

Summary
Background
Multiple carcinoid tumors of the small intestine are rare and are very difficult to detect preoperatively.
Case Report
A 75-year-old woman in whom the bleeding focus could not be found by upper and lower endoscopy and abdominal CT was admitted for evaluation of anemia. We examined the patient with total double-balloon endoscopy (DBE) and located multiple submucosal tumors. The multiple carcinoid tumors were resected successfully under laparoscopy.
Conclusions
We report a case of a successful laparoscopic operation for multiple carcinoid tumors in the small intestine without intraoperative endoscopy. Total digestive tract observation using DBE is very useful for laparoscopic operation for multiple tumors in the small intestine.
Keywords: double balloon endoscopy, carcinoid tumor, small intestine, capsule endoscopy
Background
Tumors of the small intestine account for 1% to 2% of all gastrointestinal neoplasms (only 0.3% of all neoplasms) [1]. However, the incidence of small intestine cancer has increased dramatically over the past 30 years [2], and the increase in carcinoid tumors has been largely responsible. Carcinoids of the ileum account for 15.4% of all gastrointestinal carcinoids [3] and are multicentric in 20–30% of patients [4]. The lack of signs and symptoms, lack of definitive preoperative diagnostic tests, and the variable efficacy of available tests make small intestine tumors difficult to diagnose [5]. The recent development of capsule endoscopy (CE) and double balloon endoscopy (DBE) has improved diagnostic capabilities for the small intestine. We report the first case of multiple carcinoid tumors of the small intestine preoperatively diagnosed by DBE and treated with laparoscopic surgery.
Case Report
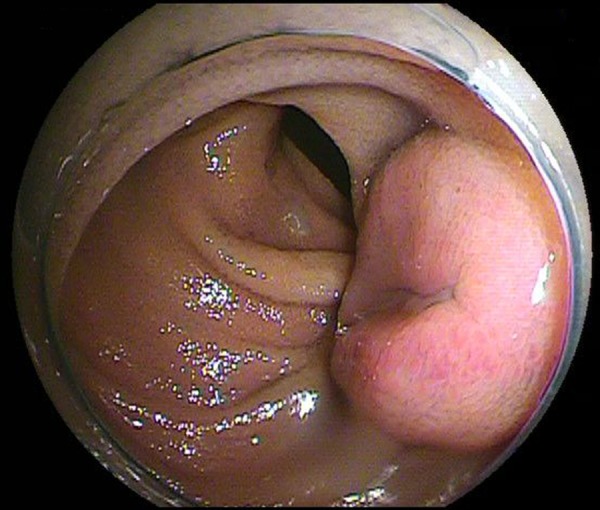
A 75-year-old woman was referred to our hospital with melena and severe anemia (hemoglobin (Hb) 7.2 g/dL). She had a history of stroke at age 59 years, and was being treated with antiplatelet therapy at the time of admission to the referring hospital. At that hospital, the source of GI bleeding was not revealed by upper and lower gastrointestinal endoscopy examination, abdominal computed tomography (CT), or ultrasound (US). Through radiological enteroclysis, an elevated lesion was found in the ileum, which was suspected to be a submucosal tumor and measured 15 mm in diameter. Melena had resolved after stopping low-dose aspirin. Anemia was also improved by administration of an iron preparation without a blood transfusion. After 2 months at the referring hospital, she was admitted to our hospital for a thorough investigation of the small intestine. Physical examination revealed her abdomen to be soft and flat without any pain or tenderness. Results of blood tests were as follows: Hb 11.3 g/dL (normal: 11.1–15.2 g/dL), red blood cell count 418 104/mL (normal: 380–540 104/mL), and hematocrit 35.3% (normal: 35.6–45.4%). The remaining results were also normal. No findings were noted on abdominal X-ray. We then examined the patient with peroral DBE (EN-450P5: FUJIFILM Medical Co., Ltd., Tokyo, Japan). A tumor was located about 250 cm from the ligament of Treitz and measured 8 mm in diameter (Figure 1). The tumor was yellowish in color and covered with mucosa of normal appearance. However, active bleeding was not observed during the procedure. Histologic examination of the biopsy sample obtained by endoscopy confirmed the diagnosis of a carcinoid tumor. The tumor was composed of small uniform epithelial cells, which stained positively for chromogranin A and synaptophysin.
