

Abstract
In Europe, the combination of plerixafor + granulocyte colony-stimulating factor is approved for the mobilization of hematopoietic stem cells for autologous transplantation in patients with lymphoma and myeloma whose cells mobilize poorly. The purpose of this study was to further assess the safety and efficacy of plerixafor + granulocyte colony-stimulating factor for front-line mobilization in European patients with lymphoma or myeloma. In this multicenter, open label, single-arm study, patients received granulocyte colony-stimulating factor (10 μg/kg/day) subcutaneously for 4 days; on the evening of day 4 they were given plerixafor (0.24 mg/kg) subcutaneously. Patients underwent apheresis on day 5 after a morning dose of granulocyte colony-stimulating factor. The primary study objective was to confirm the safety of mobilization with plerixafor. Secondary objectives included assessment of efficacy (apheresis yield, time to engraftment). The combination of plerixafor + granulocyte colony-stimulating factor was used to mobilize hematopoietic stem cells in 118 patients (90 with myeloma, 25 with non-Hodgkin's lymphoma, 3 with Hodgkin's disease). Treatment-emergent plerixafor-related adverse events were reported in 24 patients. Most adverse events occurred within 1 hour after injection, were grade 1 or 2 in severity and included gastrointestinal disorders or injection-site reactions. The minimum cell yield (≥2×106 CD34+ cells/kg) was harvested in 98% of patients with myeloma and in 80% of those with non-Hodgkin's lymphoma in a median of one apheresis. The optimum cell dose (≥5×106 CD34+ cells/kg for non-Hodgkin's lymphoma or ≥6×106 CD34+ cells/kg for myeloma) was harvested in 89% of myeloma patients and 48% of non-Hodgkin's lymphoma patients. In this prospective, multicenter European study, mobilization with plerixafor + granulocyte colony-stimulating factor allowed the majority of patients with myeloma or non-Hodgkin's lymphoma to undergo transplantation with minimal toxicity, providing further data supporting the safety and efficacy of plerixafor + granulocyte colony-stimulating factor for front-line mobilization of hematopoietic stem cells in patients with non-Hodgkin's lymphoma or myeloma.
Introduction
High-dose chemotherapy followed by autologous hematopoietic stem cell transplantation of peripheral blood stem cells remains a standard of care for patients with relapsed or treatment-refractory high-grade non-Hodgkin's lymphoma (NHL), Hodgkin's disease (HD), or multiple myeloma (MM) with a large tumor mass.1-4 The correlation between successful engraftment and the number of CD34+ cells infused has been well established, making it important to optimize the number of peripheral blood stem cells collected during apheresis.5 The target number of CD34+ cells utilized for a single autologous hematopoietic stem cell transplant may vary between sites, but it has been suggested to be ≥5×106 CD34+ cells/kg recipient body weight with 2×106 CD34+ cells/kg being the minimum number required to guarantee successful engraftment.6,7 The number of circulating hematopoietic stem cells increases during the recovery phase of chemotherapy-induced myelosuppression, as well as after the administration of various cytokines and hematopoietic growth factors including granulocyte colony-stimulating factor (G-CSF).2,8,9 Over the last two decades, clinical practices have taken advantage of these observations. However, increasing awareness of mobilization failure with G-CSF alone or with chemotherapy, and the potential for toxicities and infection with chemotherapy-based mobilization highlighted the need to develop novel mobilization agents.6,10
Plerixafor is a novel bicyclam small-molecule that reversibly binds to chemokine receptor CXCR4 and antagonizes the chemokine stromal cell-derived factor-1α (SDF-1α) interaction.173 Plerixafor is approved by the Food and Drug Administration in combination with G-CSF to mobilize hematopoietic stem cells to the peripheral blood for collection and subsequent autologous transplantation in patients with NHL and MM.12,13 Comparatively, the approved indication for plerixafor in Europe is in combination with G-CSF for mobilization of hematopoietic stem cells for autologous transplantation in patients with lymphoma and MM whose cells mobilize poorly.14
Two phase III, multicenter, double blind, placebo-controlled, randomized clinical studies were conducted in the USA to evaluate the safety and efficacy of plerixafor 0.24 mg/kg plus G-CSF versus placebo plus G-CSF when used to mobilize CD34+ stem cells. The two studies enrolled patients with NHL and MM who had not previously had unsuccessful stem cell collections nor received prior stem cell transplants. In both studies, the combination of plerixafor plus G-CSF was safe and well tolerated and the efficacy results demonstrated that plerixafor plus G-CSF mobilized significantly higher numbers of hematopoietic stem cells and allowed collection of higher numbers of stem cells in fewer days of apheresis compared to G-CSF alone.12,13 The vast majority of sites for both studies were located in the USA, with the exception of one center in Germany which enrolled ten patients with MM. Prior to carrying out this study, there was a paucity of data about the use of plerixafor as a first-line mobilization agent in the European Union, where clinical practices and patients' characteristics are different from those in the USA. The purpose of this multicenter, open label, single-arm study was to further investigate the safety and efficacy of plerixafor plus G-CSF for first-line mobilization in European patients with lymphoma or multiple myeloma.
