

Abstract
Objectives
The age of adolescents at first sexual intercourse is an important risk factor for sexually transmitted diseases (STDs) and adolescent pregnancy. Black adolescents are at higher risk than white adolescents for first sexual intercourse at younger ages as well as STDs and pregnancy. Individual- and family-level factors do not fully explain this disparity. We examined whether five dimensions of black-white residential racial segregation can help explain the racial disparity in age at first sexual intercourse.
Methods
Using the National Longitudinal Survey of Youth 1997 and U.S. Census 2000 data, we performed multiple hierarchical discrete time-to-event analyses on a nationally representative cohort of adolescents followed since 1997. Although the cohort study is ongoing, we used data from 1997 through 2005.
Results
Concentration and unevenness significantly modified the association of race and age at first sexual intercourse. However, stratified results suggested differences in the effect of race on age at first sexual intercourse at each level of segregation across dimensions of segregation.
Conclusions
Residential racial segregation may modify the black-white disparity in risk of first sexual intercourse at younger ages, but these associations are complex. Future studies should be conducted to elucidate the causal mechanisms.
In the United States, the age of adolescents at first sexual intercourse has been shown to be a risk factor for other sexual risk behaviors, even long term,1–3 as well as for sexually transmitted disease (STD) acquisition and adolescent pregnancy.2,4 Adolescents continue to have the highest rates of STDs in the U.S., and adolescent pregnancy rates remain higher in the U.S. than in other industrialized countries.5,6
Black adolescents are more likely than white adolescents to report first sexual intercourse at younger ages.7 Similarly, compared with white adolescents, black adolescents have higher rates of most STDs8 as well as higher rates of adolescent pregnancies and births.6 Studies of individual- and family-level predictors of adolescent age at first sexual intercourse have not fully explained the racial disparities.9 Individual-level interventions aimed at delaying sexual intercourse have not been as successful as interventions to reduce other risky sexual behaviors, such as unprotected sex.10 Examining characteristics of the social environment can contextualize behavior and help explain what puts individuals at differential risk. The social environment likely influences individual sexual risk by shaping risk behaviors and social and sexual network patterns.11–14
Residential racial segregation (hereafter, segregation)—i.e., the spatial distribution of one racial group relative to another—continues to characterize many metropolitan areas (MAs) in the U.S., and black people continue to experience segregation more than any other racial group.15–18 Segregation is defined by five distinct dimensions—isolation, concentration, centralization, clustering, and unevenness.15–17 Isolation of the black population from other racial groups, or the probability that black people share neighborhoods with other black people rather than white people, may strengthen within-group social norms. Concentration of the black population, or the density of black people in each neighborhood, further concentrates social, economic, and political disadvantage. Centralization of the black population, or the extent to which black neighborhoods are located around the center of the MA, limits this group to urban centers, which in the U.S. are largely characterized by crowding and poverty. Clustering of the black population, or the degree to which black neighborhoods are contiguous within the MA, may exacerbate the concentration of social problems. Finally, unevenness of the black population, or the extent to which the proportion of black people in each neighborhood differs from the proportion of black people in the MA as a whole, can result in further social isolation.15,16,18–20 These characteristics are associated with multiple risk behaviors, including sexual risk behaviors.1,18,19,21–26
Segregation is posited to be a fundamental cause of racial disparities in sexual risk.19,27 While studies have found that living in more segregated areas is associated with poorer health outcomes,20,22,23,28–31 limited studies have examined the association between segregation and health behaviors.32–34 To the best of our knowledge, only two studies have empirically examined the association between segregation and sexual health outcomes. First, using national surveillance data, our research group found that certain dimensions of segregation were associated with gonorrhea rates among black people in the U.S.35 Second, we found that among adolescents and young adults, hypersegregation was not associated with a sexual risk index, which included measures of sexual activity, condom use, and number of partners.36 In this article, we assessed whether black-white segregation can help explain the black-white racial disparity in adolescent age at first sexual intercourse, beyond individual- and family-level characteristics, in a nationally representative cohort of adolescents in the U.S.
METHODS
Person-level data
Data on person-level measures came from the National Longitudinal Survey of Youth 1997 (NLSY97). Briefly, NLSY97 is a longitudinal survey of 8,984 young people who were 12–16 years of age on December 31, 1996. Participants were interviewed on a yearly basis with baseline interviews completed in 1997–1998. Nine rounds of data were used for this analysis (1997–2005) to ensure follow-up of participants through age 20 years (i.e., adolescence). Retention rates were greater than 80%.37
Based on our study objectives, the sample was limited to non-Hispanic black and non-Hispanic white participants (n=6,746 in 121 MAs). We further limited the sample to those living in U.S. Census-defined MAs (n=5,176 in 120 MAs), as segregation is an MA characteristic. Furthermore, to remove unstable segregation estimates,15,28 the sample was limited to those living in MAs with a total population >100,000 and a black population >5,000 (n=4,794 individuals in 110 MAs). Participants who had no valid responses about ever having sex (n=27) or who reported having sex but did not report an age at first sexual intercourse (n=277) were excluded. Research suggests that only a very small number of individuals have their first, non-coerced, sexual intercourse before age 12 years.38 Therefore, we excluded those who reported having sex before age 12 (n=167). Individuals living in MAs where three or fewer individuals were represented were excluded (n=12 individuals in five MAs). The final sample comprised 4,311 individuals in 105 MAs, with a mean of 41.06 individuals per MA (range: 4.00 to 175.00).
