

Summary
Background
Hyperlipidemia is an identified factor of premature vessel atherosclerosis. Lipemia retinalis is an unusual retinal manifestation of hyperlipidemia and is thought to be directly correlated with the serum triglyceride level.
Case Report
This paper discusses the case of a 55-year-old patient with lipemia retinalis, which deteriorated his visual acuity. The patient had an extremely high serum cholesterol level (1053 mg/dl) and a very high level of triglycerides (1513 mg/dl). The normalization of serum lipids, reversion of retinal vessels alterations and visual acuity improvement was achieved after an intensive statin lipid-lowering therapy. Pathological changes of the patient’s retina, connected with lipemia retinalis, disappeared completely.
Conclusions
Hyperlipidemia can cause lipemia retinalis, which is characterized by the hyperlipidemic vascular lesions-whitish color of vessels, lipid infiltration into the retina and decrease of visual acuity. The lipid-lowering therapy may lead to the normalization of the appearance of the fundus and restore the visual acuity.
Keywords: hyperlipidemia, atherosclerosis, lipemia retinalis
Background
Hyperlipidemias manifest themselves mainly by increased blood serum concentrations of cholesterol or triglycerides and the disturbances in LDL or/and HDL cholesterol. The consequences of hyperlipidemia are multiorgan and include premature atherosclerosis with all its effects, lesions of the digestive system (liver and pancreas), skin and sometimes ocular changes [1]. Lipemia retinalis is a rare retinal manifestation of hypertriglyceridemia [2–4]. It was first described by Heyl in 1880 [5]. Retinal vessels become cream colored due to the scattering of light by the triglyceride-laden chylomicrons. Very high levels of triglycerides are required; hypercholesterolemia alone does not produce this vascular appearance [2]. In clinical practice, elevated serum triglycerides are most often observed in persons with metabolic syndrome, despite the fact that secondary or genetic factors can heighten triglyceride levels [6].
Case Report
We report the case of a 55-year-old patient treated for age-related macular degeneration who had exudative form in the right eye and non-exudative in the left eye for 2 years, and presented a deterioration of vision in his left eye. For this reason, preparations containing antioxidants, vitamins and minerals (Zinc) were prescribed. However, it is not certain that he used them systematically. He had also a history of lipid disorder (high serum cholesterol and dyslipidemia in anamnesis). The visual acuity in his right eye was counting fingers at 2 m and acuity in his left eye decreased from 0.7 to 0.5. Eye fundus examination revealed lipemia retinalis; the hyperlipidemic vascular lesions had whitish-colored vessels and lipid infiltration into the retina and age-related macular degeneration in both eyes. (Figures 1, 2).
Figure 1.
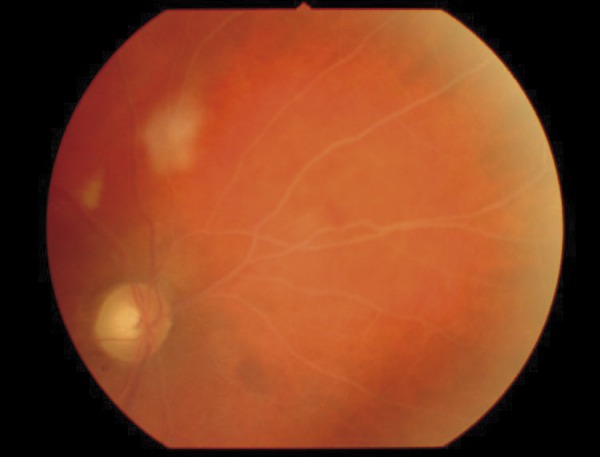
The right eye fundus with signs of lipemia retinalis (optic disc and nasal part of retina). Characteristic whitish vessels are visible. It is difficult to distinguish the arteries from the veins.
Figure 2.

The left eye fundus with signs of lipemia retinalis (optic disc and a part of macula). Characteristic whitish vessels are visible. It is difficult to distinguish the arteries from the veins.
