV outcomes with interventions to retain patients in HIV care and promote adherence to HAART.
The business world offers a framework for increasing retention by focusing on customer satisfaction. Marketing studies clearly show that high satisfaction levels have a positive impact on customer loyalty, repeat patronage, and more extensive and favorable referrals [7]. Firms that appreciate this relationship view customer satisfaction as a useful metric for mapping customer retention strategies.
Analogous to the business model of customer satisfaction and retention, patient satisfaction could serve as an innovative focus for increasing retention in HIV care and adherence to HAART. Suppression of HIV replication represents the most important prognostic indicator for long-term survival with HIV infection. We sought to understand if patient satisfaction is related to suppression of HIV replication through its effects on retention in HIV care and adherence to HAART. We hypothesize that patient satisfaction positively impacts retention in HIV care and adherence to HAART, which in turn impact HIV suppression.
Methods
Study population
We used data from a cross-sectional study of patients receiving outpatient HIV primary care at Thomas Street Health Center (TSHC) and the Michael E. DeBakey Veterans Affairs Medical Center (VAMC) in Houston, Texas. This study took place within the context of a primary study to identify the drivers of overall satisfaction in patients receiving HIV primary care. A full description of the study design is described elsewhere [8]. The study detailed here was planned prior to primary data collection and represents the second phase of analysis. From January 13 to April 21, 2011, study staff screened all patients with a scheduled HIV primary care visit to preliminarily determine study eligibility. Eligibility requirements included: 1) age ≥18 years old; 2) time enrolled in clinic ≥1 year; and 3) having at least one HIV primary care visit in the past year. Patients incarcerated >30 days in the past year or who could not complete the survey due to mental, physical or language barriers were excluded from the study. Clinic exposure requirements ensured sufficient experience at the clinic to assess satisfaction over a 12-month time frame.
Due to limited study staff, we could not recruit all eligible patients concurrently. As such, we decided a priori to systematically sample patients from a list of eligible patients who had arrived at the clinic and checked in. Patients with the most recent check-in time at the time of study staff availability were approached for enrollment. The survey, available in English and Spanish, was administered prior to the HIV provider visit and took about 10 minutes to complete.
Measures
Overall patient satisfaction
The survey instrument included 2 questions about overall care received in the clinic 1) “Overall, how do you feel about the care you got at this clinic in the past 12 months?” and 2) “Would you recommend this clinic to other patients with HIV?” These questions were adapted from validated patient self-report survey instruments [9], [10]. We converted responses for each question to a 0- to 10-point scale. Overall patient satisfaction was measured by averaging the response values of these 2 questions. Construct reliability was evaluated by calculating composite reliability and average variance extracted. We used recommended thresholds of 0.70 and 0.50, respectively [11]–[14].
Medication adherence
A validated, single-item measure assessed adherence to HAART. The item stated, “Many patients find it hard to take HIV medicines as their doctor prescribes them. In the past 4 weeks, how would you rate your ability to take all your HIV medicines as your doctor prescribed?” The 6-point response scale ranged from “very poor” to “excellent” [15], [16]. This item has been validated against medication event monitoring system data, an objective measure of adherence [15], and has an estimated reliability of 0.67 (personal communication, Y. Lee, 2012).
Retention in care
Since 2011, the US Department of Health and Human Services has recognized that patients with HIV suppression and a CD4 cell count well above the threshold for risk of opportunistic infection may need less intensive monitoring (e.g. clinicians may extend the interval for HIV RNA monitoring to every 6 months) [17]. Our definition of adequate versus inadequate retention in HIV care reflects clinical practice, where patients with stable clinical and immunological status can have follow-up intervals of 6 months (as opposed to the traditional 3–4 months). Retention in care was based on 1) the number of 3-month quarters with at least 1 completed HIV primary care visit in the year prior to survey completion (i.e. visit constancy) [18], and 2) HIV RNA and CD4 cell count results 1 year prior to survey completion ±60 days. Because some participants may be seen at imprecise intervals, and the last interval was bounded by the enrollment date, we extended the first quarter interval by 2 weeks on the front end. Patients with adequate retention in care had 1) 3 or 4 quarters with an HIV primary care provider visit, or 2) at least 2 quarters with an HIV primary care provider visit and HIV suppression 1 year prior to survey completion, or 3) at least 2 quarters with an HIV primary care provider visit, and both a CD4 cell count ≥500 and not yet prescribed HAART 1 year prior to survey completion. Patients not meeting these criteria were classified as having inadequate retention in HIV care.