Outcome measure: age at first sexual intercourse.
Age at first sexual intercourse was determined by participants' response to the following question: “Thinking about the very first time in your life that you had sexual intercourse with a person of the opposite sex, how old were you?” Adolescent sexual intercourse was defined as the participant being 20 years of age or younger at first sexual intercourse. Our sample had data on age at first sexual intercourse for 3,900 individuals.
Primary person-level exposure: race/ethnicity.
Race and ethnicity were self-reported and categorized into non-Hispanic white or non-Hispanic black race/ethnicity.
Person-level baseline covariates.
Person-level covariates were assessed at baseline and included individual, family, and geographic attributes hypothesized to be important predictors of adolescent first sexual intercourse.
Individual.
Age at baseline and sex of participant were included.
Family.
Socioeconomic status was assessed using four measures: gross household income in the last year, maternal education, paternal education (<high school vs. ≥high school for both), and number of rooms per person in the household. Family structure was assessed using three measures: whether the participant lived in a home with both biological parents at age 2 years, whether the participant lived in a single-parent home at baseline, and the number of children who lived with the participant at baseline (≤2 vs. >2 children).
Geographic.
Based on participants' addresses, we determined whether they lived in a Census-defined urban area and in what part of the MA they resided. Census region of residence was also determined.
We included in all analyses variables indicating whether the participant was part of the NLSY97 oversample of black and Hispanic participants and whether age at first sex was retrospectively reported at baseline.
Metropolitan area-level data
Data on all MA-level measures were obtained from the U.S. Census Bureau.
Primary MA-level exposure: residential racial segregation.
Segregation is operationalized by assessing the distribution of black residents across neighborhoods (e.g., census tracts) within larger MAs (e.g., Census-defined metropolitan statistical areas). Five dimensions of segregation—exposure, concentration, centralization, clustering, and unevenness—represent distinct components of segregation.39 Each dimension of segregation may have varying degrees of salience in describing distinct mechanisms.20 As these specific mechanisms have, to date, been unexplored, we examined indices of each dimension as well as a summary measure, hypersegregation.
These dimensions have been described in a previous section of this article, and the indices are described in detail elsewhere.15–17,39 Isolation was operationalized using the isolation index (range: 0.0 to 1.0). Concentration and centralization were measured using the relative concentration index (range: –1.0 to 1.0) and absolute centralization index (range: –1.0 to 1.0), respectively. Clustering was measured using the spatial proximity index. While this index can be any real value, in practice it ranges from 1.0 to 2.0. We subtracted 1.0 to put it on the same scale as the other indices. Finally, unevenness was measured by the dissimilarity index (range: 0.0 to 1.0).15 For all indices, higher values indicate higher segregation of black people from white people.
Values for segregation indices were obtained from the U.S. Census Bureau Housing and Household Economic Statistics Division, which used U.S. Census 2000 data and 1999 MA definitions to calculate these indices. Segregation indices were categorized at values established previously by segregation demographers: very low (≤0.30), low (>0.30–0.40), moderate (>0.40–0.60), and high (>0.60).29,32,40 MAs that were highly segregated on four or five dimensions were categorized as hypersegregated.17,28
MA-level covariates.
MA-level sociodemographic measures were obtained from the U.S. Census Bureau's 2000 Census Summary 1 and 3 files. Population size (log), population density (people per square mile), and racial composition (proportion black) were included.41 Krieger's socioeconomic position index was used to measure MA-level socioeconomic status, incorporating multiple area-level measures (e.g., percentage unemployed and percentage in poverty).42 Higher scores represent lower socioeconomic position.
Statistical analysis
MA of residence of participants at baseline was reported by NLSY97 and defined according to 1999 U.S. Census demarcations of metropolitan statistical areas. MA-level data and person-level survey data were then linked based on these MAs.
Several person-level covariates had missing data: gross household income (26.0%), paternal education (19.7%), biological parents in the home (11.6%), maternal education (7.0%), rooms per people in home (1.7%), and single-parent household (0.2%). We performed multiple imputations using an iterative Markov Chain Monte Carlo procedure, which incorporates uncertainty due to missing data in calculating parameter estimates and standard errors.43
Age at first sexual intercourse was collected as an integer value with nine possible responses (ages 12–20 years). Therefore, discrete time-to-event analysis with a logit function was performed. Hazard rates of adolescent first sexual intercourse were modeled, and hazard odds ratios (HORs) and 95% confidence intervals (CIs) are reported.
We created two-level hierarchical models to account for dependence of individuals within MAs. First, we created an unconditional random intercept model with the age indicator variables to account for the heterogeneity in ages of adolescents at first sexual intercourse across MAs. Because we were examining racial disparities, we added race and specified a random intercept and slope (for race) model with an unstructured covariance.28,29 After including covariates, we tested a main effect of segregation for each dimension separately. As the test of the primary research question, to examine whether the black-white disparity in age at adolescent first sexual intercourse varied in areas with different levels of segregation, we included race-by-segregation interaction terms. F-tests were used to test statistical significance for all models.