We found an extremely high serum cholesterol level (1053 mg/dl [normal desirable <200 mg/dl, borderline high 200–239 mg/dl, high ≥240 mg/dl]), very high level of triglycerides (1513 mg/dl [normal <200 mg/dl]) and dyslipidemia characterized by very high LDL cholesterol level (722 mg/dl [normal range 60–130 mg/dl]) and low concentration of HDL cholesterol (29 mg/dl [normal >40 mg/dl]). Additionally, a higher activity of aminotransferases was observed – Aspat (169 U/L [normal <34U/L]) and Alat (89 U/l [normal <31 U/L]). Subsequently, considering the lipid disturbances, the patient was referred to the Department of Internal Medicine to perform further diagnosis and treatment. During hospitalization, the medical diagnosis was made on the basis of medical history, medical examination and diagnostic investigations. The patient suffered from coronary disease, hypertension, hyperlipidemia, hepatic lesion and alcoholic dependence. The normalization of serum lipids and reversion of retinal vessels alterations was achieved after an intensive statin lipid-lowering therapy (atorvastatin 40 mg daily for 8 weeks) (Figures 3, 4).
Figure 3.

The right eye fundus after treatment. The retinal vessels abnormalities returned to normal. Nevertheless, the age-related macular degenerations remained (a big scar in the macula).
Figure 4.

The left eye fundus after treatment. The retinal vessels abnormalities returned to normal. Nevertheless, the age-related macular degenerations remained (retinal pigment defects, drusen).
After the treatment, the visual acuity of right eye did not change, but the left eye improved to 0.7. It was impossible to achieve significant improvement of visual acuity in the right eye because of the severe form of macular degenerations.
Discussion
Primary and secondary hyperlipidemias are identified factors of premature vessel atherosclerosis. Endothelial damage in atherosclerosis is characterized by abnormal vascular functionality [7–9]. Despite the fact that alterations in the cardio-vascular system, skin changes and digestive symptoms are well known and expected, the ocular lesions in hyperlipidemia are often forgotten. However, there are reports describing the ocular lesions in hyperlipoproteinemia, such as xanthelasma (a deposition of lipid the in eyelid), lipid keratopathy (corneal arcus), retinal artery and vein occlusions, ischemic optic neuropathy, cataract and even dry eye [2,10,11].
The Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on the Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) defines lipemia retinalis as one of the outcomes of hypertriglyceridemia [5]. According the NCEP, optimal serum LDL cholesterol level should be below 100 mg/dL (LDL above 190 mg/dl is classified as very high) [6]. As it is a rare entity, we found it interesting to present the case, in which the markedly elevated serum concentrations of triglycerides, total cholesterol and LDL cholesterol altered the retinal vessels as lipid infiltrated the small vessels’ walls. According to Nagra et al., lipemia retinalis is thought to be directly correlated with the serum triglyceride level. Typically, the retinal findings do not occur until the triglyceride level reaches 2500 mg per deciliter. The findings can fluctuate widely from day to day, depending on the triglyceride level [2]. Hypercholesterolemia alone does not produce retinal changes [12]. Patients with lipemia retinalis in typical cases maintain good vision, and fundus changes resolve when serum lipid levels are reduced [2,13]. However, it was shown in a rabbit model of hypercholesterolemia that normalization of serum cholesterol levels was not enough to reverse cholesterol-induced vascular damage to the choroid and retinal vessels. These vascular changes could be compatible with a chronic ischemia that could produce retinal degeneration [7,14]. It is interesting that in the described patient, lipemia retinalis was observed at concentrations of triglycerides below 2500 mg per deciliter. We believe that in the presented case an extremely high serum cholesterol level and dyslipidemia could contribute to the vascular changes. In the case of our patient, hyperlipidemia was secondary to a lipid-rich diet, excessive use of alcohol and lack of physical activity. It should be stressed that a lipid disorder resulting in lipemia retinalis causes a risk of life-threatening atherosclerotic disease [4,8,9] and other severe complications like acute pancreatitis [15]. Moreover, characteristic retinal findings may be the only sign of lipid disturbances (which are often asymptomatic). In such patients a multidisciplinary approach is necessary to obtain the desirable systemic outcome [4,15].
After 2 months of lipid-lowering therapy, the serum cholesterol and triglyceride levels returned to normal. Pathological changes in the patient’s retina, connected with lipemia retinalis, disappeared completely; however, the macular lesions remained. Such intensity of age-related macular degeneration at a relatively young age could be caused by irreversible, microscopic damage to choroid and retina. Lipid-lowering treatment of lipemia retinalis with statin and improvement in vision has not been reported thus far in the medical literature.
Conclusions
Hyperlipidemia can cause retinal alterations called ‘lipemia retinalis’, which is characterized by hyperlipidemic vascular lesions with whitish-colored vessels, lipid infiltration into the retina and decreased visual acuity.