Design and Methods
Study design and patients
This was a multicenter, open label, single-arm study that evaluated the safety and efficacy of plerixafor in patients with NHL, HD, or MM. The study was divided into three time periods: period 1 (mobilization and apheresis): from the first G-CSF dose up to 30 days after the last plerixafor dose or until the first dose of chemotherapy (whichever was earlier); period 2 (high-dose ablative chemotherapy and transplantation): first day of high-dose chemotherapy to first day of engraftment; and period 3 (posttransplantation): engraftment to the 12-month follow-up.
This study was conducted in accordance with the International Conference on Harmonization, Good Clinical Practice guidelines, the European Union Clinical Trial Directive, and the principles defined in the Declaration of Helsinki and its amendments. The study was approved by the ethics committee of each participating site and registered at clinicaltrials.gov under identification number NCT 00838357. All patients provided written informed consent.
Eligibility and exclusion criteria
Patients aged ≥18 years with a confirmed diagnosis of MM, NHL, or HD in partial or complete remission, eligible for autologous hematopoietic stem cell transplantation and with an Eastern Cooperative Oncology Group performance status of 0 to 1 were eligible to participate. Additional key inclusion criteria included a white blood cell count ≥2.5×109/L, absolute neutrophil count ≥1.5×109/L, platelet count ≥100×109/L, serum creatinine ≤2.2 mg/dL, liver function tests less than 2.5 times the upper limit of normal, and adequate renal, cardiac and pulmonary function sufficient to undergo apheresis.
Patients were excluded if they: had a history of any acute or chronic leukemia (including myelodysplastic syndrome); had failed previous CD34+ cell collection or collection attempts; had undergone a prior allogeneic transplant or more than one prior autologous transplant; had received their last anti-cancer therapy less than 4 weeks previously or less than 6 weeks if the prior therapy included nitrosourea or mitomycin; had bone marrow involvement >20 %; had received cytokines within 14 days prior to the first dose of G-CSF for mobilization; were positive for human immunodeficiency virus; had active hepatitis B or C; had an acute infection within 24 hours or antibiotic therapy within 7 days prior to the first dose of G-CSF; had hypercalcemia, as evidenced by a calcium concentration more than 1 mg/dL above the local laboratory upper limit of normal; had received investigational therapy within 4 weeks or been enrolled in another protocol during mobilization; had central nervous system involvement; were pregnant or breast-feeding; had cardiac ischemia or a history of a significant arrhythmia; or had co-morbid condition(s) which, in the opinion of the investigator, rendered the patient at high risk of treatment complications.
Treatment
The mobilization protocol consisted of G-CSF (10 μg/kg) subcutaneously daily for 4 days prior to the initiation of plerixafor. Plerixafor (0.24 mg/kg) was then administered subcutaneously on the evening of day 4. Patients underwent apheresis on day 5 following the morning dose of G-CSF, approximately 10 to 11 h after the dose of plerixafor (Figure 1). Plerixafor, G-CSF and apheresis were continued for up to 5 days or until ≥5×106 CD34+ cells/kg for lymphoma or ≥6×106 CD34+ cells/kg for MM had been collected. Following the last apheresis, patients underwent high-dose chemotherapy followed by autologous hematopoietic stem cell infusion according to institutional practices. Post-transplant G-CSF, transfusions and other supportive care procedures were also provided in accordance with institutional practices. Patients were followed for 12 months after transplantation and were evaluated after transplantation for safety and efficacy.
Figure 1.

Overall study design. PMN: polymorphonuclear cells. PLT: platelets.
Study objectives
The primary study objective was to confirm the safety of mobilization with plerixafor in patients with NHL and MM who were eligible to undergo treatment with autologous hematopoietic stem cell transplantation. Secondary objectives were to assess the efficacy of plerixafor and G-CSF as a mobilization regimen, as measured by the number of CD34+ cells collected in each apheresis session, and to assess the clinical effectiveness of plerixafor and G-CSF mobilized stem cells by examining hematopoietic cell engraftment and graft durability.
Safety outcomes
Safety was assessed by the incidence of adverse events, serious adverse events, deaths, treatment emergent adverse events and treatment emergent serious adverse events which were graded by investigators using the National Cancer Institute's Common Terminology Criteria for Adverse Events (version 3.0). A treatment emergent event was defined as an event occurring from the first dose of plerixafor up to 30 days after the last dose of plerixafor or until the first dose of myeloablative chemotherapy, whichever occurred first.
