

Abstract
The optimal post-remission treatment for acute myeloid leukemia in first complete remission remains uncertain. Previous comparisons of autologous versus allogeneic hematopoietic cell transplantation noted higher relapse, but lower treatment-related mortality though using bone marrow grafts, with treatment-related mortality of 12-20%. Recognizing lower treatment-related mortality using autologous peripheral blood grafts, in an analysis of registry data from the Center for International Blood and Transplant Research, we compared treatment-related mortality, relapse, leukemia-free survival, and overall survival for patients with acute myeloid leukemia in first complete remission (median ages 36-44, range 19-60) receiving myeloablative HLA-matched sibling donor grafts (bone marrow, n=475 or peripheral blood, n=428) versus autologous peripheral blood (n=230). The 5-year cumulative incidence of treatment-related mortality was 19% (95% confidence interval, 16-23%), 20% (17-24%) and 8% (5-12%) for allogeneic bone marrow, allogeneic peripheral blood and autologous peripheral blood stem cell transplant recipients, respectively. The corresponding figures for 5-year cumulative incidence of relapse were 20% (17-24%), 26% (21-30%) and 45% (38-52%), respectively. At 5 years, leukemia-free survival and overall survival rates were similar: allogeneic bone marrow 61% (56-65%) and 64% (59-68%); allogeneic peripheral blood 54% (49-59%) and 59% (54-64%); autologous peripheral blood 47% (40-54%) and 54% (47-60%); P=0.13 and P=0.19, respectively. In multivariate analysis the incidence of treatment-related mortality was lower after autologous peripheral blood transplantation than after allogeneic bone marrow/peripheral blood transplants [relative risk 0.37 (0.20-0.69); P=0.001], but treatment failure (death or relapse) after autologous peripheral blood was significantly more likely [relative risk 1.32 (1.06-1.64); P=0.011]. The 5-year overall survival, however, was similar in patients who received autologous peripheral blood (n=230) [relative risk 1.23 (0.98-1.55); P=0.071] or allogeneic bone marrow/peripheral blood (n=903). In the absence of an HLA-matched sibling donor, autologous peripheral blood may provide acceptable alternative post-remission therapy for patients with acute myeloid leukemia in first complete remission.
Introduction
Optimal post-remission strategies for acute myeloid leukemia in first complete remission remain controversial. Autologous hematopoietic cell transplantation with bone marrow or peripheral blood and allogeneic blood or marrow transplantation from an HLA-matched sibling donor are potentially curative for many patients with acute myeloid leukemia in first complete remission. At many centers, the preferred approach is allogeneic hematopoietic cell transplantation from a matched sibling donor or HLA-matched unrelated donors for patients with intermediate or high risk cytogenetic or molecular abnormalities. Allogeneic hematopoietic cell transplantation has not been shown to benefit certain categories of patients with favorable risk features.1 Consolidation chemotherapy is another option for those with intermediate or favorable risk characteristics.2 For patients without a suitable donor, autologous transplantation is also a valid option.3
Controlled prospective trials comparing consolidation chemotherapy with autologous bone marrow transplantation and biological randomization to HLA-identical matched sibling donor myeloablative transplantation conducted in the mid-1990s favored the allogeneic bone marrow strategy because of a lower probability of relapse, despite the high incidence of treatment-related mortality of up to 30%.3-7 In all of the prospective studies, and in general during this period, autotransplants were performed with a bone marrow graft and led to treatment-related mortality rates of 8-20%, considerably more than with consolidation chemotherapy. Since the completion of these trials, the stem cell source for autologous transplantation has shifted from bone marrow to peripheral blood. More recent literature suggests that the treatment-related mortality is significantly lower after autologous peripheral blood cell transplantation and the reported treatment-related mortality in many series was less than 5%.8-14 One study analyzed outcomes of patients with acute myeloid leukemia in first complete remission after post-remission consolidation therapy based on donor versus no donor availability, but did not specifically investigate the cohort receiving only autologous peripheral blood cells.15
A recent, large prospective randomized trial of peripheral blood autotransplantation versus intensive consolidation chemotherapy showed a lower relapse rate and superior relapse-free survival, but similar overall survival for the autotransplanted cohort.3 The non-relapse mortality rate was 4% versus 1% for patients undergoing only consolidation chemotherapy. The majority of patients in that study had intermediate risk cytogenetics.
We were interested in determining the effect of the lower treatment-related mortality rate obtained with peripheral blood autografts reported since the earlier prospective trials and whether the benefit of lower treatment-related mortality with autologous peripheral blood cell transplantation translated into better outcomes compared with those of either allogeneic bone marrow or allogeneic peripheral blood transplantation.
The Center for International Blood and Marrow Transplant Research (CIBMTR) database offers a unique opportunity to conduct a comparative evaluation. We recognize the inherent limitations of a retrospective analysis of observational databases, especially in studies of hematopoietic cell transplantation in which factors affecting the patients' selection cannot be fully determined. Here, we confirm the lower treatment-related mortality associated with autologous peripheral blood cell transplantation and report that survival was similar among patients undergoing allogeneic transplantation with peripheral blood or bone marrow from a matched sibling donor for acute myeloid leukemia in first complete remission. Our data suggest that given the similar survival outcomes, future studies addressing post-remission strategies for acute myeloid leukemia in first complete remission should include consideration of autologous peripheral blood hematopoietic cell transplantation together with post-transplant treatment strategies and appropriate stratification for prognostic factors.
Design and Methods
Data sources
The CIBMTR receives data on consecutive allogeneic and autologous hematopoietic cell transplants from more than 450 transplantation centers worldwide. The data are collected at the Statistical Center at the Medical College of Wisconsin in Milwaukee and the National Marrow Donor Program (NMDP) Coordinating Center in Minneapolis with computerized checks for discrepancies, physicians' review of submitted data and on-site audits of participating centers to ensure data quality. The CIBMTR collects both Transplant Essential Data and Comprehensive Report Form data prior to the transplant, 100 days and 6 months post-transplant and annually thereafter.
Observational studies conducted by the CIBMTR are performed with approval of the Institutional Review Boards of the NMDP and the Medical College of Wisconsin.