We performed estimation with maximum likelihood using adaptive Gaussian quadrature. All analyses were conducted using Stata® release 11.44
RESULTS
Sample characteristics
Baseline characteristics are described in Table 1. Briefly, compared with white respondents, black respondents were more socioeconomically disadvantaged and more likely to live in a single-parent household at baseline. Of the 105 MAs included in this analysis, 23.8% were highly isolated, 60.9% were highly concentrated, 72.4% were highly centralized, 4.8% were highly clustered, 43.8% were highly uneven, and 16.2% were hypersegregated.
Table 1.
NLSY 1997 and metropolitan area sample characteristics in a study on residential racial segregation and the black-white disparity among adolescents in age at first sexual intercoursea
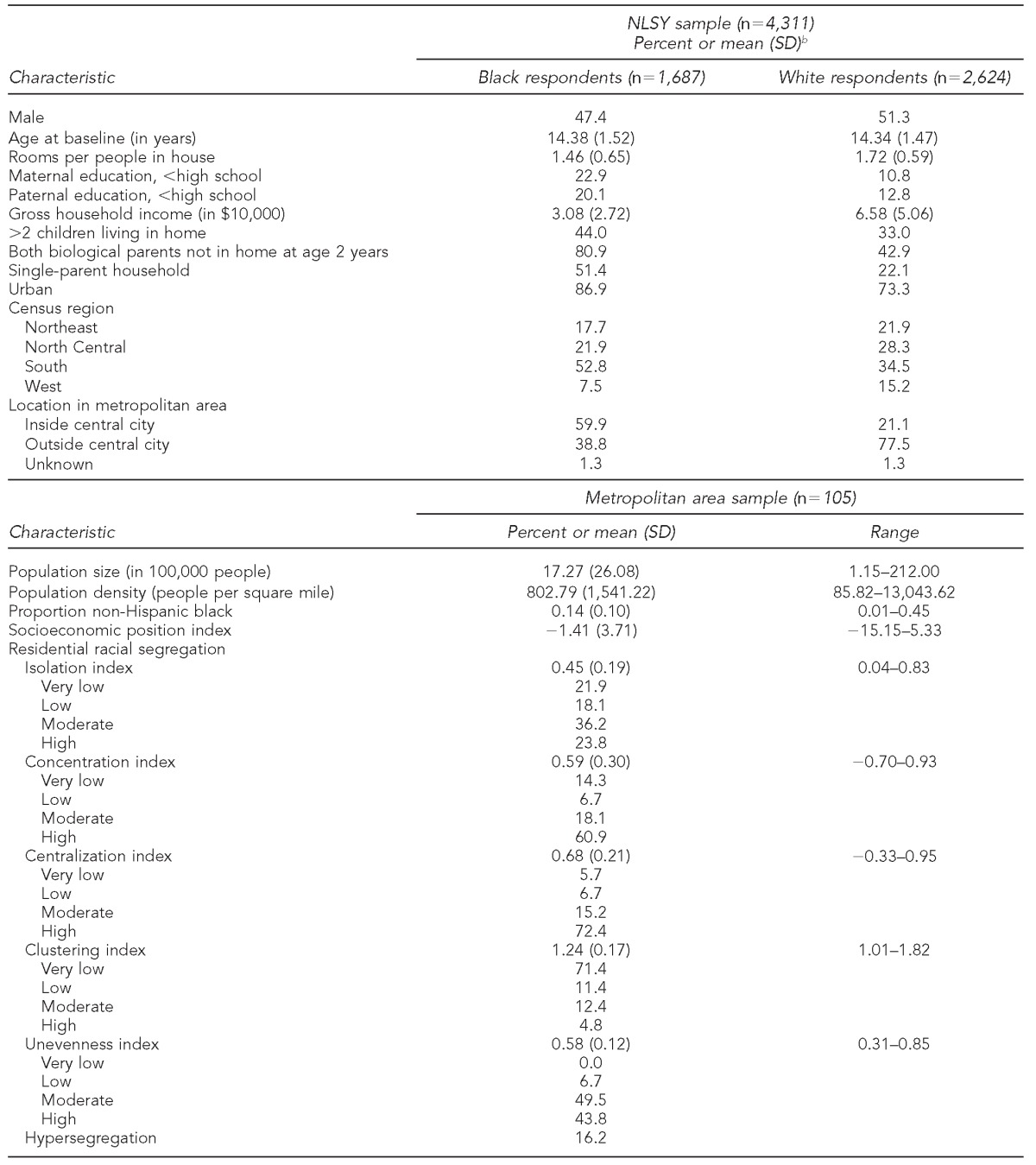
aBased on NLSY 1997 (1997–2005) and U.S. Census 2000 data. Note: Sampling weights were not used, so these data should not be interpreted as representing national characteristics.
bProportions and means were calculated on pre-imputed data.
NLSY = National Longitudinal Survey of Youth
SD = standard deviation
Race, segregation, and adolescent first sexual intercourse
Among black participants, 91.5% reported having first sexual intercourse in adolescence, compared with 85.6% of white participants. Among those who had their first sexual intercourse in adolescence, the mean age of first sexual intercourse for black participants was 15.26 years of age (standard deviation [SD] = 1.84), compared with a mean of 16.15 years of age (SD=1.84) for white participants (data not shown).
