

Abstract
We describe a case of infective endocarditis due to Moraxella lacunata involving the native mitral and aortic valves, complicated by cerebral emboli and resultant hemiparesis. The patient was treated with ceftriaxone and gentamicin and improved. This appears to be the first case reported in the medical literature of native multivalvular endocarditis produced by this rare organism.
Keywords: Moraxella lacunata, multivalvular endocarditis, native valve endocarditis, cerebral emboli, modified Duke’s criteria
Background
M. lacunata is a non-fermentative Gram-negative coccobacillus, belonging to the Moraxella family. These bacteria constitute part of the normal flora of the respiratory and genital tracts. Of the various species of Moraxella, only M. catarrhalis is strongly associated with systemic infection, especially in patients with chronic pulmonary disease. Although well-known as a cause of conjunctivitis, keratitis and chronic sinusitis, M. lacunata is rarely associated with severe infections such as endocarditis.
Case details
A 32-year-old housewife diagnosed previously with multivalvular rheumatic heart disease, on irregular prophylaxis with penicillin, was admitted with a history of high grade fever and arthralgias for the past three weeks.
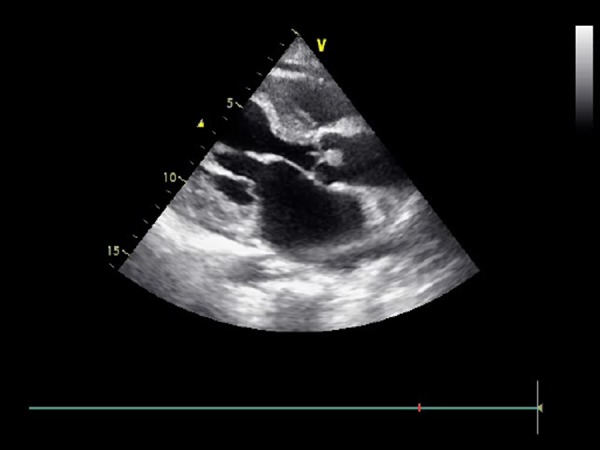
On examination, she was febrile and had mild pallor but exhibited no other signs of infective endocarditis. Cardiac examination revealed a pansystolic murmur at the apex and an ejection systolic murmur at the aortic area, with corresponding systolic thrills. Routine laboratory tests showed mild anaemia (Haemoglobin: 10.1 gm/dL), neutrophilic leucocytosis (17,200 cells/cu.mm; 87% neutrophils, 5% bands) and an elevated ESR (124 mm in first hour). Transthoracic echocardiography confirmed the presence of mitral regurgitation and aortic stenosis, as well as mitral stenosis and aortic regurgitation. Two vegetations were seen respectively on the aortic and mitral valve leaflets (see Figures 1, 2 and Figure 3).
Figure 1. Transthoracic echocardiography (apical two chamber view) showing mitral leaflet vegetations.
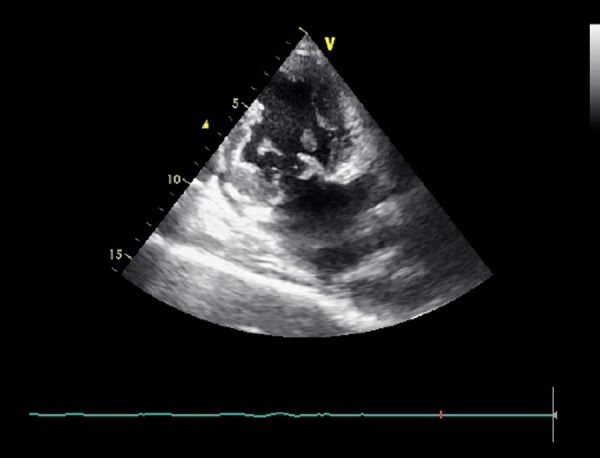
Figure 2. Transthoracic echocardiography (apical four chamber view) showing mitral leaflet vegetations.
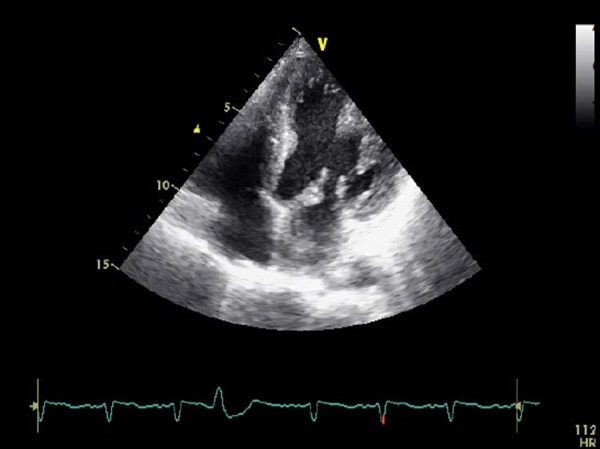
Figure 3. Transthoracic echocardiography (parasternal long axis view) showing aortic leaflet vegetations.
Five blood cultures were drawn and sent over the next 96 hours. Pending results, the patient was treated empirically with intravenous ceftriaxone and gentamicin. Despite early institution of therapy, she developed right-sided hemiparesis on the fifth day of hospital stay. CT imaging revealed an acute infarct in the left lentiform nucleus (see Figure 4).
Figure 4. CT head showing an acute infarct in the lentiform nucleus of the left basal ganglia.