Patients
The study included all patients 19-60 years of age in first complete remission who underwent autologous peripheral blood transplantation or HLA-identical matched sibling donor myeloablative allogeneic bone marrow or peripheral blood transplantation for acute myeloid leukemia between 1995 and 2004, whose data were reported to the CIBMTR. Patients with M3 acute myeloid leukemia, granulocytic sarcoma, a known previous myelodysplastic syndrome or prior malignancy, and those who underwent syngeneic, T-cell depleted, umbilical cord blood or non-myeloablative transplants were excluded.
Cytogenetic risk categories were defined using the South West Oncology Group criteria. Good prognosis cytogenetics include: 16q, t(8;21) and t(15;17); intermediate prognosis cytogenetics include: +8, +21, t(1;7) and t(8;16); other abnormalities and poor prognosis cytogenetics include: -5/5q-, -7/7q-, -20/20q-, 3q, 11q, t(5;7), t(9;22) and t(6;9). Pre-transplant remission status was confirmed by morphological analysis of the bone marrow.
Endpoints
Primary endpoints were treatment-related mortality, morphological leukemia relapse (hematologic and/or extramedullary), leukemia-free survival and its converse, treatment failure, and overall survival. Treatment-related mortality was defined as death during continuous complete remission following hematopoietic cell transplantation. Relapse was defined as clinical or hematologic leukemia recurrence. For analyses of leukemia-free survival, failures were considered to be clinical or hematologic relapses or deaths from any cause; patients alive and in complete remission were censored at the time of last follow-up. For analyses of overall survival, failure was considered to be death from any cause; surviving patients were censored at the date of last contact.
Statistical analysis
Patient-, disease-, and transplant-related variables among the three groups (allogeneic bone marrow, allogeneic peripheral blood or autologous peripheral blood transplant recipients) were compared using the chi-square statistic for categorical variables and the Kruskal-Wallis test for continuous variables. Univariate probabilities of leukemia-free and overall survival were calculated using the Kaplan-Meier estimator,16 with the variance estimated by Greenwood's formula. Probabilities of relapse and treatment-related mortality were calculated using cumulative incidence curves to accommodate competing risks.17-19
Assessments of potential risk factors for outcomes of interest were evaluated in multivariate analyses using the pseudo-value technique.20,21 These analyses fit models to determine which risk factors are related to a given outcome. The pseudo-value technique is used to analyze survival data on predetermined time points when proportional assumptions needed for the Cox model22 do not hold for overall survival. For 5-year overall and leukemia-free survival, pseudo-values were computed using the Kaplan-Meier estimator for the survival function and a generalized linear model with complementary log-log link function.
The variables considered in the multivariate analyses were age at transplant (≤40 years versus >40 years), gender (female versus male), Karnofsky performance score (≥90% versus <90% versus unknown), French-American-British subtype (M0-M2 versus M4-M7 versus other/unclassified), white blood cell count at diagnosis (<20×109/L versus 20-50×109/L versus 50-100×109/L versus >100×109/L), cytogenetics (no abnormalities or intermediate versus good versus poor prognosis versus unknown), extramedullary disease (no versus yes), time from diagnosis to transplantation, time from first complete remission to transplantation, chemotherapy cycles to achieve complete remission (1 versus >1), consolidation therapy prior to transplantation (none versus 1 versus ≥2 versus unknown), consolidation therapy prior to transplantation (standard dose cytarabine versus high dose cytarabine versus other drugs versus no therapy) and year of transplantation (1995-1999 versus 2000-2004).
An initial analysis determined cut points for low/high risk groups for two continuous variables (time from diagnosis to transplantation and time from first complete remission to transplantation) by multivariate analysis of overall survival at 5 years, based on pseudo-values and the Wald test statistic. Using the cut points obtained, regression models (generalized linear models with complementary log-log link function) were fitted to each time point for both overall survival and leukemia-free survival. The estimated hazard ratios of the final models are shown. Initially, an analysis was performed with each model containing the main effect for type of transplant (allogeneic bone marrow versus allogeneic peripheral blood versus autologous peripheral blood). However, risks associated with allogeneic bone marrow and allogeneic peripheral blood were virtually identical in all analyses, so final models show only the relative risk (RR) of each outcome for patients receiving any allotransplant (bone marrow/peripheral blood) versus those receiving an autologous peripheral blood cell transplant. Variables not listed in the final models did not meet the 0.05 level of statistical significance. All computations were performed using the generalized linear model with complementary log-log link function in the statistical package of SAS version 9”. All P values are two-sided.
Results
Patients and clinical characteristics
A total of 1133 patients from 205 reporting centers in 38 countries met our study criteria. of whom 475 underwent allogeneic bone marrow transplantation, 428 underwent allogeneic peripheral blood cell transplantation and 230 underwent autologous peripheral blood cell transplantation. The median follow-up of survivors for the three groups (allogeneic bone marrow, allogeneic peripheral blood and autologous peripheral blood) was 82 (6-149), 61 (4-144), and 62 (1-139) months, respectively. Table 1 shows the patient-, disease- and transplant-related characteristics of the study patients and the decreasing use of autologous transplantation in more recent years of the study.
Table 1.
Characteristics of the patients.