Figure 1.

Double balloon endoscopy showed a submucosal tumor of the ileum.
Another tumor detected through peranal DBE was located about 110 cm from the ileocecal valve and measured 15 mm in diameter. Also, other small tumors were detected that measured 3 mm and 5 mm in diameter and had a relatively smooth surface, similar to a submucosal tumor. These small tumors were diagnosed as carcinoid tumors by endoscopic findings, whereas histologic examination could not make this diagnosis. The largest tumor had ulcerations, which could account for the GI bleeding (Figure 2). However, active bleeding was not observed from the ulcer during the procedure. Thus, endoscopic treatment was not required. The patient underwent partial resection of the small intestine by laparoscopic surgery (resected portion: 23.8 cm). She had already undergone a preoperative total small intestinal examination using DBE; therefore, it was not necessary to perform intraoperative endoscopy. The resected specimen contained tumors measuring 14×10 mm, with central ulceration (Figure 3), 2.8×6 mm and a tumor 3 mm in diameter. Microscopically, the tumors were composed of small uniform epithelial cells (Figure 4B), which stained positively for chromogranin A and synaptophysin (Figure 5). Furthermore, the largest tumor had invaded the muscularis propria (Figure 4A). MIB-1 index was less than 1%. No metastases were found in the regional lymph nodes, and the surgical margins were negative for tumor cells. After the surgery, the patient had no gastrointestinal bleeding. Follow-up DBE was performed 18 months later, and there was no sign of recurrence in the small intestine.
Figure 2.
The largest tumor had ulcerations as shown by double balloon endoscopy.
Figure 3.
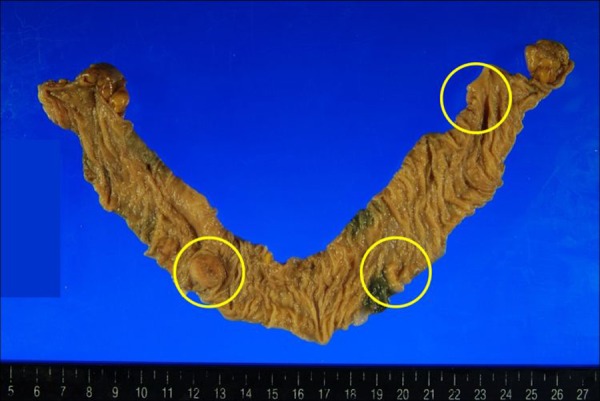
Macroscopically, the resected specimen appears as a flat and slightly depressed polypoid lesion measuring 14×10 mm, with central ulceration and another tumor 3 mm in diameter.
Figure 4.
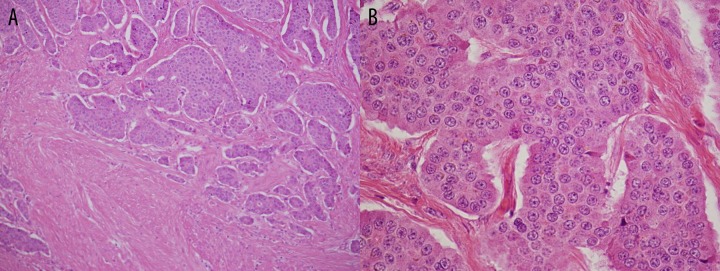
(A) Carcinoid tumors with different degrees of cellularity of various sized solid nests of tumor cells. The islands are relatively closely packed and a marked tissue retraction artifact is present. Carcinoid tumors invaded the muscularis propria. (B) Higher magnification of the lesion shown in solid nests as well as glandular structures. Some cells have large nuclei and small nucleoli as well as inconspicusous cytoplasm and fine chromatin (Haematoxilin-eosin staining).
Figure 5.