During the screening period (from signing the consent form to the first dose of G-CSF), only adverse events related to study procedures were recorded. All grade 3 and 4 treatment emergent adverse events and all treatment emergent serious adverse events were documented. Any adverse events regardless of grade, that occurred during the immediate post-injection time period (up to 1 h after plerixafor injection), and any adverse events, regardless of grade, that resulted in permanent discontinuation of plerixafor during the mobilization period were recorded. Any serious adverse events that occurred after the 30-day follow-up period which came to the attention of the site staff and which may have been causally related to the study drug were reported to the Sponsor regardless of time elapsed. All grade 3 or 4, study drugrelated adverse events and any serious adverse events were followed until resolution, return to baseline, or discontinuation of monitoring was mutually agreed upon by both the Investigator and the Sponsor's safety physician. Disease progression, graft failure, and/or death were reported as serious adverse events for up to 12 months after transplantation.
Efficacy outcomes
Efficacy outcome measures included the number of days of apheresis required to mobilize the minimum (≥2×106 CD34+ cells/kg) and optimum (≥5×106 CD34+ cells/kg for NHL and HD or ≥6×106 CD34+ cells/kg for MM) number of CD34+ cells/kg; the number of patients reaching minimum and optimum numbers of target CD34+ cells/kg within 4 days of apheresis; the number of CD34+ cells/kg collected per day of apheresis; the fold-increase in peripheral blood CD34+ cells; assessment of neutrophil and platelet engraftment following transplantation, and assessment of disease status.
Neutrophil engraftment was defined as an absolute neutrophil count ≥0.5×109/L for 3 consecutive days. Platelet engraftment was defined as a three consecutive platelet counts ≥20×109/L obtained over at least 7 days without transfusion. In addition, the date at which platelets reached ≥50×109/L measured by at least two values over at least 7 days without transfusion and the date at which hemoglobin reached ≥10 g/L without transfusion over the preceding 7 days were recorded. Delayed engraftment of platelets was defined as achieving a sustained platelet count of ≥20×109/L (stable for at least 7 days without transfusion) but not reaching ≥50 ×109/L, as defined by at least two consecutive platelet count measurements obtained over at least 7 days and occurring within 100 days post-transplant (day +100). Primary graft failure was defined as confirmation of one of the following in the absence of evidence of other causes such as recurrence or progression of cancer, renal failure, chronic bleeding, severe infection, drug-induced cytopenia, development of new hematologic problems (nutritional or otherwise): failure to achieve a sustained absolute neutrophil count of ≥0.5×109/L (defined by three consecutive laboratory values on 3 different days) within 30 days post-transplant (day +30) or failure to achieve a sustained platelet count ≥20×109/L (defined by at least three consecutive platelet count measurements obtained over at least 7 days without transfusion) within 100 days post-transplant (day +100). A durable graft was defined as the absence of primary and secondary graft failure.
Disease status was assessed according to internationally recognized criteria at each site. Patients were assessed for disease recurrence or progression and/or death during the first 12 months following transplantation. Investigators recorded the date and the criteria used to determine recurrence or progressive disease. Any deaths and the causes of deaths occurring during the study and up to the 12-month visit were recorded.
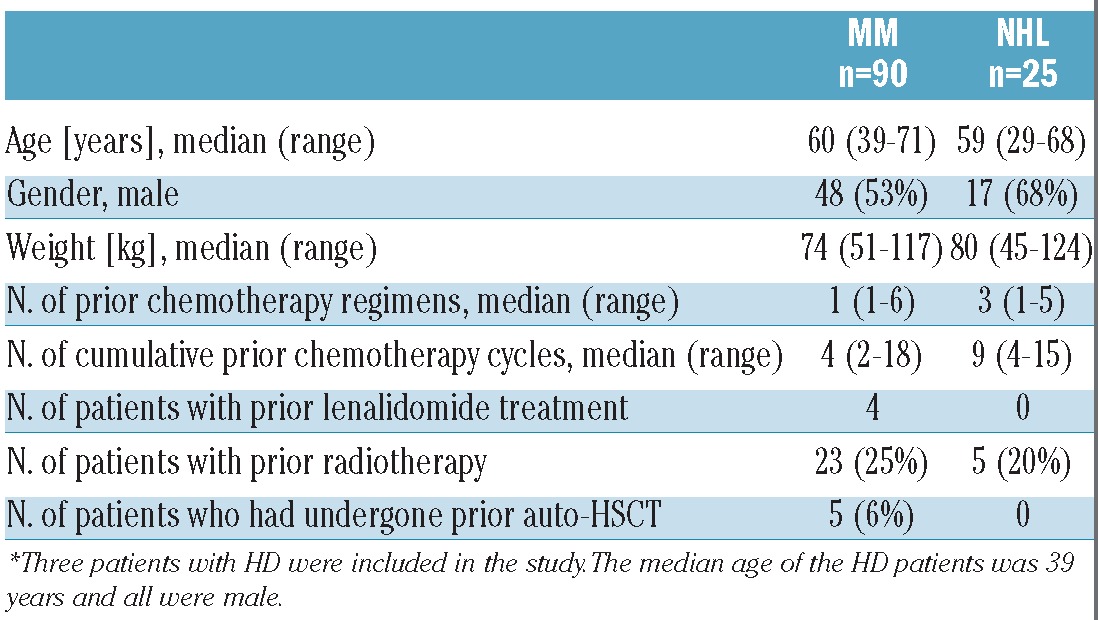
Results
A total of 126 patients were screened at 26 centers; of these 126 patients, 118 (MM=90, NHL=25, HD=3) received at least one dose of plerixafor. Overall, 114 (97%) patients underwent apheresis with 105 (89%) proceeding to transplantation. Eighty-nine (75%) patients completed the 12-month follow-up evaluation. The disposition of the patients during the study is displayed in Figure 2. Overall, the patients' age ranged from 22 to 71 years and 58% of the patients were male. The median number of prior chemotherapy regimens for NHL and MM patients was three (range, 1-5) and one (range, 1-6), respectively. The patients' baseline characteristics are presented in Table 1. Data for HD patients were included in the overall results, though subgroup analysis is footnoted in the tables because of the small size of the sample (n=3).