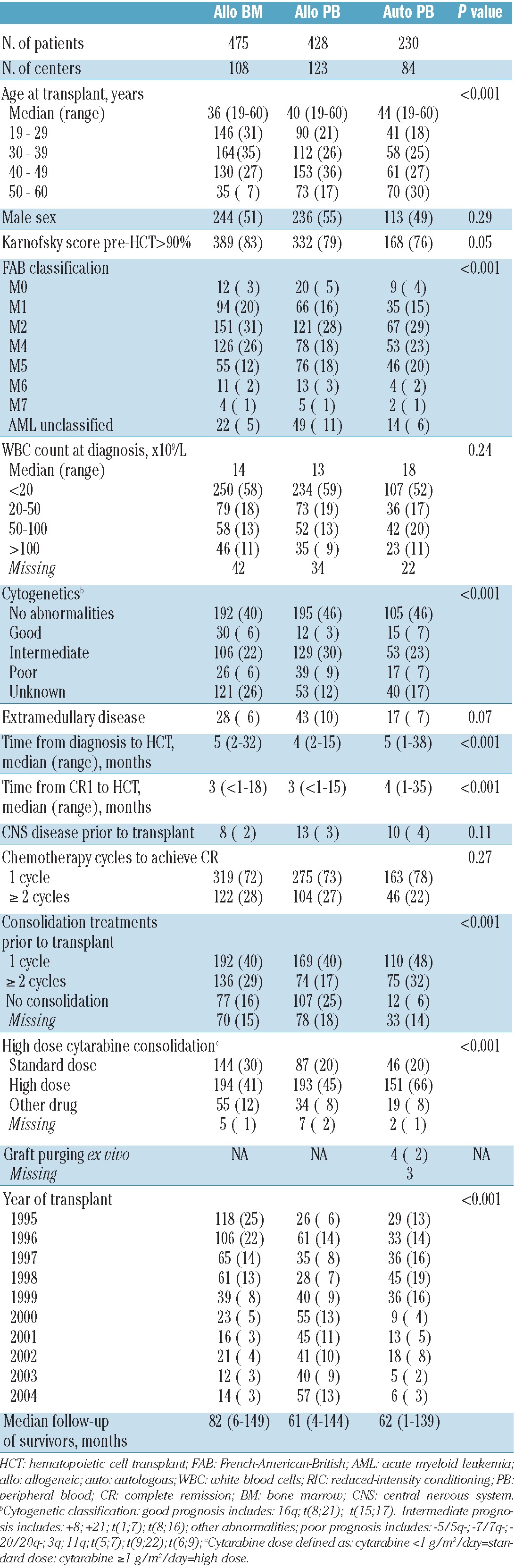
Figure 1.
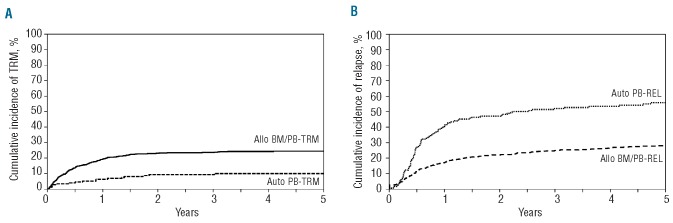
Cumulative incidence of (A) treatment-related mortality (TRM) in patients with acute myeloid leukemia in first complete remission by type of transplant; (B) Relapse (REL) in patients with acute myeloid leukemia in first complete remission by type of transplant. auto: autologous; allo: allogeneic; BM: bone marrow; PB: peripheral blood.
Treatment-related mortality
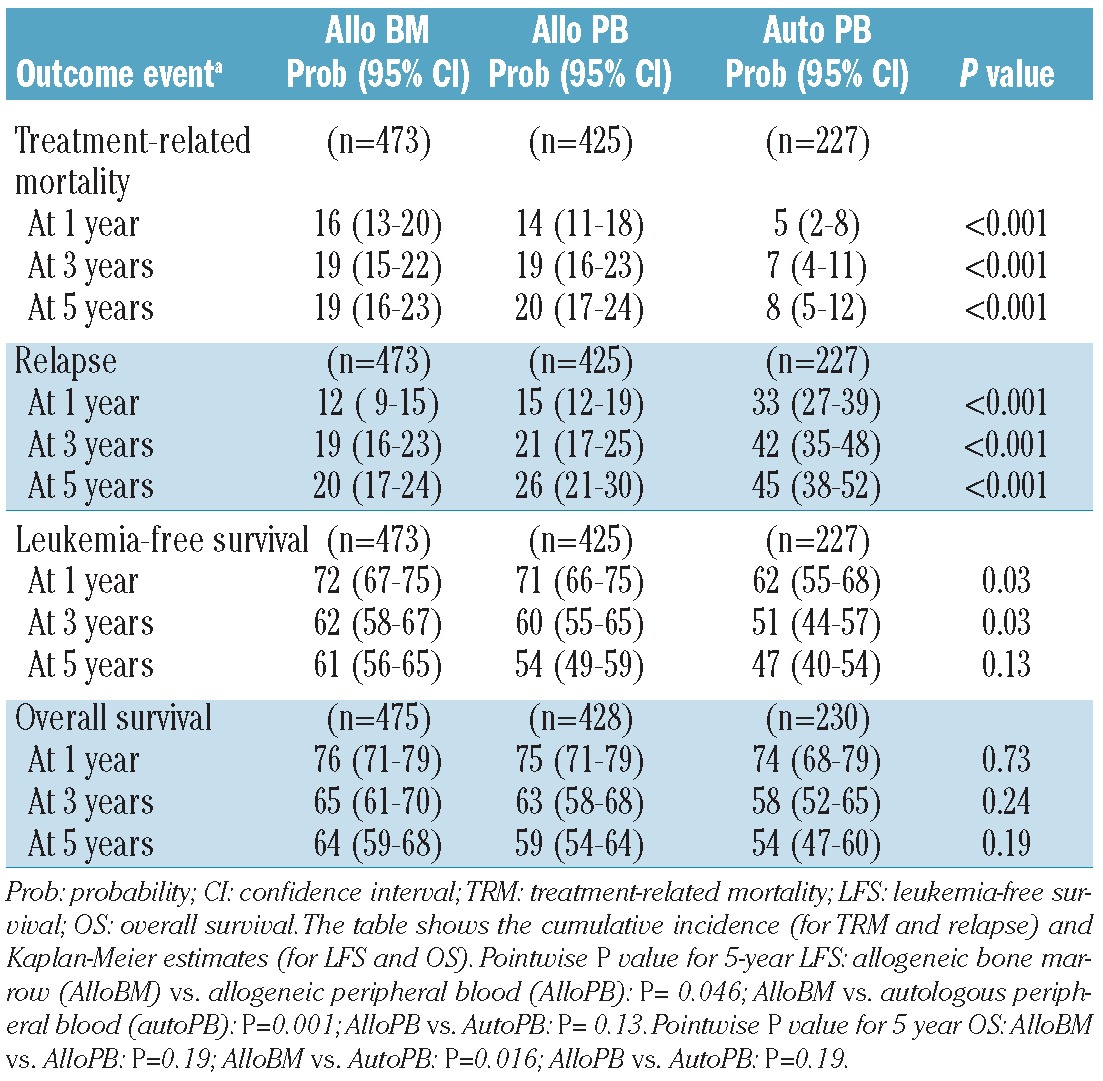
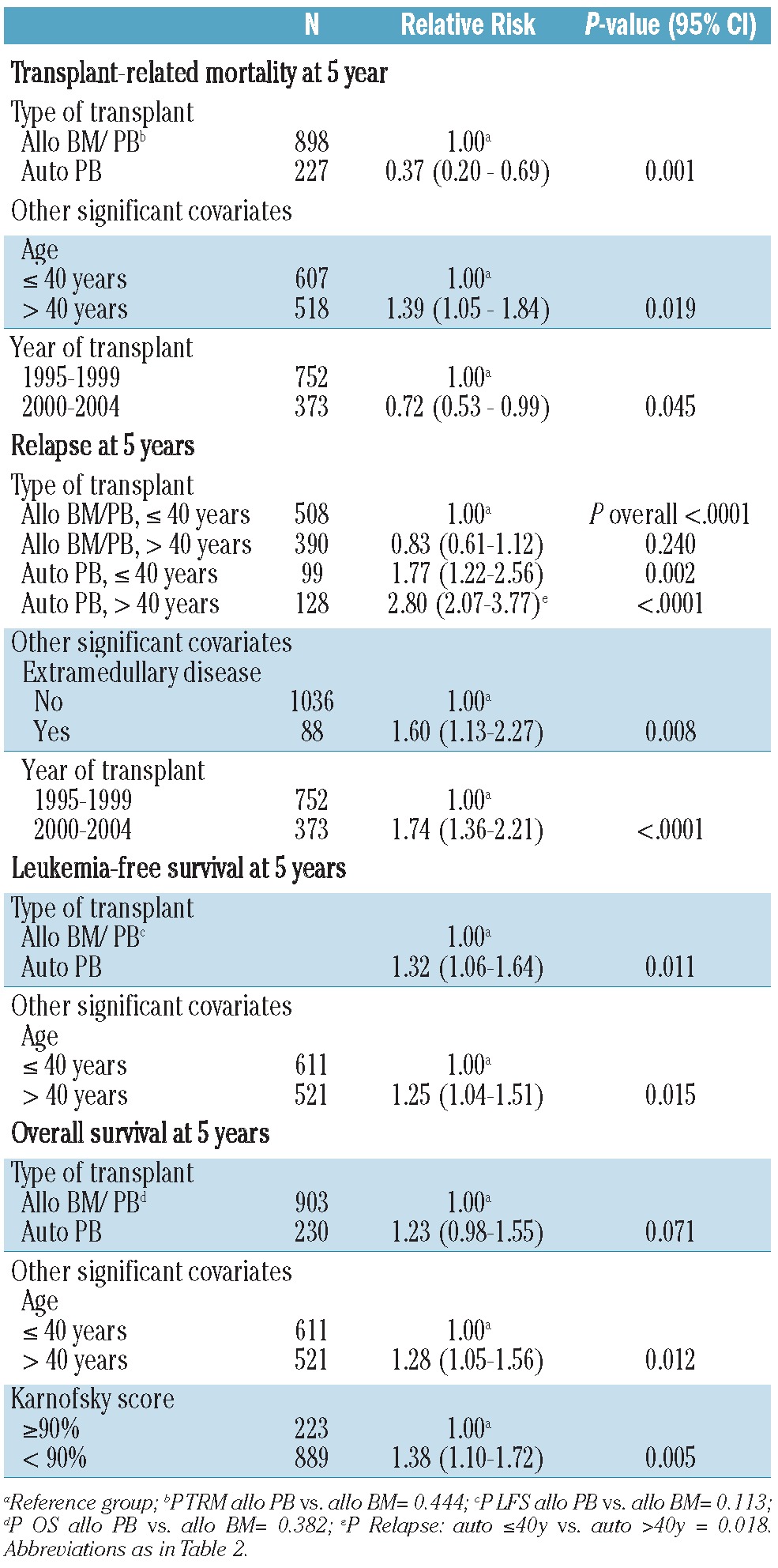
In univariate analysis (Table 2), the rate of treatment-related mortality at 5 years was significantly lower after autologous peripheral blood cell transplantation (8%; 95% CI 5-12) than after allogeneic peripheral blood (20%; 95% CI 17-24) or allogeneic bone marrow (19%; 95% CI 16-23) transplantation (P<0.001). In multivariate analysis, other independent factors associated with increased treatment-related mortality at 5 years were age >40 years and transplantation before the year 2000. In univariate analysis, treatment-related mortality at 5 years among patients transplanted between 2000 and 2004 was 10% (95% CI 6-15) for allogeneic peripheral blood recipients and 0% for autologous peripheral blood recipients (n=51; 22 disease-free, 29 relapsed).
Table 2.
Univariate probabilities of transplant outcomes.
Relapse
In univariate analysis (Table 2), the 5-year relapse rate was significantly higher among patients undergoing autologous peripheral blood cell transplantation (45%; 95% CI 38-52) than those undergoing allogeneic peripheral blood (26%; 95% CI 21-30) or allogeneic bone marrow (20%; 95% CI 17-24) transplantation (P<0.001). In multivariate analysis, age did not influence risk of relapse after allogeneic bone marrow or peripheral blood transplantation, but there was an increased risk of relapse in older (>40 years) autologous peripheral blood recipients (P=0.018) (Table 3). Other independent factors associated with increased relapse were presence of extramedullary disease and transplantation performed after the year 2000 (Table 3). For patients with and without extramedullary disease, the 5-year probabilities of relapse for allogeneic bone marrow, allogeneic peripheral blood and autologous peripheral blood recipients were 21% (95% CI 9-38) and 20% (95% CI 17-24)(P=0.88); 44% (95% CI 29-60) and 24% (95% CI 19-28) (P=0.013); and 47% (95% CI 25-70) and 45% (95% CI 38-52) (P=0.86), respectively.
Table 3.
Multivariate analysis of transplant outcomes.