HIV suppression
HIV suppression was defined as a plasma HIV RNA <48 copies/mL±30 days from the date of survey completion. Lab values were obtained from electronic medical records.
Other measures
Participants self-reported their gender, race, ethnicity, education, income, health status and incarceration history. The health status item was based on a validated, widely used question, “In general, how would you rate your overall health?” [10], [19]–[21]. The 5-point response scale ranged from “poor” to “excellent.” Validated, single-item questions identified participants with possible depression, excessive alcohol use, and illegal or prescription drug abuse [22]–[24]. Electronic medical and administrative records provided data on age, appointments and laboratory values (CD4 cell count and HIV RNA).
Statistical Analysis
Relationship between Patient Satisfaction and Adherence to HIV Care
We compared overall patient satisfaction scores between participants with adequate versus inadequate retention in HIV care, “excellent” versus non-“excellent” adherence to HAART, and suppressed versus unsuppressed HIV replication using the Wilcoxon Rank-Sum Test.
Bivariate analyses
We performed bivariate analyses between potential control variables (demographic, health status, behavioral characteristics, and clinic utilization variables listed in Table 1) and all dependent variables in the structural equation model (patient satisfaction, retention in HIV care, adherence to HAART and HIV suppression). To be parsimonious in selecting control variables, we included only variables achieving a significance level of p<0.10 in bivariate analyses with at least 2 of the 4 dependent variables.
Table 1. Baseline characteristics of participants (N = 489).
| Characteristics | |
| Age, years – mean (±SD) | 48 (±11) |
| Gender – (%) | |
| Male | 71 |
| Female | 29 |
| Race ethnicity – (%) | |
| Non-Hispanic black | 61 |
| Non-Hispanic white | 15 |
| Hispanic | 21 |
| Other | 3 |
| Survey mode – (%) | |
| Self-administered | 85 |
| Interviewer-administered | 15 |
| Education – (%) | |
| Some high school or less | 22 |
| High school graduate or equivalent | 35 |
| Some college of higher | 43 |
| Household income – (%) | |
| ≤$10K | 54 |
| >$10K and ≤$30K | 36 |
| >$30K | 10 |
| Depression screen, positive – (%) | 43 |
| Alcohol screen, positive – (%) | 42 |
| Illegal or Rx drug abuse screen, positive – (%) | 19 |
| Health status – (%) | |
| Poor/fair | 20 |
| Good/very good | 65 |
| Excellent | 15 |
| HIV risk factor – (%) | |
| IVDA | 16 |
| MSM, no IVDA | 33 |
| Heterosexual sex, no IVDA | 50 |
| Transfusion | <1 |
| Currently prescribed HAART – (%) | 94 |
| Duration enrolled in clinic, years – mean (±SD) | 7.6 (±4.5) |
| CD4 counta – median (25th, 75th percentiles) | 449 (276, 665) |
SD indicates standard deviation; IVDA intravenous drug abuse; MSM, men who have sex with men.
Value closest to date of survey completion, ±30 days; CD4 cell count available for 85% of participants.
Structural equation modeling
We used structural equation modeling (SEM) to examine hypothesized relationships between patient satisfaction, retention in HIV care, adherence to HAART, and HIV suppression. SEM is a multivariate statistical method that: 1) inputs empirical data and qualitative causal assumptions from theory-based models, 2) allows for the simultaneous evaluation of direct, indirect and total effects of multiple variables, and 3) accounts for measurement error in the process of modeling relationships between latent variables (i.e. variables that are not directly observed, but estimated from directly measured ones).
Spearman's partial correlation coefficients were calculated for all measures in the structural modeling by controlling for age, race, ethnicity, depression and health status. These computations parcel out the shared variance between each control variable and pair of measures. The resulting partial correlation matrix was used as the input for the structural model estimation (Table 2). Missing data were treated by pairwise deletion. The correlations between clinic sites were comparable.
Table 2. Correlation Matrix.a .
| 1 | 2 | 3 | 4 | 5 | ||
| 1 | Likelihood of recommending clinic | 1.00 | ||||
| 2 | Feelings about care | 0.53** | 1.00 | |||
| 3 | Adherence to HAART | 0.11* | 0.17** | 1.00 | ||
| 4 | Retention in HIV care | 0.17** | 0.08 | 0.12* | 1.00 | |
| 5 | HIV suppression | 0.11* | 0.09 | 0.26** | 0.26** | 1.00 |
Partial correlations controlling for age, race ethnicity, depression, and health status.
p<0.05;
p<0.01.