Figure 2.

Disposition of patients in the study.
Table 1.
Patients' baseline characteristics.*
Safety
Overall, 45 (38%) of 118 patients reported treatment emergent adverse events (events occurring during period 1) with only eight patients experiencing events graded 3 or higher. The most frequently occurring treatment emergent adverse events were diarrhea (7%), nausea (6%), and bone pain (4%). All other treatment emergent adverse events occurred in fewer than five (4%) patients.
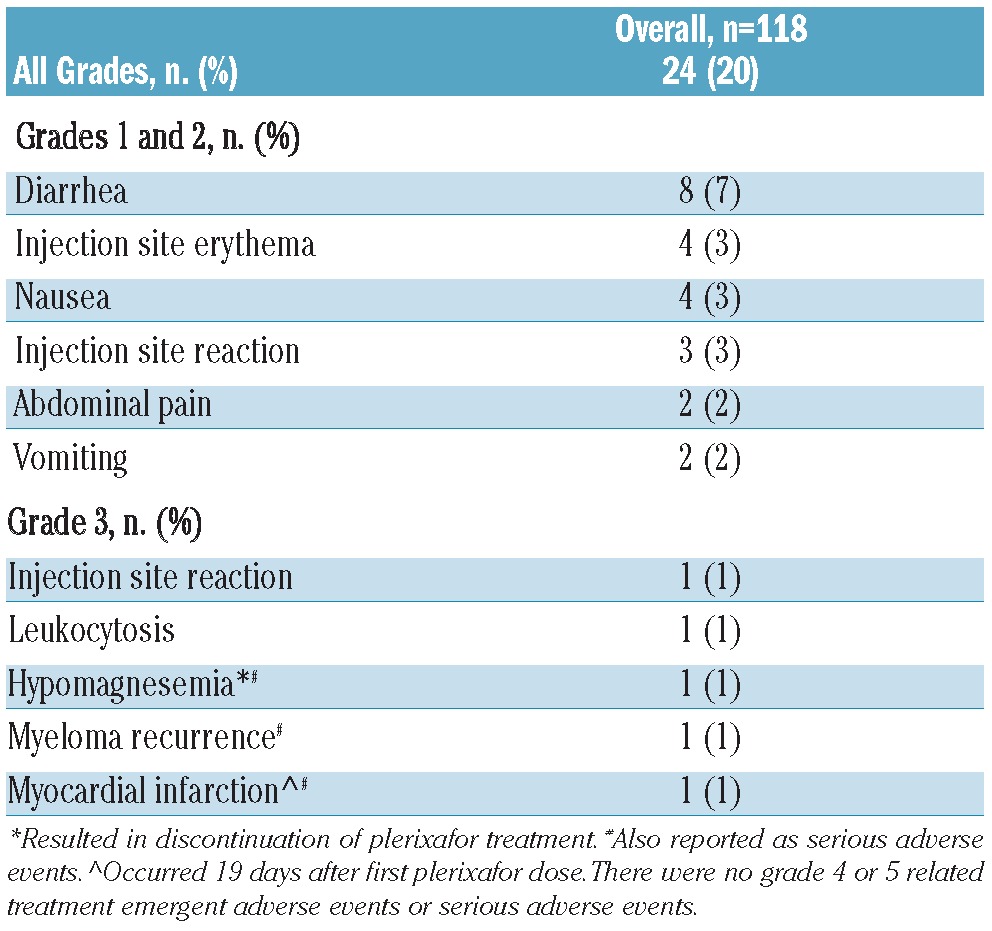
Twenty-four (20%) of 118 patients experienced at least one treatment emergent adverse event that was considered related to the study treatment. The majority of these treatment emergent adverse events occurred within 1 h post-injection and were of grade 1 or 2 in severity. The most commonly occurring treatment emergent adverse events (considered related to the study treatment) in order of decreasing frequency were: diarrhea (7%), injection site erythema (3%), nausea (3%), injection site reaction (3%), abdominal pain (2%), and vomiting (2%). All other related treatment emergent adverse events were each experienced by one patient only. Five MM patients experienced grade 3 events (Table 2): one patient had a myocardial infarction (grade 3, serious adverse event), one patient experienced myeloma relapse (grade 3, serious adverse event), one patient developed hypomagnesemia (grade 3, serious adverse event), one patient had an injection site reaction (grade 3, non-serious adverse event), and one patient developed leukocytosis (grade 3, non-serious adverse event). During periods 2 and 3 there were no non-serious treatment related adverse events, although one patient experienced serious adverse events of procedural complication (grade 3), neutropenia (grade 4) and thrombocytopenia (grade 4) that were considered possibly related to plerixafor.