Leukemia-free and overall survival
By univariate analysis, the 5-year leukemia-free survival rates for allogeneic bone marrow, allogeneic peripheral blood and autologous peripheral blood recipients were 61% (95% CI 56-65), 54% (95% CI 49-59) and 47% (95% CI 40-54), respectively (Table 2) (P=0.13). The univariate pairwise comparisons (pointwise P values at 5 years) showed an advantage for the allogeneic bone marrow transplant strategy over the other two approaches: allogeneic bone marrow versus allogeneic peripheral blood (P=0.046); allogeneic bone marrow versus autologous peripheral blood (P=0.001); and allogeneic peripheral blood versus autologous peripheral blood (P=0.13). In multivariate analysis, allogeneic hematopoietic cell transplantation was associated with a significantly lower risk of treatment failure (relapse or death) at 5 years (Table 3, P=0.01). The only factor associated with increased risk of treatment failure was older age of the recipient at the time of transplantation. For patients ≤40 years of age, the 5-year leukemia-free survival was the same for allogeneic peripheral blood/bone marrow recipients and the autologous peripheral blood recipients; 54% (46-61) versus 57% (47-67).
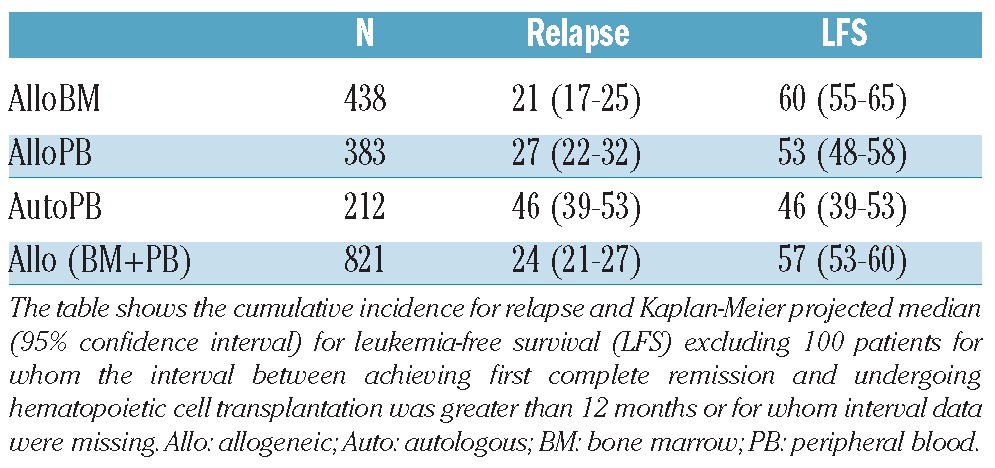
To assess the potential value of hematopoietic cell transplantation for patients transplanted after a shorter period of first complete remission, the data were reanalyzed including only those patients transplanted within 12 months of achieving complete remission; excluding 10% of allogeneic bone marrow/peripheral blood recipients and 6.6% autologous peripheral blood cases from the analysis. The 5-year probabilities of relapse and leukemia-free survival were unchanged (Table 4).
Table 4.
Five-year relapse and leukemia-free survival for patients transplanted within 12 months of achieving first complete remission.
At 5 years, the overall survival probabilities for allogeneic bone marrow, allogeneic peripheral blood and autologous peripheral blood recipients were 64% (59-68%), 59% (54-64%) and 54% (47-60%), respectively (Table 2) (P=0.19). By pairwise comparison, overall survival was significantly better for allogeneic bone marrow recipients versus autologous peripheral blood recipients (P=0.016), but similar for allogeneic bone marrow versus allogeneic peripheral blood (P=0.19) and allogeneic peripheral blood versus autologous peripheral blood (P=0.19) recipients. The multivariate adjusted survival analysis showed that risks of death did not differ significantly between patients who received an allogeneic bone marrow/peripheral blood or autologous peripheral blood (Table 3, P=0.07) transplant. Independently of the type of transplant, the risk of death was significantly higher in older patients (age >40 years) and those with lower Karnofsky scores. For patients ≤40 years old with a Karnofsky score of >90%, overall survival rates for recipients of allogeneic peripheral blood (n=156), allogeneic bone marrow/peripheral blood (n=418), and autologous peripheral blood (n= 74) were identical: 64% (56-72%), 66% (61-71%), and 63% (51-74%), respectively. For patients >40 years old with a Karnofsky score of <90%, 5-year survival rates, although inferior to those of younger patients with excellent performance status, were also similar between recipients of allogeneic bone marrow/peripheral blood (n=83) and autologous peripheral blood (n=34): 47% (36-57%) versus 48% (31-65%).
Cytogenetics did not influence any outcomes analyzed among the groups in this study. The large majority (69%) of patients had either normal or intermediate risk cytogenetics, while the frequency of good or poor risk cytogenetics was less than 10% (3-7% and 6-9%, respectively). Due to the importance of this intermediate risk cohort, a limited re-analysis of those with intermediate risk or normal cytogenetics was performed. It demonstrated that leukemia-free survival and overall survival in those receiving allogeneic bone marrow were 58% (52-63%) and 61% (55-67%), with the corresponding figures for recipients of allogeneic peripheral blood being 56% (50-61%) and 62% (56-67%) and those for autologous peripheral blood recipients being 48% (40-56%) and 54% (46-62%), respectively, similar to our findings in the entire cohort. Multivariate analysis demonstrated concordance as well, with similar risks of overall survival (RR 1.21; 95% CI 0.92-1.59, P=0.172) and leukemia-free survival (RR 1.27; 95% CI 0.98-1.65, P=0.071) in those receiving autologous peripheral blood compared with the allogeneic bone marrow/peripheral blood group.
The numbers of patients who received a second transplant among the allogeneic bone marrow, allogeneic peripheral blood and autologous peripheral blood cohorts were 36 (7.6%), 54 (12.7%) and 26 (11.5%), respectively. The frequency was, however, higher among patients who underwent autologous peripheral blood transplantation in the period from 2000 to 2004: 11 of 51 (21.6%). To account for the possible effect of second transplants and other potential factors on these later outcomes, overall survival rates were determined at 1 and 5 years after leukemia relapse for allogeneic bone marrow/peripheral blood (n=212) and autologous peripheral blood (n=99) recipients, being 31% (16-48%) and 10% (6-15%) versus 28% (19-38%) and 8% (2-16%), respectively.
Figure 2.