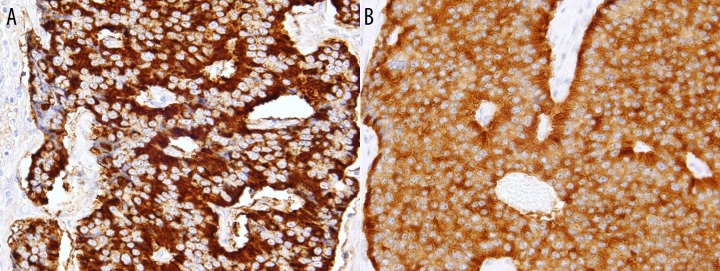
Small uniform epithelial cells stained positively for chromogranin A and synaptophysin. (A) Chromogranin immunostain demonstrating the strong immunoreactivity of the tumor cells. The majority of neuroendocrine granules cluster at the base of the cells giving a prominent peripheral staining pattern. (B) Synaptophysin immunostain demonstrating the neuroendocrine nature of the tumor.
Discussion
This is the first report of laparoscopic surgery without the use of intraoperative endoscopy for multiple carcinoid tumors of the small intestine, which was possible because the tumors were diagnosed before surgery by DBE.
Carcinoid is the second most common malignancy, accounting for approximately 20–25% of all small intestine lesions [6]. Carcinoid tumors are more common in the ileum (most within 60 cm of the ileocecal valve) than in the jejunum or duodenum, and lesions may be multiple and/or metastatic (liver and lungs) at the time of diagnosis because one fourth of carcinoid tumors in the small intestine are multiple [7]. On the guideline, by far the majority of small intestinal neuroendocrine tumors (NETs, including carcinoid) are malignant in nature. Whether liver metastases are present or not, resection of the primary tumor is appropriate to cure or to delay progression that would otherwise endanger the small bowel [8].
It is difficult and rare to preoperatively diagnose carcinoid tumors in the small intestine [5]. Carcinoids of the rectum, stomach, and duodenum generally are found by endoscopy at an early stage, whereas carcinoid tumors of the small intestine usually are discovered after resection of the small intestine for symptoms of obstruction or during exploration of the small intestine in search of a primary tumor after distant metastases have been found [2,9–12]. Through conventional imaging techniques (e.g., CT, US, double contrast barium study), few tumors of a small diameter are identified.
Currently, with advancement in methods of CE, small intestine tumors can be located. CE had a high diagnostic yield of 45% for identification of primary small intestinal carcinoid tumors [13]. CE is a simple, safe and comfortable diagnostic technique [14]. However, it remains purely a diagnostic procedure at present because it is not suitable for histological diagnosis and procedures. For this reason, if laparoscopic surgery is performed in a patient who was diagnosed as having multiple carcinoid tumors of the small intestine, it is usually necessary to perform intraoperative endoscopy to confirm that the lesion is a carcinoid tumor. It is notable that in reporting the results of their study, M. Bellutti et al. suggested that intraoperative endoscopy is a potential gold standard for NETs [15].
On the other hand, DBE can detect these lesions and perform therapeutic procedures and diagnostic interventions [16]. A submucosal tumor of the ileum or the jejunum was detected by DBE in 7 of 12 patients (58%) with suspected carcinoid syndrome [15]. In addition, tumor marking using injection of ink for the exact location during DBE has been helpful for subsequent operations, especially for laparoscopic resection. By utilizing DBE, we were able to locate the multiple ileal tumors and to perform laparoscopic surgery without intraoperative endoscopy in the patient reported here.
DBE is a safe procedure, with low complication rates even when therapeutic maneuvers are performed [17]. As only DBE allows direct, controlled visualization of small intestine tumors and their histological confirmation preoperatively, it may be considered the gold standard for the diagnosis of such tumors [18]. DBE is extremely useful to detect and diagnose asymptomatic small lesions in the small intestine.
Conclusions
Based on the case presented here, we recommend total digestive tract observation using DBE before performing laparoscopic operation for multiple tumors of the small intestine.
Footnotes
Statement
The authors declare no conflicts of interest.