The likelihood of having first sexual intercourse in adolescence increased through age 18 years and then decreased from age 18 to age 20 years, and black participants had a higher likelihood of first sexual intercourse in adolescence than white respondents (p<0.0001) (Figure). After allowing the association between race and age at first sexual intercourse to vary randomly across MAs and adjusting for control variables, black participants were 1.56 times as likely as white participants to have had their first sexual intercourse in adolescence (95% CI 1.37, 1.77). After additionally adjusting for individual covariates, this racial disparity remained. Inclusion of family and then additionally geographic covariates reduced the disparity substantially (HOR=1.15, 95% CI 1.00, 1.33). However, the disparity still remained. Inclusion of MA-level covariates did not further reduce the racial disparity in the odds of having first sexual intercourse in adolescence (Table 2).
Figure.
Estimated log-hazard odds of adolescent first sexual intercourse, overall and by race, in a study on residential racial segregation and the black-white disparity among adolescents in age at first sexual intercoursea
aBased on National Longitudinal Survey of Youth 1997 (1995–2005)

Table 2.
Hazard odds of adolescent first sexual intercourse in multiple hierarchical discrete time-to-event models: National Longitudinal Survey of Youth 1997 (1997–2005)
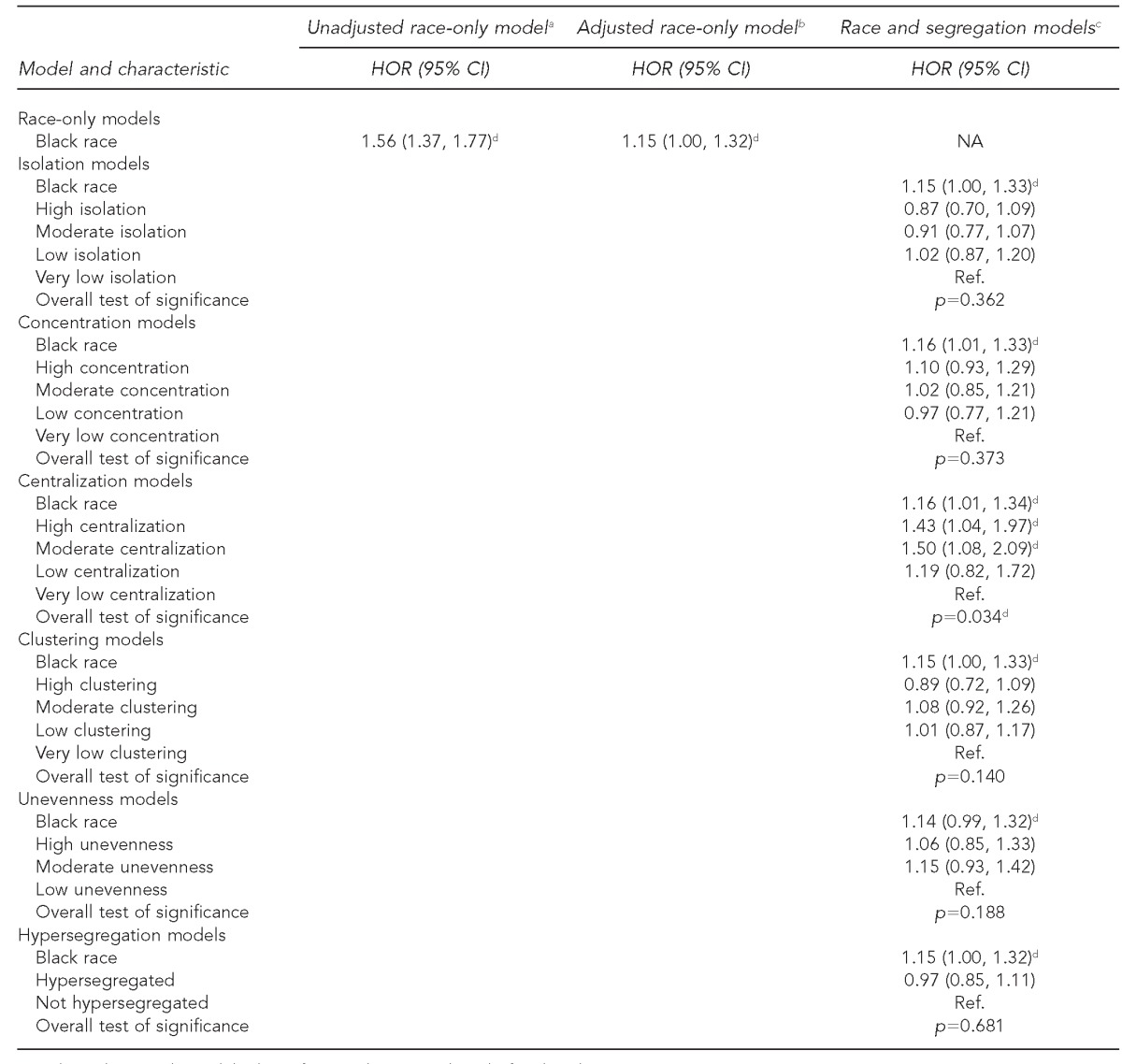
aUnadjusted race-only model adjusts for sample type and sex before baseline interview.
bAdjusted race-only model includes all covariates (adjusted), but does not include segregation measures.
cRace and segregation models include all covariates (adjusted).
dStatistically significant at p≤0.05
HOR = hazard odds ratio
CI = confidence interval
NA = not applicable
Ref. = reference category
Only centralization was significantly associated with adolescent first sexual intercourse (p=0.034); living in areas with high and moderate centralization increased the odds of adolescent first sexual intercourse by approximately 50% compared with living in areas with very low centralization (Table 2).