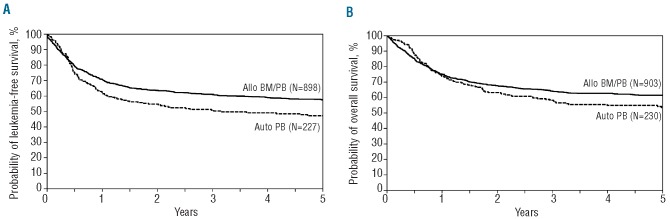
Probability of (A) leukemia-free survival for patients with acute myeloid leukemia in first complete remission by type of transplant; (B) overall survival for patients with acute myeloid leukemia in first complete remission by type of transplant. Allo: allogeneic; Auto: autologous; BM: bone marrow; PB: peripheral blood.
Leukemia recurrence and infection accounted for the majority of deaths. Patients in the autologous peripheral blood cohort were more likely to die of primary disease (67% compared to 35% for recipients of allogeneic peripheral blood and 37% for those grafted with allogeneic bone marrow).
Discussion
Despite the many prospective trials of post-remission treatment for acute myeloid leukemia in first complete remission, a definitive role for autologous transplantation remains uncertain and is now less frequently performed. Several systematic reviews suggest an advantage of matched sibling donor hematopoietic cell transplantation for patients in first complete remission with high risk and, possibly, intermediate risk acute myeloid leukemia at diagnosis.2 Earlier trials of allogeneic bone marrow versus autologous bone marrow transplantation showed advantages for the former with regard to leukemia-free survival.1
More recent studies have compared patients treated on the basis of whether they do or do not have a donor, which has the advantage of avoiding the bias of eliminating higher risk patients who relapse before assignment to autotransplantation or to consolidation chemotherapy. This approach generally shows a benefit from matched sibling donor allografting.2 The no-donor arms in such studies, however, combine patients treated with consolidation chemotherapy or autotransplantation, with the latter consisting entirely of autologous bone marrow recipients or with an unstated proportion of autologous peripheral blood recipients.2 In one major study, only 28% of the cases without a donor received autotransplants and the proportion of autologous peripheral blood transplants was not specified.15 Consequently, while treatment-related mortality in the “no-donor” arm was lower than that in the patients allografted from matched sibling donors, the treatment-related mortality due specifically to autologous peripheral blood transplants was uncertain. A recent, large prospective trial of autotransplantation versus consolidation chemotherapy (n=517) for patients with acute myeloid leukemia in first complete remission, conducted by the Dutch-Belgian Hemato-Oncology Cooperative Group (HOVON) and the Swiss Group for Clinical Cancer Research Collaborative Group (SAKK), demonstrated a low treatment-related mortality after peripheral blood autotransplantation (4%) and confirmed the lower relapse rate in patients treated with this strategy compared with consolidation chemotherapy (58% versus 70%, respectively; P=0.02).3
The comprehensive CIBMTR dataset enabled us to investigate several issues that were not addressed by published prospective trials. We are aware of the inherent limitations of studying registry databases, including potential unknown selection biases, incomplete reporting of cytogenetic analysis, the relatively long interval over which the transplants were performed and data collected and the lack of a non-transplant chemotherapy cohort. We attempted to address as many of these issues as possible. In this context, the HOVON/SAKK study provided a valuable control cohort treated only with consolidation chemotherapy, which was not available in our dataset.3
We found a significantly lower 5-year treatment-related mortality with autologous peripheral blood transplants than with allogeneic bone marrow/peripheral blood transplants, a finding confirmed by multivariate analysis (RR=0.37). While patients undergoing transplantation after 1999 had a significantly lower treatment-related mortality, likely related to improvements in supportive care, the 5-year transplant-related mortality rate for autologous peripheral blood recipients declined to 0% from 10% for years before 1999. However, relapse remained significantly higher following autologous peripheral blood transplantation than after allogeneic bone marrow or peripheral blood transplantation. As a result of these competing risks, the leukemia-free survival at 5 years was significantly inferior for patients undergoing autologous peripheral blood transplantation (RR 1.32, P=0.01), but only a marginal and non-significant difference in overall survival at 5 years was observed between patients treated with the two strategies (RR 1.23, P=0.07). For patients aged 40 years or younger, the 5-year leukemia-free and overall survival rates were the same following autologous peripheral blood and allogeneic bone marrow/peripheral blood transplants: 57% versus 60% and 62 versus 64%, respectively. Due to higher transplant-related mortality in patients >40 years, leukemia-free survival and overall survival in these older patients were significantly inferior not only with allotransplantation, but also with autologous peripheral blood transplants.
We also observed more frequent relapses after the more recent transplantations; the reasons for this are uncertain, but may be due to selection of lower risk patients for non-transplant therapies. Extramedullary disease was noted as an independent risk factor for higher relapse rate after either transplant approach.
Unexpectedly, cytogenetics did not affect outcomes in this study. Patient selection might again explain these results in part. Most patients had no cytogenetic abnormalities or favorable/intermediate risk cytogenetics and fewer than 10% had poor risk cytogenetics. One possible explanation for the low frequency of a high-risk cohort in the registry cases is initial treatment failure, prior to any consideration of transplantation. It is also possible that missing karyotype and modern molecular analysis for 12-26% of patients may have confounded the results, although outcomes for those with missing cytogenetics were not different from the outcomes for patients in other categories.
Autologous peripheral blood transplants were associated with a higher risk of relapse, as seen in most other studies, and the risk was even higher in patients over 40 years old.3,4,6,7,23 The HOVON/SAKK study of peripheral blood autotransplantation versus consolidation chemotherapy showed a relatively high relapse rate of 58%, albeit significantly better than after consolidation chemotherapy (70%).3 An EBMT study compared peripheral blood and bone marrow graft sources in patients undergoing autotransplantation for acute myeloid leukemia in complete remission24 and reported a higher relapse risk in recipients of autologous peripheral blood (bone marrow, 39% versus early peripheral blood, 56% versus late peripheral blood, 46%, P<0.001). Treatment-related mortality rates following peripheral blood or bone marrow autografts were similar (7-9%). Consequently, leukemia-free survival was inferior after peripheral blood transplants than after autologous bone marrow transplants. Following autologous peripheral blood cell transplantation, recipients with a higher CD34 cell dose had the highest risk of relapse.13,25 These findings suggest that peripheral blood grafts may include mobilized leukemic cells resulting in greater graft contamination. Information on the CD34+ cell dose was not available for many patients in our study, hence we were unable to study the effect of CD34+ cell dose on outcomes.