Table 2.
Summary of treatment-emergent adverse events related to study treatment in period 1.
Two patients experienced treatment emergent adverse events leading to discontinuation or modification of the study treatment. One patient had a decrease in platelet count (not related to plerixafor) and the other patient had a decrease in blood magnesium levels (possibly related to plerixafor).
Four patients were reported to have died, with the earliest death occurring 46 days after the last dose of plerixafor. The deaths, considered unrelated to plerixafor, were due to relapse (n=1), liver failure likely due to disease progression (n=1), cardio-respiratory failure (n=1), and sepsis (n=1).
Mobilization
Among the 114 patients who underwent apheresis, 110 (96%) yielded the minimum required cell collection of ≥2×106 CD34+ cells/kg within a median of 1 day (range, 1 to 3) of apheresis [Table 3; data for HD patients (n=3) not included]. Analyzed by disease state, 20 (80%) patients within the NHL group and 88 (98%) patients within the MM group yielded the minimum target cell collection (Figure 3A). Ninety-four (82%) of all patients achieved the optimum target cell collection (i.e. ≥5×106 CD34+ cells/kg for NHL and HD or ≥6×106 CD34+ cells/kg for MM) within a median of 1 day (range, 1 to 4) of apheresis. Analyzed by disease state, 12 (48%) patients within the NHL group and 80 (89%) patients within the MM group achieved the optimum target cell collection (Figure 3B). Overall, the median fold increase in peripheral blood CD34+ cell count following the first dose of plerixafor was 2.6 (range, 0.2 to 94.0). The median total number of all CD34+ cells collected over 4 days was 7.3×106 CD34+ cells/kg (range, 0.1×106 to 24.0×106 CD34+ cells/kg).
Table 3.
Mobilization features **.
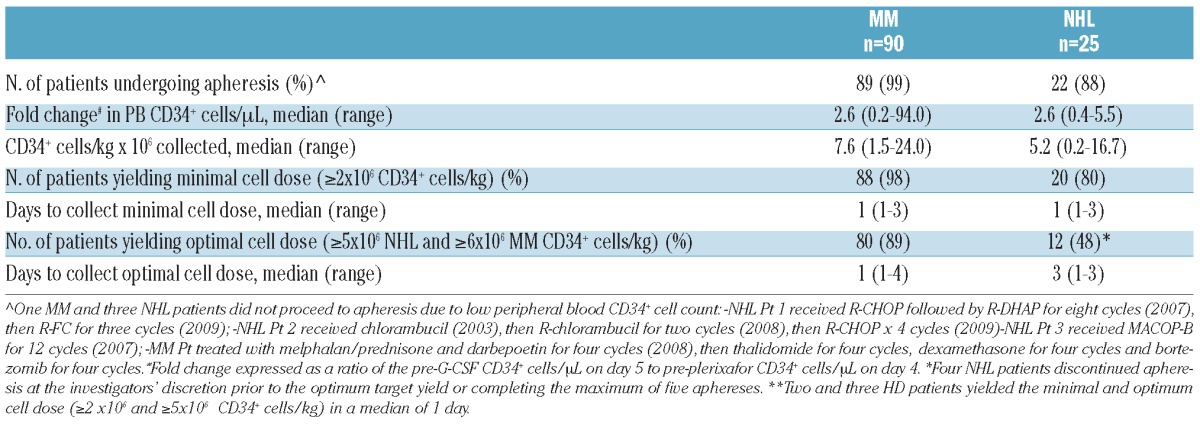
Figure 3.