Concentration (p=0.016 for interaction) modified the race-adolescent first sexual intercourse association significantly, and unevenness (p=0.052 for interaction) and hypersegregation (p=0.060 for interaction) were borderline significant. While race-segregation interaction terms were not significant for isolation, centralization, and clustering, stratified results suggested potential differences in the association between race and adolescent first sexual intercourse at each level of segregation across these dimensions of segregation (Table 3).
Table 3.
Hazard odds of adolescent first sexual intercourse of black compared with white adolescents, by segregation, in multiple hierarchical discrete time-to-event models: National Longitudinal Survey of Youth 1997 (1997–2005)a

aRace X segregation models include all covariates (adjusted).
bHypersegregation categories are hypersegregated and not hypersegregated.
cStatistically significant at p≤0.05
HOR = hazard odds ratio
CI = confidence interval
NA = not applicable
As hypothesized, across all dimensions in highly segregated MAs, black participants were 1.20 to 1.40 times as likely to have had adolescent first sexual intercourse compared with white participants (Table 3). For concentration, centralization, and clustering, this racial disparity was not seen in areas characterized by low or very low segregation. Similarly, in hypersegregated areas, black participants were at increased odds of adolescent first sexual intercourse compared with white participants, whereas no racial disparity was seen in non-hypersegregated areas. In contrast, however, according to the isolation and unevenness dimensions, black participants were 1.56 and 1.52 times as likely as white participants to have had adolescent first sexual intercourse in areas characterized by very low and low isolation and unevenness, respectively (Table 3).
DISCUSSION
Age at first sexual intercourse in adolescence is an important predictor of STD infection and adolescent pregnancy,2,4 and black-white disparities exist in each of these health outcomes.6–8 The results of our study support previous findings9 that there is indeed a black-white disparity in age of adolescent first sexual intercourse and that this disparity is not fully explained by individual characteristics. Our study indicates that residential racial segregation may help to explain this disparity. However, these associations are complex.
According to the concentration, centralization, and clustering indices, in areas with the highest levels of segregation, black participants had increased odds compared with white participants of having first sexual intercourse in adolescence, whereas in areas with the lowest levels of segregation, this racial disparity did not exist. High concentration of black people may be associated with increased likelihood of adolescent first sexual intercourse because racial concentration further concentrates inherited economic, political, and social disadvantage.18–20 Studies have found that concentrated poverty is associated with increased odds of adolescent first sexual intercourse.9,45 Similarly, high centralization indicates that black people live closer to the center of the MA and, therefore, may experience the attributes that characterize many of these urban cities in the U.S., including a poorer neighborhood environment. A poor neighborhood environment is believed to increase social disorder and foster crime, drug use, and risky sexual behaviors.18,19,21,40,46 Studies have shown that segregation is associated with increased crime rates and drug use.33,40,47 High clustering may exacerbate the effects of the concentrated disadvantage and social disorder in these areas.
According to the isolation and unevenness measures, the racial disparity existed in areas with the lowest and highest levels of segregation, yet the racial disparity did not exist in areas with moderate levels of segregation. Bell et al. described this U-shaped association when examining the association between segregation and smoking among black people.32 Measures of isolation and unevenness, while distinct, are conceptually and empirically correlated,48 indicating consistency in these findings. If an area is highly uneven, the black population is not distributed evenly across neighborhoods in an MA and is living in separate neighborhoods and in neighborhoods with a high percentage of black people, resulting in black people being isolated from white people. In areas characterized by low values of isolation and unevenness indices, segregation may appear low; however, if the black population is relatively small in these MAs, true integration may not exist.48 In fact, under these conditions, black people may experience more racism,49 in turn increasing health risks for black adolescents in these areas. Studies have found that experiencing racial discrimination is associated with increased risk behaviors in adolescents.46,50,51 On the other hand, a moderate level of isolation may in fact be protective for black people, potentially by fostering social support and political power within the black communities.52
In hypersegregated areas, black participants were at increased odds of adolescent first sexual intercourse compared with white people. This racial disparity did not exist in non-hypersegregated areas. Conceptually, the disadvantageous effects of high segregation are multiplied in areas characterized by high segregation across multiple dimensions.16,41 Therefore, this finding is not surprising given the association between race and first sexual intercourse in highly segregated areas across the dimensions.