Source of support: No funding support
References
- 1.Ugurlu MM, Asoglu O, Potter DD, et al. Adenocarcinomas of the jejunum and ileum: a 25-year experience. J Gastrointest Surg. 2005;9:1182–88. doi: 10.1016/j.gassur.2005.08.027. [DOI] [PubMed] [Google Scholar]
- 2.Bilimoria KY, Bentrem DJ, Wayne JD, et al. Small Bowel Cancer in the United States. Ann Surg. 2009;249:63–71. doi: 10.1097/SLA.0b013e31818e4641. [DOI] [PubMed] [Google Scholar]
- 3.Memon MA, Nelson H. Gastrointestinal carcinoid tumors. Dis Colon Rectum. 1997;40:1101–13. doi: 10.1007/BF02050937. [DOI] [PubMed] [Google Scholar]
- 4.Yamaguchi T, Manabe N, Tanaka S, et al. Multiple carcinoid tumors of the ileum preoperatively diagnosed by enteroscopy with the double-balloon technique. Gastrointest Endosc. 2005;62:315–18. doi: 10.1016/s0016-5107(05)01569-5. [DOI] [PubMed] [Google Scholar]
- 5.Zouhairi ME, Venner A, Charabaty A, et al. Small bowel adenocarcinoma. Curr Treat Options Oncol. 2008;9:388–99. doi: 10.1007/s11864-009-0098-0. [DOI] [PubMed] [Google Scholar]
- 6.Marshall JB, Bodnarchuk G. Carcinoid tumors of the gut. Our experience over three decades and review of the literature. J Clin Gastroenterol. 1993;16:123–29. [PubMed] [Google Scholar]
- 7.Anzidei M, Napoli A, Zini C, et al. Malignant tumors of the small intestine. Br J Radiol. 2011;84:677–90. doi: 10.1259/bjr/20673379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ramage JK, Ahmed A, Ardill J, et al. Guidelines for the management of gastroenteropancreatic neuroendocrine tumours. Gut. 2012;61:6–32. doi: 10.1136/gutjnl-2011-300831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gill SS, Heuman DM, Mihas AA. Small intestinal neoplasms. J Clin Gastroenterol. 2001;33:267–82. doi: 10.1097/00004836-200110000-00004. [DOI] [PubMed] [Google Scholar]
- 10.Kulke MH, Mayer RJ. Carcinoid tumors. N Engl J Med. 1999;340:858–68. doi: 10.1056/NEJM199903183401107. [DOI] [PubMed] [Google Scholar]
- 11.Burke AP, Thomas RM, Elsayed AM, et al. Carcinoids of the jejunum and ileum. Cancer. 1997;79:1086–93. [PubMed] [Google Scholar]
- 12.Bilimoria K, Bentrem D, Wayne J, et al. Small bowel cancer in the United States. Ann Surg. 2009;249:63–71. doi: 10.1097/SLA.0b013e31818e4641. [DOI] [PubMed] [Google Scholar]
- 13.van Tuyl SA, van Noorden JT, Timmer R, et al. Detection of small-bowel neuroendocrine tumors by video capsule endoscopy. Gastrointest Endosc. 2006;64:66–72. doi: 10.1016/j.gie.2006.01.054. [DOI] [PubMed] [Google Scholar]
- 14.Harrison’s Principles of Internal Medicine. 17th ed. McGraw-Hill; 2008. [Google Scholar]
- 15.Bellutti M, Fry LC, Schmitt J, et al. Detection of neuroendocrine tumors of the small bowel by double balloon enteroscopy. Dig Dis Sci. 2009;54:1050–58. doi: 10.1007/s10620-008-0456-y. [DOI] [PubMed] [Google Scholar]
- 16.Adi L, Moshe N, Carlos S. Double balloon enteroscopy: a 2 year experience. IMAJ. 2009;11:456–59. [PubMed] [Google Scholar]
- 17.Mensink PB, Garingsma J, Kucharzik T, et al. Complications of double balloon enteroscopy: a multicenter survey. Endoscopy. 2007;39:613–15. doi: 10.1055/s-2007-966444. [DOI] [PubMed] [Google Scholar]
- 18.Lee HJ, Cha JM, Lee JI, et al. A case of jejunal adenocarcinoma diagnosied by preoperative double balloon enteroscopy. Gut and Liver. 2009;3:311–14. doi: 10.5009/gnl.2009.3.4.311. [DOI] [PMC free article] [PubMed] [Google Scholar]