Lipid-lowering therapy may lead to the normalization of the fundus appearance and restoration of visual acuity.
Ophthalmologists should refer patients with lipemia retinalis to lipid disorder specialists.
Footnotes
Disclosure
The authors have no financial or other relationships that might lead to a conflict of interest.
Source of support: This study was supported by grant No 507/11 from the Medical University of Lublin
References
- 1.Leaf DA. Chylomicronemia and the chylomicronemia syndrome: a practical approach to management. Am J Med. 2008;121:10–12. doi: 10.1016/j.amjmed.2007.10.004. [DOI] [PubMed] [Google Scholar]
- 2.Nagra PK, Ho AC, Dugan JD. Lipemia retinalis associated with branch retinal vein occlusion. Am J Ophthalmol. 2003;135:539–42. doi: 10.1016/s0002-9394(02)02076-7. [DOI] [PubMed] [Google Scholar]
- 3.Park YH, Lee YC. Images in clinical medicine. Lipemia retinalis associated with secondary hyperlipidemia. N Engl J Med. 2007;357(10):e11. doi: 10.1056/NEJMicm065167. [DOI] [PubMed] [Google Scholar]
- 4.Nogales SL, Grimes AL, Song HF. Lipemia retinalis: A combination of genetics and the American diet and lifestyle. Optometry. 2011 Nov 2; doi: 10.1016/j.optm.2011.05.008. [DOI] [PubMed] [Google Scholar]
- 5.Heyl AG. Intraocular lipemia. Trans Am Ophthalmol Soc. 1880;3:55. [PMC free article] [PubMed] [Google Scholar]
- 6.Expert Panel on Detection Evaluation and Treatment of High Blood Cholesterol in Adults: Executive Summary of the Third Report pf the National Cholesterol Education Program (NCEP) JAMA. 2001;285:2486–97. doi: 10.1001/jama.285.19.2486. [DOI] [PubMed] [Google Scholar]
- 7.Salazar JJ, Ramírez AI, de Hoz R, et al. Alterations in the choroids in hypercholesterolemic rabbits: reversibility after normalization of cholesterol levels. Exp Eye Res. 2007;84(3):412–22. doi: 10.1016/j.exer.2006.10.012. [DOI] [PubMed] [Google Scholar]
- 8.Rafael H. Cerebral atherosclerosis causes neurodegenerative diseases. Med Sci Monit. 2010;16(1):LE1–2. [PubMed] [Google Scholar]
- 9.Giaginis C, Klonaris C, Katsargyris A, et al. Correlation of Peroxisome Proliferator-Activated Receptor-gamma (PPAR-gamma) and Retinoid X Receptor-alpha (RXR-alpha) expression with clinical risk factors in patients with advanced carotid atherosclerosis. Med Sci Monit. 2011;17(7):CR381–91. doi: 10.12659/MSM.881849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rowe S, MacLean CH, Shekelle PG. Preventing visual loss from chronic eye disease in primary care: scientific review. JAMA. 2004;291:1487–95. doi: 10.1001/jama.291.12.1487. [DOI] [PubMed] [Google Scholar]
- 11.Kumar J, Wierzbicki AS. Images in clinical medicine. Lipemia retinalis N Engl J Med. 2005;353(8):823. doi: 10.1056/NEJMicm040437. [DOI] [PubMed] [Google Scholar]
- 12.Vinger PF, Sachs BA. Ocular manifestations of hyperlipoproteinemia. Am J Opthalmol. 1970;70:563–72. doi: 10.1016/0002-9394(70)90890-1. [DOI] [PubMed] [Google Scholar]
- 13.Ram J, Pandav SS, Jain S, et al. Reversal of lipemia retinalis with dietary control. Eye. 1993;7:763–65. doi: 10.1038/eye.1993.178. [DOI] [PubMed] [Google Scholar]
- 14.Ramírez AI, Salazar JJ, de Hoz R, et al. Macroglial and retinal changes in hypercholesterolemic rabbits after normalization of cholesterol levels. Exp Eye Res. 2006;83:1423–38. doi: 10.1016/j.exer.2006.07.023. [DOI] [PubMed] [Google Scholar]
- 15.Horton M, Thompson K. Lipemia retinalis preceding acute pancreatitis. Optometry. 2011;82(8):475–80. doi: 10.1016/j.optm.2011.01.011. [DOI] [PubMed] [Google Scholar]