An important and still unanswered question is whether autologous transplantation should be routinely used or be further investigated for acute myeloid leukemia in first complete remission.25 Autotransplantation strategies were initially developed for patients lacking a matched sibling donor or for older patients considered unsuitable candidates for allogeneic transplantation. Over the last decade, safer allografts, suitable for older patients with acute myeloid leukemia, using reduced intensity conditioning,24-29 and broad use of well-matched unrelated donor transplants have yielded outcomes similar to those of matched sibling donor allogeneic bone marrow or allogeneic peripheral blood transplants for acute myeloid leukemia in remission.28,30,31 Therefore, only patients without a suitable allogeneic donor might be considered potential candidates for autotransplantation. Nonetheless, the favorable outcomes we report suggest that autologous peripheral blood transplantation should be studied again in well-designed prospective studies, especially in the context of post-transplant immunemediated cell therapy which may target clonogenic leukemic cells.32
Acknowledgments
Funding: The CIBMTR is supported by Public Health Service Grant/Cooperative Agreement 24-CA76518 from the National Cancer Institute (NCI), the National Heart, Lung and Blood Institute (NHLBI) and the National Institute of Allergy and Infectious Diseases (NIAID); a Grant/Cooperative Agreement 5U01HL069294 from the NHLBI and NCI; a contract HHSH234200637015C with Health Resources and Services Administration (HRSA/DHHS); two Grants N00014-06-1-0704 and N00014-08-1-0058 from the Office of Naval Research; and grants from Allos, Inc.; Amgen, Inc.; Angioblast; Anonymous donation to the Medical College of Wisconsin; Ariad; Be the Match Foundation; Blue Cross and Blue Shield Association; Buchanan Family Foundation; CaridianBCT; Celgene Corporation; CellGenix, GmbH; Children's Leukemia Research Association; Fresenius-Biotech North America, Inc.; Gamida Cell Teva Joint Venture Ltd.; Genentech, Inc.; Genzyme Corporation; GlaxoSmithKline; Kiadis Pharma; The Leukemia & Lymphoma Society; The Medical College of Wisconsin; Millennium Pharmaceuticals, Inc.; Milliman USA, Inc.; Miltenyi Biotec, Inc.; National Marrow Donor Program; Optum Healthcare Solutions, Inc.; Otsuka America Pharmaceutical, Inc.; Seattle Genetics; Sigma-Tau Pharmaceuticals; Soligenix, Inc.; Swedish Orphan Biovitrum; THERAKOS, Inc.; and Wellpoint, Inc.
Footnotes
Authorship and Disclosures: Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Gupta V, Tallman MS, Weisdorf DJ. Allogeneic hematopoietic cell transplantation for adults with acute myeloid leukemia: myths, controversies, and unknowns. Blood. 2011;117(8):2307-18 [DOI] [PubMed] [Google Scholar]
- 2.Reiffers J, Stoppa AM, Attal M, Michallet M, Marit G, Blaise D, et al. Allogeneic vs autologous stem cell transplantation vs chemotherapy in patients with acute myeloid leukemia in first remission: the BGMT 87 study. Leukemia. 1996;10(12):1874-82 [PubMed] [Google Scholar]
- 3.Keating S, de Witte T, Suciu S, Willemze R, Hayat M, Labar B, et al. The influence of HLA-matched sibling donor availability on treatment outcome for patients with AML: an analysis of the AML 8A study of the EORTC Leukaemia Cooperative Group and GIMEMA. European Organization for Research and Treatment of Cancer. Gruppo Italiano Malattie Ematologiche Maligne dell'Adulto. Br J Haematol. 1998;102(5):1344-53 [DOI] [PubMed] [Google Scholar]
- 4.Burnett AK, Wheatley K, Goldstone AH, Stevens RF, Hann IM, Rees JH, et al. The value of allogeneic bone marrow transplant in patients with acute myeloid leukaemia at differing risk of relapse: results of the UK MRC AML 10 trial. Br J Haematol. 2002;118(2):385-400 [DOI] [PubMed] [Google Scholar]
- 5.Suciu S, Mandelli F, de Witte T, Zittoun R, Gallo E, Labar B, et al. Allogeneic compared with autologous stem cell transplantation in the treatment of patients younger than 46 years with acute myeloid leukemia (AML) in first complete remission (CR1): an intention-to-treat analysis of the EORTC/GIMEMAAML-10 trial. Blood.2003;15;102(4):1232-40 [DOI] [PubMed] [Google Scholar]
- 6.Burnett AK, Goldstone AH, Stevens RM, Hann IM, Rees JK, Gray RG, et al. Randomised comparison of addition of autologous bone-marrow transplantation to intensive chemotherapy for acute myeloid leukaemia in first remission: results of MRC AML 10 trial. UK Medical Research Council Adult and Children's Leukaemia Working Parties. Lancet. 1998;351(9104):700-8 [DOI] [PubMed] [Google Scholar]
- 7.Mollee P, Gupta V, Song K, Reddy V, Califaretti N, Tsang R, et al. Long-term outcome after intensive therapy with etoposide, melphalan, total body irradiation and autotransplant for acute myeloid leukemia. Bone Marrow Transplant.2004;33(12):1201-8 [DOI] [PubMed] [Google Scholar]
- 8.Linker CA, Ries CA, Damon LE, Sayre P, Navarro W, Rugo HS, et al. Autologous stem cell transplantation for acute myeloid leukemia in first remission. Biol Blood Marrow Transplant. 2000;6(1):50-7 [DOI] [PubMed] [Google Scholar]
- 9.Linker CA, Ries CA, Damon LE, Rugo HS, Wolf JL. Autologous bone marrow transplantation for acute myeloid leukemia using 4-hydroperoxycyclophosphamide-purged bone marrow and the busulfan/etoposide preparative regimen: a follow-up report. Bone Marrow Transplant. 1998;22(9):865-72 [DOI] [PubMed] [Google Scholar]
- 10.Linker CA. Autologous stem cell transplantation for acute myeloid leukemia. Bone Marrow Transplant. 2003;31(9):731-8 [DOI] [PubMed] [Google Scholar]
