

Abstract
Background
Nurses are required to perform gluteal intramuscular (IM) injections in practice. There are dangers associated with erroneous performance of this task, particularly with dorsogluteal injections. Knowledge regarding safe injection practice is therefore vital for nursing students.
Method
Fifty-eight second year students at a New Zealand Nursing School were given schematic drawings of the posterior and lateral aspects of the gluteal region. They were asked to mark and justify the safest location for gluteal IM injections.
Results
Fifty-seven students marked the dorsal schematic and one the lateral, with 38 (66.7%) marking in the upper outer quadrant (UOQ). Twenty indicating the UOQ (52.6%) wrote ‘sciatic’ or ‘nerve’ in justifying their location.
Nineteen (33.3%) marked a location outside the UOQ; nine (47.4%) of these mentioned ‘sciatic’ or ‘nerve’ as reasons for injection safety. Overall, 50% of students mentioned ‘sciatic’ or ‘nerve’ in justifying the safety of their chosen injection location.
Conclusion
Results suggest some second year nursing students do not understand safe gluteal IM injection locations and rationale. Current teaching practices and IM injection techniques could be revisited to prepare students more effectively; this may help prevent pathologies arising from this procedure.
Keywords: Gluteal intramuscular injection, safety, nursing student
What this study adds:
Indicates some students lack knowledge surrounding correct placement of intramuscular injections.
Indicates some students have a lack of theoretical knowledge about safe injection practice with gluteal injections.
Highlights the importance of checking student technique prior to clinical placement.
Background
In clinical practice it is necessary for some health professionals to be able to perform gluteal intramuscular (IM) injections to introduce a number of drugs, including vitamins, steroid hormones and major tranquilisers. However, there are dangers associated with erroneous performance of this task, particularly with dorsogluteal IM injections.1-7 Dangers include damage to the sciatic nerve, with symptoms including complete paralysis of the muscles supplied by portions of the sciatic nerve, sensory loss, and paraesthesias.8-11
Historically, injuries to the sciatic nerve through poorly administered gluteal IM injections have been recorded since the 1920s.12-14 The ventro-gluteal IM injection site is now suggested as the safer region for gluteal IM injections, although the dorsogluteal site does remain popular in the mental health sector and by many other clinicians.5,12,15,16
Knowledge of safe gluteal IM injection practice is therefore vital for nurses; consequently it is important that nursing students are trained correctly in this procedure. The aim of this study was to investigate second year nursing students' knowledge of safe locations for gluteal IM injections. More specifically, are nursing students able to identify the correct location for gluteal IM injections and justify their choice of injection site in terms of safety?
Method
As a teaching exercise, 58 students halfway through their second year of a three year baccalaureate course at a New Zealand Nursing School were given black and white schematic drawings of the posterior (Figure 1) and lateral (Figure 2) aspects of the gluteal regions. These students were taught safe gluteal IM injection technique and rationale halfway through the first year of their course, and not formally instructed in the classroom by the institution at any time after this. Students were asked to mark the safest location for a gluteal IM injection on only one or other diagram, and list reasons justifying the safety of their chosen location.
Figure 1. Posterior view of gluteal region. Schematic drawing of the posterior aspect of the gluteal region. The region shaded in shaded in grey was not visible to students and indicates the upper outer quadrant of the buttock. This is the safest location for the introduction of a dorsogluteal intramuscular injection.
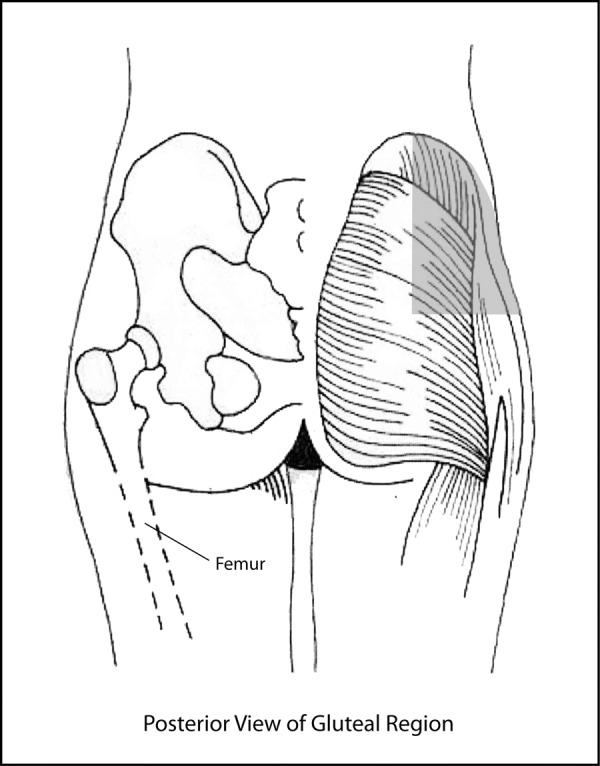
Figure 2. Lateral view of gluteal region. Schematic drawing of the lateral aspect of the gluteal region. The region shaded in grey was not visible to students. This shaded area indicates the safest region for the introduction of a ventrogluteal intramuscular injection.