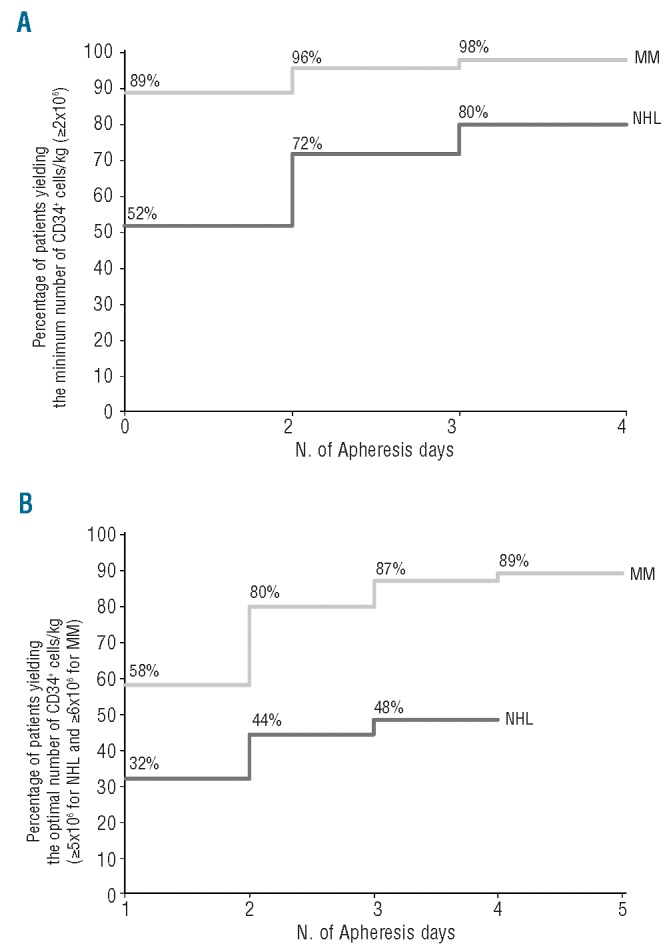
(A) Percentage of patients yielding the minimal (≥2×106) cell dose (≥2×106) by apheresis day. (B) Percentage of patients yielding the optimal CD34+ cell dose by apheresis day.
Transplantation and engraftment
One hundred (95%) of the 105 patients who underwent transplantation achieved neutrophil engraftment and 103 (98%) of 105 patients achieved platelet engraftment. The median times to neutrophil and platelet engraftment were 14 days (range, 9 to 61) and 18 days (range, 0 to 61), respectively. Two patients failed to achieve neutrophil engraftment while one patient failed to achieve platelet engraftment. Fifty-seven (54%) of 105 patients received G-CSF post-transplantation.
Overall, 105 patients received a single transplant, with no patient receiving a tandem transplant. At 100 days post-transplant, 97/100 patients assessed had a durable graft, at 6 months 96/99 patients assessed had a durable graft, and at 12 months post-transplant 85/89 patients assessed had a durable graft. There were no reports of secondary graft failure. Twelve patients had disease progression or recurrence within 12 months after their transplant. Three patients were off-study and one patient received an allogeneic transplant during the 12-month follow-up period.
Discussion
High-dose chemotherapy with or without radiation therapy is an effective treatment strategy for patients with NHL and MM. Currently, autologous transplants are almost all performed using peripheral blood as the source of stem cells. The major advantages of peripheral blood stem cell transplants over bone marrow transplants are that the stem cells can be harvested without general anesthesia, pain after bone marrow aspiration is eliminated and engraftment is faster. There are significant variations in practices used to mobilize and collect hematopoietic stem cells, depending on the type of agents combined in induction or salvage therapy, as well as on logistical and financial issues that differ from one center to another. These variations are present especially among European countries. While chemotherapy-based mobilization regimens may produce blood grafts with higher numbers of stem cells than when G-CSF is used alone, they are also associated with significant toxicities that may be less acceptable when the initial therapy does not include the administration of conventional cytotoxic agents, as exemplified by recent trends in the treatment of myeloma. Such changes in medical practices make it realistic to design optimized “non-chemo” mobilization regimens, offering the opportunity for an easier and mostly outpatient management.
Plerixafor is a newly approved CXCR4 chemokine-receptor antagonist for autologous hematopoietic stem cell mobilization. As part of the development program of this novel agent, the goal of the current prospective study was aimed to determine the safety and efficacy of plerixafor plus G-CSF for first-line mobilization in European patients with lymphoma or MM. Overall, 20% of patients experienced treatment emergent adverse events considered related to the treatment, with the majority being mild in severity (grade 1 or 2), and most occurring within 1 h after the injection. Three patients experienced serious adverse events: myocardial infarction (1 patient with MM), hypomagnesemia (1 patient with NHL), and myeloma recurrence (1 patient with MM) which were considered possibly related to the study treatment. The myocardial infarction occurred 19 days after the last dose of plerixafor; this adverse event has previously been noted following G-CSF administration, although the mechanism, frequency and temporal relationship to G-CSF are uncertain.15 The half-life of plerixafor is approximately 3 to 5 h and plerixafor-mediated changes in white blood cell and CD34+ cell counts wane by 24 h post-dose. Based on these data, the effects of plerixafor would not be expected to increase the risk of myocardial infarction following stem cell mobilization. Disease relapse is not often described as an adverse event, but was listed as such in this study in an effort to capture all occurrences across all sites, because mobilization of cancer stem cells, contamination of apheresis products and consequent contribution to disease relapse is a theoretical concern with all peripheral blood autologous stem cell transplants. Overall, the safety profile is in line with already published data and confirmed the favorable benefit-risk ratio of this novel agent.