Strengths and limitations
These findings should be interpreted in light of the study limitations. The person-level data were self-reported and may be subject to misclassification error. Computer-assisted personal interviews were used to collect data on sex to reduce bias. Some individual-level variables had substantial missing values, and multiple imputations may not have reduced bias. Because survey questions related to sexual intercourse referred to sex with a person of the opposite sex, sexual intercourse with a same-sex partner was impossible to determine. Using baseline place of residence to determine segregation status may have introduced misclassification if it was not the place where respondents lived at the most relevant time frame for first sexual intercourse. Using the baseline place of residence is supported in neighborhood effects research.9,53,54 Nonetheless, future studies may consider an appropriate lag time between exposure to segregation and the outcome.49,52 Due to the original survey sampling and our exclusion criteria, our sample may not be representative of all MAs in the U.S.
Despite these limitations, this study is the first to empirically examine the role of segregation in racial disparities in adolescent first sexual intercourse—an important predictor of STD infection and adolescent pregnancy—using a valid multilevel framework. Our study used national longitudinal survey data and, therefore, we were able to examine the effect of segregation on sexual risk over the course of adolescence, an important contribution to a field that has focused mainly on adult and birth outcomes.49
CONCLUSIONS
Black adolescents continue to have higher rates of most STDs8 and higher rates of adolescent pregnancies and births compared with other racial/ethnic groups.6 Studies of individual- and family-level predictors of sexual health outcomes have not fully explained the racial disparities, and individual-level interventions have not been effective at reducing these disparities. Importantly, growing evidence suggests that, although complex, residential racial segregation—a characteristic of the environment that has shaped and continues to shape the urban environment in the U.S.55—may influence sexual health for black adolescents. Future studies should aim to further explore the causal mechanisms and additional moderators for these associations.
Footnotes
This study was supported by the National Institute of Mental Health (NIMH) at the National Institutes of Health (NIH) (T32MH020031 and P30MH062294 to Yale University). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIMH or the NIH. This study was approved by the Yale University Institutional Review Board.
REFERENCES
- 1.O'Donnell BL, O'Donnell CR, Stueve A. Early sexual initiation and subsequent sex-related risks among urban minority youth: the Reach for Health Study. Fam Plann Perspect. 2001;33:268–75. [PubMed] [Google Scholar]
- 2.Coker AL, Richter DL, Valois RF, McKeown RE, Garrison CZ, Vincent ML. Correlates and consequences of early initiation of sexual intercourse. J Sch Health. 1994;64:372–7. doi: 10.1111/j.1746-1561.1994.tb06208.x. [DOI] [PubMed] [Google Scholar]
- 3.Sandfort TG, Orr M, Hirsch JS, Santelli J. Long-term health correlates of timing of sexual debut: results from a national US study. Am J Public Health. 2008;98:155–61. doi: 10.2105/AJPH.2006.097444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kaestle CE, Halpern CT, Miller WC, Ford CA. Young age at first sexual intercourse and sexually transmitted infections in adolescents and young adults. Am J Epidemiol. 2005;161:774–80. doi: 10.1093/aje/kwi095. [DOI] [PubMed] [Google Scholar]
- 5.Centers for Disease Control and Prevention (US), National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, Division of STD Prevention. Sexually transmitted disease morbidity for selected STDs by age, gender, and race/ethnicity, United States and Puerto Rico, 1996-2008. [cited 2012 Jan 10]. Available from: URL: http://wonder.cdc.gov/wonder/help/std-2008-race-age.html.
- 6.Ventura SJ, Mathews TJ, Hamilton BE, Sutton PD, Abma JC. Adolescent pregnancy and childbirth—United States, 1991-2008. MMWR Surveill Summ. 2011;60(Suppl):105–8. [PubMed] [Google Scholar]
- 7.Hallfors DD, Iritani BJ, Miller WC, Bauer DJ. Sexual and drug behavior patterns and HIV and STD racial disparities: the need for new directions. Am J Public Health. 2007;97:125–32. doi: 10.2105/AJPH.2005.075747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Centers for Disease Control and Prevention (US). Sexually transmitted disease surveillance, 2009. Atlanta: CDC; 2010. [cited 2012 Jan 10]. Also available from: URL: http://www.cdc.gov/std/stats09/toc.htm. [Google Scholar]
- 9.Browning C, Leventhal T, Brooks-Gunn J. Neighborhood context and racial differences in early adolescent sexual activity. Demography. 2004;41:697–720. doi: 10.1353/dem.2004.0029. [DOI] [PubMed] [Google Scholar]
- 10.Ethier KA, Orr DP. Behavioral interventions for prevention and control of STDs among adolescents. In: Aral SO, Douglas JM Jr, editors. Behavioral interventions for prevention and control of sexually transmitted diseases. New York: Springer Science+Business Media LLC; 2007. pp. 277–309. [Google Scholar]