We first assessed the relationship between retention in HIV care, adherence to HAART and HIV suppression, controlling for age, race, ethnicity, depression and health status. This constituted the baseline model. Next, we included overall patient satisfaction as a predictor latent variable to determine its effect on the relationship between retention, adherence, and, ultimately, HIV suppression. We tested the hypothesized models using SPSS AMOS 19.0 statistical software (SPSS Inc, Chicago, IL).
We performed hypothesis testing by examining parameter estimates. The retention in HIV care and HIV suppression constructs were measured with single indicators. Since HIV RNA copies is the accepted standard measure of HIV suppression, the measurement loading for HIV suppression was set to 1.00 (i.e. no measurement error). Since no studies of reliability have been reported for the retention in HIV care construct and the construct is measured objectively, its measurement error was assumed to be 0 and the measurement loading was set to 1.00. The adherence to HAART construct has an estimated reliability of 0.67 (personal communication, Y. Lee, 2012). This was incorporated into the model by setting the measurement loading to 0.82 (the square root of the reliability 0.67) and the measurement error to 0.33 (1 minus the reliability 0.67).
Model goodness-of-fit was evaluated using 3 widely used indexes: chi-square test (χ2), the Comparative Fit Index (CFI) and Root Mean Square Error of Approximation (RMSEA) [14]. We used conventional cutoff criteria for fit indexes: 1) non-significant χ2 values, 2) CFI values >0.90 [25] or >0.95 [26], and 3) RMSEA values <0.06 [26] or <0.08 [27].
The Institutional Review Board (IRB) for Baylor College of Medicine and Affiliated Institutions approved this study. The IRB waived the need for written informed consent because this research involves no more than minimal risk to the participants. We collected verbal informed consent and documented the procedure. All data were de-identified and analyzed anonymously.
Results
Study population
The study sample includes 489 patients (94% of eligible patients approached; 388 from TSHC and 101 from VAMC). As shown in Table 1, the mean age was 48 years, 71% were men, 61% were non-Hispanic black, and 54% had a household income of ≤$10,000. Participants and eligible non-participants did not differ significantly in terms of age, race, sex, and ethnicity (data not shown).
Overall patient satisfaction
Patients reported high levels of overall satisfaction with HIV care (mean = 8.5, SD = 1.7, median 9.2, range 0.8–10.0). Over 90% would “probably” (23.4%) or “definitely” (69.8%) “recommend this clinic to other patients with HIV,” and over 80% felt “mostly satisfied” (26.7%) or “completely satisfied” (57.3%) with their HIV care.
Retention in HIV care
In the year before enrollment, 76% of participants had adequate retention in HIV care and 24% had inadequate retention. Participants with adequate retention were significantly more satisfied with their HIV care than patients with inadequate retention (median patient satisfaction score 9.17 versus 8.47, respectively; p = 0.02).
Adherence to HAART
A total of 94% were “taking or supposed to be taking HIV medicines.” Among those prescribed HAART, 46%, 28%, 16%, 6%, 2% and 2% reported “excellent,” “very good,” “good,” “fair,” “poor,” and “very poor” adherence, respectively. Participants who reported “excellent” adherence were significantly more satisfied with their HIV care than patients who did not (median patient satisfaction score 10.00 versus 8.61, respectively; p<.0001).
HIV suppression
HIV RNA values at the time of survey completion ±30 days were available for 84% of participants (N = 409). Seventy percent of these patients achieved HIV suppression. Participants who achieved HIV suppression were significantly more satisfied with their HIV care than patients who did not (median patient satisfaction score 9.17 versus 8.47, respectively; p<.01).
Baseline model
The baseline model evaluated the roles of retention in HIV care and adherence to HAART as independent antecedents to HIV suppression (Figure 1). The hypothesized model was a just-identified model with zero degrees of freedom. As such, the model did not allow a test of goodness-of-fit, since technically, all goodness-of-fit indexes in the estimated model have maximum values (χ2 = 0.00, df = 0, p = 0.00, CFI = 1.00, RMSEA = 0.00). However, the model still provides suitable estimates of the hypothesized relationships between latent variables. Table 3 shows the parameter estimates from the baseline model. Retention in HIV care and adherence to HAART were significantly associated with greater HIV suppression (standardized coefficient = .220, p<.0001 and standardized coefficient = .287, p<.0001, respectively).