A Gram-negative bacillus was isolated from all five blood cultures, ruling out the possibility of a contaminant. On further analysis, it was found to be catalase and oxidase positive. It was identified by the API 20NE system (Bio Merieux-France) as M. lacunata. Sensitivity testing by the disk-diffusion method demonstrated sensitivity to ampicillin, ceftriaxone and aminoglycosides; the same antibiotic regimen was therefore continued for the next six weeks.
Although serial transthoracic echocardiograms were suspicious of a root abscess, this possibility was ruled out by transesophageal echocardiography. Furthermore, the patient responded clinically with gradual reduction of her fever. Her hemiparesis also improved with only minimal residual deficits. She was kept on maintenance penicillin prophylaxis for rheumatic heart disease.
Patient consent
Signed informed consent was given by the patient for publication of material pertaining to this case.
Discussion
Although frequently associated with conjunctivitis, especially in the paediatric age-group1, M. lacunata is an exceedingly rare cause of endocarditis. Other unusual manifestations include acute meningitis, arthritis and septicaemia.2 To date, only eight cases of endocarditis have been reported in the medical literature. These were summarised by Maayan H et al3, who reviewed 16 cases of endocarditis due to various species of Moraxella, including five cases due to M. lacunata. Prior to this Robles et al4 had reported a case of M. lacunata producing prosthetic valve endocarditis. Subsequently, two more cases were reported by Noman F et al5, and Kutlesa M et al6. Only four of these cases fulfilled the modified Duke’s criteria.
Despite its rarity, Moraxella endocarditis can be severe. Systemic embolisation can occur to multiple organs including the brain and spleen. M. lacunata has a relatively predictable antibiotic profile and is most often sensitive to beta-lactams, although beta-lactamase producing strains have occasionally been reported. 7In our case, the isolate was not a beta-lactamase producing strain, and could therefore be treated by ceftriaxone and gentamicin.
Our case is unique in many ways. It fulfils the modified Duke’s criteria, making it a definite case of M. lacunata endocarditis. Unlike the majority of previously reported cases which involved prosthetic valves, our patient had native valve endocarditis. Furthermore, she had demonstrable multivalvular involvement, which has not been previously reported.
This case conclusively demonstrates the pathogenic potential and aggressive course of M. lacunata, as illustrated by the involvement of multiple native valves and cerebral embolisation. Awareness of this organism among practising physicians is crucial for institution of early aggressive management and prevention of devastating complications like embolic stroke.
ACKNOWLEDGEMENTS
Written consent for publication was obtained from the patient.
Footnotes
PEER REVIEW
Not commissioned. Externally peer reviewed.
CONFLICTS OF INTEREST
The authors declare that they have no competing interest.
FUNDING
None
CONSENT
The authors declare that
1. They have obtained informed consent for the publication of the details relating to the patient in this report.
2. All possible steps have been taken to safeguard the identity of the patient.
3. This submission is compliant with the requirements of local research ethics committees.
Please cite this paper as: Dasari S, Shetty RK, Devasia T. A rare case of Moraxella lacunata producing combined native mitral and aortic valve endocarditis. AMJ 2011, 4, 7, 386- 388 http//dx.doi.org/10.4066/AMJ.2011.718
References
- 1.Ringvold A, Vik E, Bevanger LS. Moraxella lacunata isolated from epidemic conjunctivitis among teen-aged females. Acta Ophthalomol (Copenh) 1985;63(4):427–31. doi: 10.1111/j.1755-3768.1985.tb01558.x. [DOI] [PubMed] [Google Scholar]
- 2.Ray U, Kar S. Invasive infection due to Moraxella lacunata, an unusual pathogen. Southeast Asian J Trop Med Public Health. 2006;37(6):1183–6. [PubMed] [Google Scholar]
- 3.Maayan H, Cohen Poradosu R, Halperin E, Rudensky B, Schlesinger Y, Yinnon AM, Raveh D. Infective endocarditis due to Moraxella lacunata: Report of 4 patients and review of published cases of Moraxella endocarditis. Scand J Infect Dis. 2004;36(11-12):878–81. doi: 10.1080/00365540410024925. [DOI] [PubMed] [Google Scholar]
- 4.Robles M, Tejada J, Jerez V, Pérez D, Jimeno B, Julia JA. Endocarditis caused by Moraxella lacunata on the natural and prosthetic valves. An unusual pathogenesis. Enferm Infecc Microbiol Clin. 1998;16(6):290–1. [PubMed] [Google Scholar]
- 5.Noman F, Khan SG, Khursheed M, Noor SA, Abubaker J. Moraxella lacunata endocarditis treated with penicillin. J Pak Med Assoc. 2008;58:336–7. [PubMed] [Google Scholar]
- 6.Kutleša A, Lepur D, Klinar I, Rudež D, Vincelj J, Bukovski S. et al. Moraxella lacunata: a rare cause of infective endocarditis. Scand J Infect Dis. 2007;39(10):917–9. doi: 10.1080/00365540701403002. [DOI] [PubMed] [Google Scholar]
- 7.Nagano N, Sato J, Cordevant C, Nagano Y, Taguchi F, Inoue M. Presumed endocarditis caused by BRO betalactamase- producing Moraxella lacunata in an infant with Fallot's tetrad. J Clin Microbiol. 2003;41(11):5310–2. doi: 10.1128/JCM.41.11.5310-5312.2003. [DOI] [PMC free article] [PubMed] [Google Scholar]