- 11.Adimora AA, Schoenbach VJ, Bonas DM, Martinson FE, Donaldson KH, Stancil TR. Concurrent sexual partnerships among women in the United States. Epidemiology. 2002;13:320–7. doi: 10.1097/00001648-200205000-00013. [DOI] [PubMed] [Google Scholar]
- 12.Leichliter JS, Aral SO. Black women in the United States decrease their number of recent sex partners: temporal trends from the National Survey of Family Growth. Sex Transm Dis. 2009;36:1–3. doi: 10.1097/OLQ.0b013e3181845b84. [DOI] [PubMed] [Google Scholar]
- 13.Leichliter JS, Chesson HW, Sternberg M, Aral SO. The concentration of sexual behaviours in the USA: a closer examination of subpopulations. Sex Transm Infect. 2010;86(Suppl 3):iii45–51. doi: 10.1136/sti.2010.042283. [DOI] [PubMed] [Google Scholar]
- 14.Aral SO, Adimora AA, Fenton KA. Understanding and responding to disparities in HIV and other sexually transmitted infections in African Americans. Lancet. 2008;372:337–40. doi: 10.1016/S0140-6736(08)61118-6. [DOI] [PubMed] [Google Scholar]
- 15.Iceland J, Weinberg DH, Steinmetz E. U.S. Census Bureau, series CENSR-3, racial and ethnic residential segregation in the United States: 1980-2000. Washington: Government Printing Office (US); 2002. [Google Scholar]
- 16.Massey D, Denton NA. Hypersegregation in U.S. metropolitan areas: black and Hispanic segregation along five dimensions. Demography. 1989;26:373–91. [PubMed] [Google Scholar]
- 17.Massey DS, White MJ, Phua V-C. The dimensions of segregation revisited. Sociol Methods Res. 1996;25:172–206. [Google Scholar]
- 18.Williams DR, Collins C. Racial residential segregation: a fundamental cause of racial disparities in health. Public Health Rep. 2001;116:404–16. doi: 10.1093/phr/116.5.404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hogben M, Leichliter JS. Social determinants and sexually transmitted disease disparities. Sex Transm Dis. 2008;35(12 Suppl):S13–8. doi: 10.1097/OLQ.0b013e31818d3cad. [DOI] [PubMed] [Google Scholar]
- 20.Poundstone KE, Strathdee SA, Celentano DD. The social epidemiology of human immunodeficiency virus/acquired immunodeficiency syndrome. Epidemiol Rev. 2004;26:22–35. doi: 10.1093/epirev/mxh005. [DOI] [PubMed] [Google Scholar]
- 21.Acevedo-Garcia D, Lochner KA, Osypuk TL, Subramanian SV. Future directions in residential segregation and health research: a multilevel approach. Am J Public Health. 2003;93:215–21. doi: 10.2105/ajph.93.2.215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Massey DS. Segregation and violent crime in urban America. In: Anderson E, Massey DS, editors. Problem of the century: racial stratification in the United States. New York: Russell Sage Foundation; 2001. pp. 317–44. [Google Scholar]
- 23.Acevedo-Garcia D. Residential segregation and the epidemiology of infectious diseases. Soc Sci Med. 2000;51:1143–61. doi: 10.1016/s0277-9536(00)00016-2. [DOI] [PubMed] [Google Scholar]
- 24.Bell JF, Zimmerman FJ, Almgren GR, Mayer JD, Huebner CE. Birth outcomes among urban African-American women: a multilevel analysis of the role of racial residential segregation. Soc Sci Med. 2006;63:3030–45. doi: 10.1016/j.socscimed.2006.08.011. [DOI] [PubMed] [Google Scholar]
- 25.Albarracin D, Kumkale G, Johnson BT. Influences of social power and normative support on condom use decisions: a research synthesis. AIDS Care. 2004;16:700–23. doi: 10.1080/09540120412331269558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Carvajal SC, Parcel GS, Banspach SW, Basen-Engquist K, Coyle KK, Kirby D, et al. Psychosocial predictors of delay of first sexual intercourse by adolescents. Health Psychol. 1999;18:443–52. doi: 10.1037//0278-6133.18.5.443. [DOI] [PubMed] [Google Scholar]
- 27.El-Bassel N, Caldeira NA, Ruglass LM, Gilbert L. Addressing the unique needs of African American women in HIV prevention. Am J Public Health. 2009;99:996–1001. doi: 10.2105/AJPH.2008.140541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Osypuk TL, Acevedo-Garcia D. Are racial disparities in preterm birth larger in hypersegregated areas? Am J Epidemiol. 2008;167:1295–304. doi: 10.1093/aje/kwn043. [DOI] [PubMed] [Google Scholar]
- 29.Subramanian SV, Acevedo-Garcia D, Osypuk TL. Racial residential segregation and geographic heterogeneity in black/white disparity in poor self-rated health in the US: a multilevel statistical analysis. Soc Sci Med. 2005;60:1667–79. doi: 10.1016/j.socscimed.2004.08.040. [DOI] [PubMed] [Google Scholar]
- 30.Acevedo-Garcia D. Zip Code-level risk factors for tuberculosis: neighborhood environment and residential segregation in New Jersey, 1985-1992. Am J Public Health. 2001;91:734–41. doi: 10.2105/ajph.91.5.734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Grady SC. Racial disparities in low birthweight and the contribution of residential segregation: a multilevel analysis. Soc Sci Med. 2006;63:3013–29. doi: 10.1016/j.socscimed.2006.08.017. [DOI] [PubMed] [Google Scholar]