Figure 1. Baseline Model of Retention in HIV Care, Adherence to HAART and HIV Suppression (N = 489).
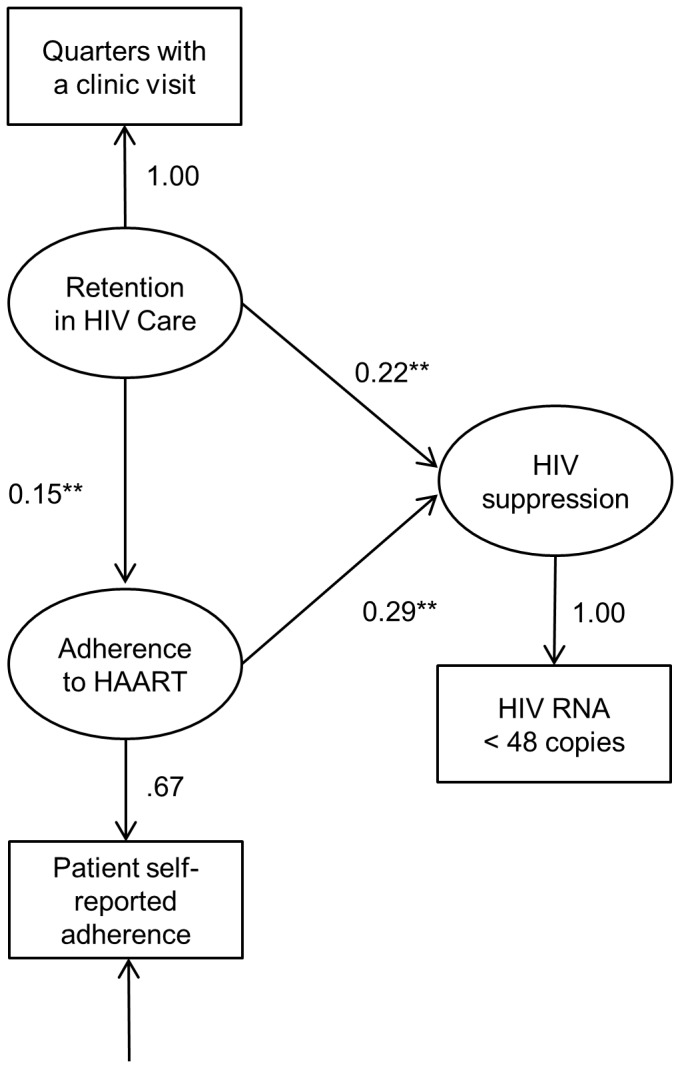
Values indicate standardized coefficients; * p<0.05; ** p<0.001.
Table 3. Parameter Estimates.
| Ba | β | p | |
| Baseline Model b | |||
| Structural Model | |||
| Retention in Care→Adherence to HAART | .147 (.062) | .147 | .02 |
| Retention in Care→HIV Suppression | .220 (.049) | .220 | <.001 |
| Adherence to HAART→HIV Suppression | .287 (.061) | .287 | <.001 |
| Patient Satisfaction Model c | |||
| Measurement Model | |||
| Patient Satisfaction→Feelings about care | 1.000 | .680 | NAd |
| Patient Satisfaction→Recommend Clinic | 1.149 | .778 | <.001 |
| Structural Model | |||
| Patient Satisfaction→Retention in Care | .266 (.094) | .181 | <.001 |
| Patient Satisfaction→Adherence to HAART | .298 (.115) | .203 | <.001 |
| Patient Satisfaction→HIV Suppression | .047 (.089) | .032 | .60 |
| Retention in Care→Adherence to HAART | .110 (.063) | .110 | .08 |
| Retention in Care→HIV Suppression | .215 (.050) | .215 | <.001 |
| Adherence to HAART→HIV Suppression | .280 (.062) | .280 | <.001 |
B denotes B coefficient; β indicates beta coefficient.
Patient Satisfaction properties: composite reliability = 0.70; average variance extracted = 0.54.
Standard errors in parentheses.
Model Goodness of Fit: χ2 = 0.00, df = 0, p = 0.00, CFI = 1.00, RMSEA = 0.00.
Model Goodness of Fit: χ2 = 5.106, df = 2, p = 0.078, CFI = 0.984, RMSEA = 0.064.
NA indicates not applicable. The indicator loading is constrained to 1.0 for latent construct estimation and represents the reference item. No direct test of statistical significance is possible for the constrained indicator.