A transparency with the safe regions indicated was overlaid on the completed schematics and the drawings assessed for IM injection location. For the posterior-view schematic the acceptable location for IM injection was within the boundaries of the upper outer quadrant of the buttock (Figure 1). In this instance this region is defined by dividing each buttock with a vertical line from the highest point of the iliac crest, followed by drawing a horizontal line through the midway point between the iscial tuberosity and the most superior point of the iliac crest. The region which is located in the most superior and lateral part of the four divisions is the upper outer quadrant.17 Injection locations were recorded as either inside or outside the upper outer quadrant. On the lateral-view schematic the acceptable location was within the reported triangular ventrogluteal region between the highest region of the iliac crest, anterior superior iliac spine, and a point approximately a palm's length above the greater trochanter (Figure 2).7 Any responses on this schematic were similarly grouped as inside or outside the accepted injection zone.
Justification of location safety was assessed as either ‘safe’ or ‘unsafe’. A safe response included reference to avoiding either the ‘sciatic nerve’ or ‘nerve’. If neither of these terms were present the justification was deemed to be ‘unsafe’. Departmental ethical approval was received for this exercise.
Results
Location
Fifty-seven students marked locations on the dorsal gluteal view and one marked on the lateral view, with 38 (66.7%) of the students marking the dorsal view indicating a site in the upper outer quadrant (UOQ) (Table 1). Nineteen students (33.3%) marked a location outside the UOQ, including three that marked outside the gluteal region. The single student who marked the lateral view indicated an area within the accepted ventrogluteal IM injection location for this region.
Table 1. Results for dorso-gluteal injection location and safety. Student responses from the dorsal schematic drawings grouped into injection location versus safe justification of injection site for dorsogluteal intramuscular injections. Safe justifications had to include the words ‘sciatic nerve’ or ‘nerve’. UOQ: upper outer quadrant.
| n = 57 | Safe Justification of Injection Site | ||
| Safe | Unsafe | ||
| Injection Location | UOQ | 20 | 18 |
| Outside UOQ | 9 | 10 | |
Safe justification of site
Of students marking the dorsal view, 20 (52.6%) students indicating a location within the UOQ wrote ‘sciatic’ or ‘nerve’ in justifying their location. Those marking outside the UOQ saw nine (47.4%) mention ‘sciatic’ or ‘nerve’ as reasons for injection safety. Overall, 50% of students mentioned ‘sciatic’ or ‘nerve’ in justifying the safety of their chosen injection location. The one student marking the lateral view correctly justified the safety of this location.
Analysis
A Chi-square analysis of the injection location and safe justification data provided a p-value of between 0.1 and 0.5, indicating that safe justification was unrelated to where students chose to locate their injection.
Discussion
Gluteal IM injection techniques are taught in nursing schools early in nursing training (Otago Polytechnic Curriculum 2010)18, prior to the students undertaking the bulk of their clinical placements. The results of this study suggest some second year nursing students in New Zealand do not understand safe dorsogluteal IM injection practice. Even though there are risks involved with injecting this area, the dorsogluteal region is still used for IM injections13,15,R19,20 and continues to be recommended in nursing texts and clinical practice.6,21 It is therefore paramount that this technique is learned correctly, with dorsogluteal IM injections directed to the UOQ (Figure 1) and the rationale for this placement reinforced.
Studies have indicated that pathologies arising from errant dorsogluteal IM injections are still a global problem affecting both adults and children alike with neuropathies induced by needle-inflicted injury of the sciatic nerve still occurring in large numbers.11,22 Significant proportions of injuries arising via this mechanism are still recorded in countries such as India, Pakistan, and Nigeria.16,22-26 In Pakistan alone between 2001 and 2003, the estimated annual incidence of traumatic injection neuropathy involving the sciatic nerve was thought to be around six million children.16 In New Zealand between July 2005 and September 2008 eight claims for sciatic nerve injury as a result of IM injection were made to the Accident Compensation Corporation (ACC), New Zealand's state owned accident insurance agency.7 Of these eight injuries, six occurred in a general practice setting, however whether the injections were performed by a nurse or general practitioner was not recorded by ACC. Symptoms for all patients included a combination of muscle weakness, sensory disturbance, and difficulty walking.