Efficacy results from this study showed that 96% of the patients yielded the minimum cell collection of ≥2×106 CD34+ cells/kg. The number of patients who yielded the optimum target cell collection of ≥5×106 CD34+ cells/kg for NHL or ≥6×106 CD34+ cells/kg for MM in a median of 1 day of apheresis (range, 1 to 4 days) by disease group was 12/25 (48%) for patients with NHL and 80/90 (89%) for patients with MM. In the phase III study AMD3100-3101, 89/150 (59%) of patients with NHL yielded the target cell collection (≥5×106 CD34+ cells/kg), which appears to deviate from the 48% of patients who yielded this amount in PREDICT. The small sample size of the NHL group in PREDICT makes it difficult to draw meaningful conclusions regarding this deviation from the pivotal phase III study.
Overall, the median fold increase in peripheral blood CD34+ cell count following the first dose of plerixafor was 2.6, and the median total number of all CD34+ cells collected over 4 days was 7.3×106 CD34+ cells/kg. These results are compatible with the results from other studies on the efficacy of plerixafor in these populations of patients.
Overall 95% of patients who underwent transplantation achieved neutrophil engraftment in a median of 14 days (range, 9 to 61 days) and 98% of patients achieved platelet engraftment in a median of 18 days (range, 0 to 61 days). It is important to note that neutrophil engraftment was strictly monitored in this study, unlike in routine clinical practice and most observational and retrospective studies, in which the exact day of neutrophil and platelet recovery is often not captured since the patient has been discharged from the hospital and only returns episodically to the outpatient clinic. These median times to engraftment are within the ranges expected for this patient population, although 18 patients did not engraft polymorphonuclear cells within 22 days post-transplantation and 31 patients did not achieve platelet engraftment within 22 days. Patients with lymphoma and MM usually have neutrophil engraftment within 12 days after transplantation, but it may occur as late as 21 days post-transplant.1,16 Platelet engraftment generally occurs about 1 week after neutrophil engraftment, but times to platelet engraftment are more variable. One factor which may have influenced the number of days to neutrophil engraftment (a median of 15 days for patients with NHL and 14 days for patients with MM in PREDICT compared with 10 days for NHL and 11 days for MM in phase III studies) was that 48/105 (46%) patients did not receive G-CSF post-transplant, whereas in the phase III studies all patients received G-CSF from the fifth or sixth day post-transplant until neutrophil engraftment. Another factor which may have contributed to some extended times to platelet engraftment (maximum 61 days) in PREDICT was that according to the standard of care at some sites, patients returned home after neutrophil engraftment. In these cases blood samples for assessment of platelet engraftment would not have been taken daily, potentially giving an inflated number of days to platelet engraftment as the true date of engraftment could fall on a day when no assessment was made.
Based on outcomes from the current trial and from previous trials, as well as on data obtained from the compassionate use program in both the USA and European Union, plerixafor appears to be an effective, safe and efficient approach to improve already existing mobilization regimens. Further, the combination of plerixafor with G-CSF may represent an alternative to the administration of myelosuppressive agents such as cyclophosphamide when this is not strictly required by treatment of the underlying malignancy, as is increasingly the case for patients with MM. Whether the additional costs linked to the introduction of plerixafor can be offset by reduced use of other hospital resources (reduced number of aphereses, no need for inpatient administration of myelosuppressive agents, no occurrence of febrile neutropenia, etc.) will require further economic evaluations.
Acknowledgments
Funding: This study was funded by Sanofi Oncology (previously Genzyme Corporation).