Model of the effects of patient satisfaction
A second model evaluated the role of overall patient satisfaction in influencing retention in HIV care, adherence to HAART and HIV suppression (Figure 2). The hypothesized model provided a good fit to the data (χ2 = 5.11, df = 2, p = 0.08, CFI = 0.98, RMSEA = 0.06). Table 3 shows the parameter estimates from this hypothesized model of patient satisfaction. The composite reliability and average variance extracted tests for overall patient satisfaction exceeded recommended thresholds (values 0.70 and 0.54, respectively), indicating acceptable construct reliability [11]–[14].
Figure 2. Patient Satisfaction Model (N = 489).

Values indicate standardized coefficients; * p<0.05; ** p<0.001. Estimation requires that one of the indicator loadings of a construct be constrained to 1.0. No direct test of statistical significance is possible for this reference item. Statistical significance is determined by estimating an identical second model, with the indicator constraint of 1.0 moved to a different indicator. Thus, all standardized coefficients can be tested for significance, even though one item must always be constrained in any single estimation.
Similar to the baseline model, the direct effects of retention in HIV care and adherence to HAART on HIV suppression were significant (standardized coefficient = 0.215, p<.0001 and standardized coefficient = 0.280, p<.0001, respectively) (Table 3). The direct effects of patient satisfaction on retention in HIV care and adherence to HAART were also significant (standardized coefficient = 0.181, <.0001 and standardized coefficient = 0.203, p<.0001, respectively). The direct effect of patient satisfaction on HIV suppression was not significant (standardized coefficient = .032, p = .60).
Discussion
In this study of 489 participants receiving outpatient HIV primary care, overall patient satisfaction with care is positively related to retention in HIV care and adherence to HAART, which in turn serve as key determinants of HIV suppression. The data suggest that patient satisfaction may provide a way to improve HIV outcomes through its positive influences on adherence to HAART and retention in HIV care. This finding suggests that patient-centered interventions designed to improve the care experience could serve as an innovative method for optimizing HIV outcomes.
The National Council on Patient Information and Education's report, Enhancing Prescription Medicine Adherence: A National Action Plan, states that medication nonadherence has reached crisis proportions [28]. The report calls for adherence research that explores innovative ways to increase patient uptake of proven therapies. Successful interventions not only need to demonstrate efficacy and effectiveness, but also the capacity for ultimate adoption, implementation and maintenance in real-world settings.
Retention in HIV care is a critical step for achieving long-term survival with HIV infection [29]. Furthermore, HIV primary care guidelines recognize the importance of retention in HIV care as a precursor to adherence to HAART [30]. Successful strategies to improve retention in HIV care and adherence to HAART require an understanding of retention and adherence behavior and the complex interplay between biological, psychological, behavioral, social and health systems drivers. They also require a multi-level, multi-component approach to responding to the needs and concerns of individual patients. Simple practices shown to improve adherence include reductions in dose frequency and the use of adherence aids (e.g. pill boxes, text reminders) [31]–[33]. Successful interventions to improve retention in HIV care have required more complex and intensive efforts to decrease unmet needs, decrease structural barriers and reduce substance abuse [34]. Given the suboptimal state of retention in HIV care and adherence to HAART, it is critical to identify additional modifiable drivers to inform evidence-based interventions to optimize HIV care.
Patient satisfaction represents an innovative focus for retention and adherence intervention efforts. Its innovation derives from applying the business model of customer satisfaction to improve patient adherence to care. Additionally, interventions to improve patient satisfaction with the overall care experience are not directly dependent on efforts to explicitly change patient behavior. Patient satisfaction reflects the patient's perception of the entire care process, and improving satisfaction metrics lies within the power of a clinic or institution.
Research indicates that provider and organizational factors play a large role in how patients evaluate their provider and overall clinic care [8], [35]. Several empirical studies have shown that training in patient-centered communication and audit feedback can help providers improve communication skills in ways that increase patient satisfaction [36], [37]. Furthermore, organizational factors like increasing the time allowed for provider visits and ensuring continuity of care with the same provider can increase patients' satisfaction with their provider and overall care [38]–[40]. Continued progress in studying patient satisfaction requires not only additional evaluation of its effects on health outcomes, but also developing an understanding of the particular mechanisms or processes through which beneficial results are achieved.