- 11.Breems DA, Boogaerts MA, Dekker AW, Van Putten WL, Sonneveld P, Huijgens PC, et al. Autologous bone marrow transplantation as consolidation therapy in the treatment of adult patients under 60 years with acute myeloid leukaemia in first complete remission: a prospective randomized Dutch-Belgian Haemato-Oncology Co-operative Group (HOVON) and Swiss Group for Clinical Cancer Research (SAKK) trial. Br J Haematol. 2005;128(1):59-65 [DOI] [PubMed] [Google Scholar]
- 12.Gorin NC, Labopin M, Frassoni F, Milpied N, Attal M, Blaise D, et al. Identical outcome after autologous or allogeneic genoidentical hematopoietic stem-cell transplantation in first remission of acute myelocytic leukemia carrying inversion 16 or t(8;21): a retrospective study from the European Cooperative Group for Blood and Marrow Transplantation. J Clin Oncol. 2008;26(19):3183-8 [DOI] [PubMed] [Google Scholar]
- 13.Vellenga E, van Putten WL, Boogaerts MA, Daenen SM, Verhoef GE, Hagenbeek A, et al. Peripheral blood stem cell transplantation as an alternative to autologous marrow transplantation in the treatment of acute myeloid leukemia? Bone Marrow Transplant. 1999;23(12):1279-82 [DOI] [PubMed] [Google Scholar]
- 14.Kaplan EL, Meier P. Non parametric estimation from incomplete observations. J Am Stat Assoc. 1958;53:457-81 [Google Scholar]
- 15.Lin DY. Non-parametric inference for cumulative incidence functions in competing risks studies. Stat Med. 1997;16(8):901-10 [DOI] [PubMed] [Google Scholar]
- 16.Gooley TA, Leisenring W, Crowley J, Storer BE. Estimation of failure probabilities in the presence of competing risks: new representations of old estimators. Stat Med. 1999;18(6):695-706 [DOI] [PubMed] [Google Scholar]
- 17.Fine J, Gray R. A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc. 1999;94:496-509 [Google Scholar]
- 18.Klein J P, Logan B, Harhoff M, Andersen PK. Analyzing survival curves at a fixed point in time. Stat Med. 2007;26(24):4505-19 [DOI] [PubMed] [Google Scholar]
- 19.Klein J, Moeschberger M. Survival Analysis: Techniques of censored and truncated data. 2nd ed. New York, N.Y.: Springer-Verlag, 2003 [Google Scholar]
- 20.Cox DR. Regression models and life tables. J R Stat Soc. 1972;34:187-202 [Google Scholar]
- 21.Novitzky N, Thomas V, du Toit C, McDonald A. Is there a role for autologous stem cell transplantation for patients with acute myelogenous leukemia? A retrospective analysis. Biol Blood Marrow Transplant. 2011;17(6):875-84 [DOI] [PubMed] [Google Scholar]
- 22.Gorin NC, Labopin M, Blaise D, Reiffers J, Meloni G, Michallet M, et al. Higher incidence of relapse with peripheral blood rather than marrow as a source of stem cells in adults with acute myelocytic leukemia autografted during the first remission. J Clin Oncol. 2009;27(24):3987-93 [DOI] [PubMed] [Google Scholar]
- 23.Gorin NC, Labopin M, Reiffers J, Milpied N, Blaise D, Witz F, et al. Higher incidence of relapse in patients with acute myelocytic leukemia infused with higher doses of CD34+ cells from leukapheresis products autografted during the first remission. Blood. 2009;116(17):3157-62 [DOI] [PubMed] [Google Scholar]
- 24.McClune BL, Weisdorf DJ, Pedersen TL, Tunes da Silva G, Tallman MS, Sierra J, et al. Effect of age on outcome of reduced-intensity hematopoietic cell transplantation for older patients with acute myeloid leukemia in first complete remission or with myelodysplastic syndrome. J Clin Oncol. 2010;28(11):1878-87 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Gyurkocza B, Storb R, Storer BE, Chauncey TR, Lange T, Shizuru JA, et al. Nonmyeloablative allogeneic hematopoietic cell transplantation in patients with acute myeloid leukemia. J Clin Oncol. 2010;28(17):2859-67 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Koreth J, Aldridge J, Kim HT, Alyea E P, 3rd, Cutler C, Armand P, et al. Reduced-intensity conditioning hematopoietic stem cell transplantation in patients over 60 years: hematologic malignancy outcomes are not impaired in advanced age. Biol Blood Marrow Transplant. 2010;16(6):792-800 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Gupta V, Daly A, Lipton JH, Hasegawa W, Chun K, Kamel-Reid S, et al. Nonmyeloablative stem cell transplantation for myelodysplastic syndrome or acute myeloid leukemia in patients 60 years or older. Biol Blood Marrow Transplant. 2005;11(10):764-72 [DOI] [PubMed] [Google Scholar]
- 28.Bertz H, Potthoff K, Finke J. Allogeneic stem-cell transplantation from related and unrelated donors in older patients with myeloid leukemia. J Clin Oncol. 2003;15;21(8):1480-4 [DOI] [PubMed] [Google Scholar]
- 29.Deschler B, Binek K, Ihorst G, Marks R, Wasch R, Bertz H, et al. Prognostic factor and quality of life analysis in 160 patients aged > or =60 years with hematologic neoplasias treated with allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant 2010;16(7):967-75 [DOI] [PubMed] [Google Scholar]
- 30.Gupta V, Tallman MS, He W, Logan BR, Copelan E, Gale RP, et al. Comparable survival after HLA-well-matched unrelated or matched sibling donor transplantation for acute myeloid leukemia in first remission with unfavorable cytogenetics at diagnosis. Blood. 2010;116(11):1839-48 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Walter RB, Pagel JM, Gooley TA, Petersdorf EW, Sorror ML, Woolfrey AE, et al. Comparison of matched unrelated and matched related donor myeloablative hematopoietic cell transplantation for adults with acute myeloid leukemia in first remission. Leukemia. 2010;24(7):1276-82 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Williams BA, Wang XH, Keating A. Clonogenic assays measure leukemia stem cell killing not detectable by chromium release and flow cytometric cytotoxicity assays. Cytotherapy. 2010;12(7):951-60 [DOI] [PubMed] [Google Scholar]