Footnotes
Authorship and Disclosures: Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Gazitt Y, Freytes CO, Callander N, Tsai TW, Alsina M, Anderson J, et al. Successful PBSC mobilization with high-dose G-CSF for patients failing a first round of mobilization. J Hematother. 1999;8(2):173-83 [DOI] [PubMed] [Google Scholar]
- 2.Porrata LF, Gertz MA, Inwards DJ, Litzow MR, Lacy MQ, Tefferi A, et al. Early lymphocyte recovery predicts superior survival after autologous hematopoietic stem cell transplantation in multiple myeloma or non-Hodgkin lymphoma. Blood. 2001;98(3):579-85 [DOI] [PubMed] [Google Scholar]
- 3.Lazarus HM, Loberiza FR, Jr., Zhang MJ, Armitage JO, Ballen KK, Bashey A, et al. Autotransplants for Hodgkin's disease in first relapse or second remission: a report from the autologous blood and marrow transplant registry (ABMTR). Bone Marrow Transplant. 2001;27(4):387-96 [DOI] [PubMed] [Google Scholar]
- 4.Sureda A, Arranz R, Iriondo A, Carreras E, Lahuerta JJ, Garcia-Conde J, et al. Autologous stem-cell transplantation for Hodgkin's disease: results and prognostic factors in 494 patients from the Grupo Espanol de Linfomas/Transplante Autologo de Medula Osea Spanish Cooperative Group. J Clin Oncol. 2001;19(5):1395-404 [DOI] [PubMed] [Google Scholar]
- 5.Allan DS, Keeney M, Howson-Jan K, Popma J, Weir K, Bhatia M, et al. Number of viable CD34(+) cells reinfused predicts engraftment in autologous hematopoietic stem cell transplantation. Bone Marrow Transplant. 2002;29(12):967-72 [DOI] [PubMed] [Google Scholar]
- 6.Wuchter P, Ran D, Bruckner T, Schmitt T, Witzens-Harig M, Neben K, et al. Poor mobilization of hematopoietic stem cells -definitions, incidence, risk factors and impact on outcome of autologous transplantation. Biol Blood Marrow Transplant. 2010;16(4):490-9 [DOI] [PubMed] [Google Scholar]
- 7.Giralt S, Stadtmauer E, Harousseau J, Palumbo A, Bensinger W, Comenzo R, et al. International Myeloma Working Group (IMWG) consensus statement and guidelines regarding the current status of stem cell collection and high-dose therapy for multiple myeloma and the role of plerixafor (AMD 3100). Leukemia. 2009;23(10):1904-12 [DOI] [PubMed] [Google Scholar]
- 8.van Der Auwera P, Platzer E, Xu ZX, Schulz R, Feugeas O, Capdeville R, et al. Pharmacodynamics and pharmacokinetics of single doses of subcutaneous pegylated human G-CSF mutant (Ro 25-8315) in healthy volunteers: comparison with single and multiple daily doses of filgrastim. Am J Hematol. 2001;66(4):245-51 [DOI] [PubMed] [Google Scholar]
- 9.Cassens U, Momkvist PH, Zuehlsdorf M, Mohr M, Kienast J, Berdel WE, et al. Kinetics of standardized large volume leukapheresis (LVL) in patients do not show a recruitment phenomenon of peripheral blood progenitor cells (PBPC). Bone Marrow Transplant. 2001;28(1):13-20 [DOI] [PubMed] [Google Scholar]
- 10.Pusic I, Jiang S, Landua S, Uy G, Rettig M, Cashen A, et al. Impact of mobilization and remobilization strategies on achieving sufficient stem cell yields for autologous transplantation. Biol Blood Marrow Transplant. 2008;14(9):1045-56 [DOI] [PubMed] [Google Scholar]
- 11.Pusic I, DiPersio J. The use of growth factors in hematopoietic stem cell transplantation. Current Pharmaceutical Design. 2008;14(20):1950-61 [DOI] [PubMed] [Google Scholar]
- 12.DiPersio J F, Micallef IN, Stiff PJ, Bolwell BJ, Maziarz RT, Jacobsen E, et al. Phase III prospective randomized double-blind placebo-controlled trial of plerixafor plus granulocyte colony-stimulating factor compared with placebo plus granulocyte colony-stimulating factor for autologous stem-cell mobilization and transplantation for patients with non-Hodgkin's lymphoma. J Clin Oncol. 2009;27(28):4767-73 [DOI] [PubMed] [Google Scholar]
- 13.DiPersio JF, Stadtmauer EA, Nademanee A, Micallef IN, Stiff PJ, Kaufman JL, et al. Plerixafor and G-CSF versus placebo and G-CSF to mobilize hematopoietic stem cells for autologous stem cell transplantation in patients with multiple myeloma. Blood. 2009;113(23):5720-6 [DOI] [PubMed] [Google Scholar]
- 14.Mozobil [Summary of Product Characteristics], Naarden, Netherlands: Genzyme Europe B.V.:2010 [Google Scholar]
- 15.Neupogen [Prescribing Information]. Thousand Oaks, CA: Amgen Inc.:2012 [Google Scholar]
- 16.Tricot G, Jagannath S, Vesole D, Nelson J, Tindle S, Miller L, et al. Peripheral blood stem cell transplants for multiple myeloma: identification of favorable variables for rapid engraftment in 225 patients. Blood. 1995;85(2):588-96 [PubMed] [Google Scholar]