The development of successful interventions to improve retention in HIV care and adherence to HAART requires a better understanding of how patient satisfaction impacts those constructs. The exact mechanisms explaining the linkages between these constructs remain unclear. Additionally, it remains unclear which component or components of the care experience most strongly influence retention and adherence. Several studies, including a previous study based on this dataset, have reported that patients' evaluation of their provider correlates the strongest with their overall satisfaction [35], [41], [42]. However, the provider characteristic most predictive of overall patient satisfaction may differ from those that may affect clinical outcomes. For example, provider training in problem solving focused adherence counseling techniques, as proposed in Wilson et al. [43], may have more influence on adherence than providers' interpersonal and general communication skills. Future research directions need to include prospective quantitative studies to: 1) better understand which component or components of the care experience are most predictive of overall patient satisfaction, medication adherence and retention in HIV care, 2) quantify how the strength of association changes over time as care progresses and what factors significantly influence those trends, and 3) establish causal direction.
This study has several methodological strengths. Our practice-based model incorporates the business model of customer satisfaction with the clinical end point of HIV suppression. The study took place at 2 clinic sites. It primarily included a low-income minority population, which often has low rates of adherence to care and worse clinical outcomes [44]. This population would stand to gain the most from interventions to improve adherence to care.
This study has certain limitations. Although our study supports the proposed causal linkages between overall patient satisfaction, retention in HIV care, adherence to HAART, and HIV suppression, correlational data cannot provide definitive evidence of causality. Emerging consensus, however, suggests that such data, when examined through structural equation modeling, can help researchers articulate, clarify and evaluate causal explanations between constructs of interest [45]. Study eligibility required enrollment in clinic for at least one year and thus excluded patients new to HIV clinic. New clinic patients may have greater risk of being lost to follow-up. At the same time, new clinic patients have not formed any behavioral patterns of retention or adherence yet, may be more impressionable [46], and as a result, initial care experiences may have a greater effect on retention and adherence. At present, the relationship between satisfaction and adherence to HIV care in new clinic patients remains unclear. Furthermore, participants received HIV care at the VA and a public clinic, and study findings may not generalize to patients in other settings. Lastly, our model's explanatory power is limited to its included constructs. Our model should be extended in further research by including other predictors of retention in HIV care and adherence to HAART (e.g. patient attributes like adherence self-efficacy and outcome expectations, provider attributes like adherence problem solving counseling skills, etc). The extension of our model to include these and other variables may clarify patient satisfaction's relative contribution to retention and adherence.
Conclusion
This study identified retention in HIV care and adherence to HAART as intervening constructs through which patient satisfaction influences HIV outcomes. Our data raises the intriguing possibility that interventions aimed at improving the patient care experience by improving contextual components of care (i.e. who, where and how care is provided) could affect outcomes without actually targeting objective clinical performance measures. Our findings suggest that patient satisfaction could serve as an innovative target for interventions to improve HIV outcomes.
Acknowledgments
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.
Funding Statement
This material is based upon work supported in part by the Department of Veterans Affairs, Veterans Health Administration, Office of Research and Development, and the Houston VA Health Services Research and Development Center of Excellence (HFP90-020). This material was also supported in part by the facilities and resources of Harris Health System, Houston, Texas. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. No additional external funding was received for this study.
References
- 1. Centers for Disease Control and Prevention (2008) HIV prevalence estimates–United States, 2006. MMWR Morb Mortal Wkly Rep 57 (39) 1073–6. [PubMed] [Google Scholar]
- 2. Marks G, Gardner LI, Craw J, Crepaz N (2010) Entry and retention in medical care among HIV-diagnosed persons: A meta-analysis. AIDS 24 (17) 2665–78. [DOI] [PubMed] [Google Scholar]
- 3. Mills EJ, Nachega JB, Buchan I, Orbinski J, Attaran A, et al. (2006) Adherence to antiretroviral therapy in Sub-Saharan Africa and North America: A meta-analysis. JAMA 296 (6) 679–90. [DOI] [PubMed] [Google Scholar]
- 4. Centers for Disease Control and Prevention (2011) Vital signs: HIV prevention through care and treatment–United States. MMWR Morb Mortal Wkly Rep 60 (47) 1618–23. [PubMed] [Google Scholar]
- 5. Wood E, Hogg RS, Yip B, Harrigan PR, O'Shaughnessy MV, et al. (2004) The impact of adherence on CD4 cell count responses among HIV-infected patients. J Acquir Immune Defic Syndr 35 (3) 261–8. [DOI] [PubMed] [Google Scholar]
- 6. Li JZ, Paredes R, Ribaudo HJ, Svarovskaia ES, Kozal MJ, et al. (2012) Relationship between minority nonnucleoside reverse transcriptase inhibitor resistance mutations, adherence, and the risk of virologic failure. AIDS 26 (2) 185–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mittal V, Frennea C (2010) Customer satisfaction: A strategic review and guidelines for managers. MSI Fast Forward Series, Marketing Science Institute.