- 32.Bell JF, Zimmerman FJ, Mayer JD, Almgren GR, Huebner CE. Associations between residential segregation and smoking during pregnancy among urban African-American women. J Urban Health. 2007;84:372–88. doi: 10.1007/s11524-006-9152-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Cooper HL, Friedman SR, Tempalski B, Friedman R. Residential segregation and injection drug use prevalence among black adults in US metropolitan areas. Am J Public Health. 2007;97:344–52. doi: 10.2105/AJPH.2005.074542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Lopez R. Black-white residential segregation and physical activity. Ethn Dis. 2006;16:495–502. [PubMed] [Google Scholar]
- 35.Biello KB, Kershaw T, Nelson R, Hogben M, Ickovics J, Niccolai L. Residential racial segregation and rates of gonorrhea in the United States, 2003-2007. Am J Public Health. 2012;102:1370–7. doi: 10.2105/AJPH.2011.300516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Biello KB, Niccolai L, Kershaw TS, Lin H, Ickovics J. Residential racial segregation and racial differences in sexual behaviours: an 11-year longitudinal study of sexual risk of adolescents transitioning to adulthood. J Epidemiol Community Health. 2012 Jul 3; doi: 10.1136/jech-2011-200520. Epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.The Ohio State University, Center for Human Resource Research. Prepared for the U.S. Department of Labor. Columbus (OH): The Ohio State University, Center for Human Resource Research; 2003. NLSY97 user's guide: a guide to the rounds 1-5 data, National Longitudinal Survey of Youth 1997. [Google Scholar]
- 38.Cavazos-Rehg PA, Krauss MJ, Spitznagel EL, Schootman M, Bucholz KK, Peipert JF, et al. Age of sexual debut among US adolescents. Contraception. 2009;80:158–62. doi: 10.1016/j.contraception.2009.02.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Massey DS, Denton NA. The dimensions of residential segregation. Social Forces. 1988;67:281–315. [Google Scholar]
- 40.Feldmeyer B. The effects of racial/ethnic segregation on Latino and black homicide. Sociol Q. 2010;51:600–23. doi: 10.1111/j.1533-8525.2010.01185.x. [DOI] [PubMed] [Google Scholar]
- 41.Wilkes R, Iceland J. Hypersegregation in the twenty-first century. Demography. 2004;41:23–36. doi: 10.1353/dem.2004.0009. [DOI] [PubMed] [Google Scholar]
- 42.Krieger N, Chen J, Waterman P, Rehkopf DH, Subramanian SV. Race/ethnicity, gender, and monitoring socioeconomic gradients in health: a comparison of area-based socioeconomic measures—the Public Health Disparities Geocoding Project. Am J Public Health. 2003;93:1655–71. doi: 10.2105/ajph.93.10.1655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Little RJA, Rubin DB. Statistical analysis with missing data. 2nd ed. Hoboken (NJ): John Wiley & Sons, Inc.; 2002. [Google Scholar]
- 44.StataCorp LP. Stata®: Release 11. College Station (TX): StataCorp LP; 2009. [Google Scholar]
- 45.Cubbin C, Santelli J, Brindis C, Braveman P. Neighborhood context and sexual behaviors among adolescents: findings from the National Longitudinal Study of Adolescent Health. Perspect Sex Reprod Health. 2005;37:125–34. doi: 10.1363/psrh.37.125.05. [DOI] [PubMed] [Google Scholar]
- 46.Copeland-Linder N, Lambert SF, Chen YF, Ialongo NS. Contextual stress and health risk behaviors among African American adolescents. J Youth Adolesc. 2011;40:158–73. doi: 10.1007/s10964-010-9520-y. [DOI] [PubMed] [Google Scholar]
- 47.Shihadeh ES, Maume MO. Segregation and crime. Homicide Studies. 1997;1:254–80. [Google Scholar]
- 48.Massey DS, Denton NA. American apartheid: segregation and the making of the underclass. Cambridge (MA): Harvard University Press; 1993. [Google Scholar]
- 49.White K, Borrell LN. Racial/ethnic residential segregation: framing the context of health risk and health disparities. Health Place. 2011;17:438–48. doi: 10.1016/j.healthplace.2010.12.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Pachter LM, Coll CG. Racism and child health: a review of the literature and future directions. J Dev Behav Pediatr. 2009;30:255–63. doi: 10.1097/DBP.0b013e3181a7ed5a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Wiehe SE, Aalsma MC, Liu GC, Fortenberry JD. Gender differences in the association between perceived discrimination and adolescent smoking. Am J Public Health. 2010;100:510–6. doi: 10.2105/AJPH.2009.169771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Kramer MR, Hogue CR. Is segregation bad for your health? Epidemiol Rev. 2009;31:178–94. doi: 10.1093/epirev/mxp001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Jackson SA, Anderson RT, Johnson NJ, Sorlie PD. The relation of residential segregation to all-cause mortality: a study in black and white. Am J Public Health. 2000;90:615–7. doi: 10.2105/ajph.90.4.615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Winkleby M, Cubbin C, Ahn D. Effect of cross-level interaction between individual and neighborhood socioeconomic status on adult mortality rates. Am J Public Health. 2006;96:2145–53. doi: 10.2105/AJPH.2004.060970. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Rugh JS, Massey DS. Racial segregation and the American foreclosure crisis. Am Sociol Rev. 2010;75:629–51. doi: 10.1177/0003122410380868. [DOI] [PMC free article] [PubMed] [Google Scholar]