- 8. Dang BN, Westbrook RA, Rodriguez-Barradas MC, Giordano TP (2012) Identifying drivers of overall satisfaction in patients receiving HIV primary care: A cross-sectional study. PLoS One 7 (8) e42980. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Andrews FM, Crandall R (1976) The validity of measures of self-reported well-being. Soc Indic Res 3: 1–19. [Google Scholar]
- 10.CAHPS clinician & group survey, adult primary care instrument. CAHPS clinician & group survey and reporting kit. Rockville MD: Agency for Healthcare Research and Quality. Available: https://www.cahps.ahrq.gov/clinician_group. Accessed 2012 Dec 18.
- 11. Fornell C, Larcker DF (1981) Evaluating structural equation models with unobservable variables and measurement error. Journal of Marketing Research 18 (1) 39–50. [Google Scholar]
- 12. Anderson JC, Gerbing DW (1988) Structural equation modeling in practice: A review and recommended two-step approach. Psychological Bulletin 103 (3) 411–423. [Google Scholar]
- 13. Bagozzi RP, Yi Y (1988) On the evaluation of structural equation models. Journal of the Academy of Marketing Science 16 (1) 74–94. [Google Scholar]
- 14.Hair J, Black WC, Babin BJ, Anderson RE (2010) Multivariate data analysis. 7th ed. Englewood Cliffs, NJ: Prentice Hall.
- 15. Lu M, Safren SA, Skolnik PR, Rogers WH, Coady W, et al. (2008) Optimal recall period and response task for self-reported HIV medication adherence. AIDS Behav 12 (1) 86–94. [DOI] [PubMed] [Google Scholar]
- 16. Berg KM, Wilson IB, Li X, Arnsten JH (2012) Comparison of antiretroviral adherence questions. AIDS Behav 16 (2) 461–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services. Available: http://www.aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf. Accessed 2012 Dec 18.
- 18. Mugavero MJ, Davila JA, Nevin CR, Giordano TP (2010) From access to engagement: Measuring retention in outpatient HIV clinical care. AIDS Patient Care STDS 24 (10) 607–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Davies AR, Ware JE (1981) Measuring health perceptions in the health insurance experiment. Santa Monica, CA: Rand Corporation, R-2711-HHS.
- 20. Hennessy CH, Moriarty DG, Zack MM, Scherr PA, Brackbill R (1994) Measuring health-related quality of life for public health surveillance. Public Health Rep 109 (5) 665–72. [PMC free article] [PubMed] [Google Scholar]
- 21. DeSalvo KB, Bloser N, Reynolds K, He J, Muntner P (2006) Mortality prediction with a single general self-rated health question. A meta-analysis. J Gen Intern Med 21 (3) 267–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Watkins CL, Lightbody CE, Sutton CJ, Holcroft L, Jack CI, et al. (2007) Evaluation of a single-item screening tool for depression after stroke: A cohort study. Clin Rehabil 21 (9) 846–52. [DOI] [PubMed] [Google Scholar]
- 23. Smith PC, Schmidt SM, Allensworth-Davies D, Saitz R (2009) Primary care validation of a single-question alcohol screening test. J Gen Intern Med 24 (7) 783–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Smith PC, Schmidt SM, Allensworth-Davies D, Saitz R (2010) A single-question screening test for drug use in primary care. Arch Intern Med 170 (13) 1155–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Netemeyer RG, Bearden WO, Sharma S (2003) Scaling procedures: Issues and applications. Thousand Oaks, CA: Sage Publications, Inc.
- 26. Hu L, Bentler PM (1999) Cutoff criteria for fit indices in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling 6 (1) 1–55. [Google Scholar]
- 27.Browne MW, Cudeck R (1993) Alternative ways of assessing model fit. In: Bollen KA, Long JS. Testing Structural Equation Models. Beverly Hills, CA: Sage. pp. 136–162.
- 28.National Council on Patient Information and Education (2007) Enhancing prescription medicine adherence: A national action plan. Available: http://www.talkaboutrx.org/documents/enhancing_prescription_medicine_adherence.pdf. Accessed 2012 Dec 18.
- 29. Thompson MA, Mugavero MJ, Amico KR, Cargill VA, Chang LW, et al. (2012) Guidelines for improving entry into and retention in care and antiretroviral adherence for persons with HIV: Evidence-based recommendations from an International Association of Physicians in AIDS Care panel. Ann Intern Med 156 (11) 817–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Aberg JA, Kaplan JE, Libman H, Emmanuel P, Anderson JR, et al. (2009) Primary care guidelines for the management of persons infected with human immunodeficiency virus: 2009 update by the HIV Medicine Association of the Infectious Diseases Society of America. Clin Infect Dis 49 (5) 651–81. [DOI] [PubMed] [Google Scholar]
- 31. Simoni JM, Amico KR, Pearson CR, Malow R (2008) Strategies for promoting adherence to antiretroviral therapy: A review of the literature. Curr Infect Dis Rep 10 (6) 515–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Parienti JJ, Bangsberg DR, Verdon R, Gardner EM (2009) Better adherence with once-daily antiretroviral regimens: A meta-analysis. Clin Infect Dis 48 (4) 484–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Pop-Eleches C, Thirumurthy H, Habyarimana JP, Zivin JG, Goldstein MP, et al. (2011) Mobile phone technologies improve adherence to antiretroviral treatment in a resource-limited setting: A randomized controlled trial of text message reminders. AIDS 25 (6) 825–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Rumptz MH, Tobias C, Rajabiun S, Bradford J, Cabral H, et al. (2007) Factors associated with engaging socially marginalized HIV-positive persons in primary care. AIDS Patient Care STDS 21 Suppl 1: S30–9. [DOI] [PubMed] [Google Scholar]
- 35. Crow R, Gage H, Hampson S, Hart J, Kimber A, et al. (2002) The measurement of satisfaction with healthcare: Implications for practice from a systematic review of the literature. Health Technol Assess 6 (32) 1–244. [DOI] [PubMed] [Google Scholar]
- 36. Cope DW, Linn LS, Leake BD, Barrett PA (1986) Modification of residents' behavior by preceptor feedback of patient satisfaction. J Gen Intern Med 1 (6) 394–8. [DOI] [PubMed] [Google Scholar]
- 37. Yedidia MJ, Gillespie CC, Kachur E, Schwartz MD, Ockene J, et al. (2003) Effect of communications training on medical student performance. JAMA 290 (9) 1157–65. [DOI] [PubMed] [Google Scholar]
- 38. Morrell DC, Evans ME, Morris RW, Roland MO (1986) The “five minute” consultation: Effect of time constraint on clinical content and patient satisfaction. Br Med J (Clin Res Ed) 292 (6524) 870–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Baker R (1996) Characteristics of practices, general practitioners and patients related to levels of patients' satisfaction with consultations. Br J Gen Pract 46 (411) 601–5. [PMC free article] [PubMed] [Google Scholar]
- 40. Fan VS, Burman M, McDonell MB, Fihn SD (2005) Continuity of care and other determinants of patient satisfaction with primary care. J Gen Intern Med 20 (3) 226–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Kane RL (2005) Satisfaction with care. In: Understanding Health Care Outcomes Research. Sudbury, MA: Jones & Bartlett Pub. 185 p.
- 42. Sitzia J, Wood N (1997) Patient satisfaction: A review of issues and concepts. Soc Sci Med 45 (12) 1829–43. [DOI] [PubMed] [Google Scholar]
- 43. Wilson IB, Laws MB, Safren SA, Lee Y, Lu M, et al. (2010) Provider-focused intervention increases adherence-related dialogue but does not improve antiretroviral therapy adherence in persons with HIV. J Acquir Immune Defic Syndr 53 (3) 338–47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Giordano TP, Bartsch G, Zhang Y, Tedaldi E, Absalon J, et al. (2010) Disparities in outcomes for African American and Latino subjects in the flexible initial retrovirus suppressive therapies (FIRST) trial. AIDS Patient Care STDS 24 (5) 287–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Markus KA (2010) Structural equations and causal explanations: Some challenges for causal SEM. Structural Equation Modeling: A Multidisciplinary Journal 17 (4) 654–676. [Google Scholar]
- 46. Gardner LI, Marks G, Craw JA, Wilson TE, Drainoni ML, et al. (2012) A low-effort, clinic-wide intervention improves attendance for HIV primary care. Clin Infect Dis 55 (8) 1124–34. [DOI] [PMC free article] [PubMed] [Google Scholar]