No guidelines exist for the placement of IM injections. Mishra and Stringer (2010)7 collated information from several professional bodies, and found the guidelines for immunisations from the UK (Royal College of Paediatrics27), USA (American Academy of Paediatrics28), and Australia (Australian Technical Advisory Group29) recommend the buttock should not be used for IM injections because of the risk of injury to the sciatic nerve. Injections into the dorsogluteal region not only risk damaging sciatic nerve, it is also not a good site for IM injections. In one study of 50 hospital patients injected with a 30mm needle in this region, 32% were found to have received the injection into the muscle, with most injections actually being subcutaneous.30 Yet despite this, and the fact that the ventrolateral gluteal location remains safer than the dorsogluteal, a recent study of New Zealand nurses showed that only 9% had used this site.31
Choice of location site
The vast majority of the students chose to place their injection on the dorsal schematic view of the buttock, and only one student chose the lateral view. This single student marked a location in the ventro-lateral gluteal region, the region most commonly promoted for gluteal IM injections to be introduced. Two-thirds of the students marking the dorsal view indicated their preferred location lay within the UOQ, however some of those that did not located their injection site directly over the path of the sciatic nerve, while others injected regions outside the gluteal region altogether. This indicates even basic anatomical knowledge should be revisited throughout the course of the degree when it is relevant to safe clinical practice, and in particular with reference to dorsogluteal injections.
The large number of students selecting the dorsal schematic view could be because of confusion surrounding the descriptive terminology used when dealing with the gluteal region. The instructions to students contained the word ‘gluteal’, and this term conjures up images of the buttock, not of the lateral hip area where the safer ventro-lateral gluteal injection site is located. Therein lies a conundrum when deciding how to best nominate a description for gluteal injections; perhaps the current description is misleading and the terminology used for injections in this region could be revisited, a suggestion also offered previously by Mishra and Stringer.7
Justification of safety
The introduction of any IM injection carries some risk,26 therefore with the dorsogluteal IM technique still being utilised it is critical that students and clinicians alike are able to provide the correct rationale for the safe introduction of injections in the gluteal region. A large number of students (50%) did not state either the word ‘nerve’ or ‘sciatic’ in justifying the site of their injection in the dorsogluteal region. Of the students that did not place their injection in the UOQ, 48% stated nerve or sciatic in their justification, indicating a knowledge that encompasses safe practice. However, these students still indicated their injection locations in a position that was potentially injurious. This suggests that even though some students recognise dangers are associated with performing an IM injection in this region, their clinical anatomical knowledge relating to the safety of this technique was poor.
This brief investigation does have some limitations. The schematic drawings were two-dimensional representations of a three-dimensional region, therefore some students may not have accurately appreciated where ‘true’ locations lay. In reality, the upper outer quadrant is most likely eye-balled from the posterior view in clinical situations, meaning there is some validity in presenting a two-dimensional diagram of this anatomical region for students to mark. Nevertheless the schematics of a muscular and bony outline of the posterior view and a bony outline of the lateral region may have presented the students with difficulty; some may have had problems appreciating the ‘actual’ anatomy given it was not ‘real’ or from a photograph of a person. There was also no investigation of the teaching methodology used to instruct the students, therefore it is not possible to determine how much influence this had over the observed outcomes. Despite these shortcomings the study does serve a useful purpose, indicating that many nursing students' knowledge of the location and rationale for safe placement of dorsogluteal IM injections is unsafe and should be improved.
Conclusion
Many nursing students chose a posterior gluteal location over a more lateral site when asked to identify a safe location for a gluteal IM injection, and many students' justifications of safe placement failed to take into account a major nerve (sciatic) being located in the dorsogluteal location. Even though dorsogluteal IM injections attract a higher likelihood of complications than injections into other areas such as the ventrogluteal site,13,19 this location remains an option for the introduction of medications. The results of this study suggests safe dorsogluteal IM injection practice should be revisited throughout the duration of nursing courses, thus ensuring correct technique for this procedure is reinforced and thereby helping prevent pathologies arising from errant injection technique. Educators and preceptors should be aware that some nursing students may have poor knowledge of IM injection techniques when they embark on clinical placements, and should check students' knowledge before they are required to perform such procedures in practice. It is also suggested the terminology ‘ventro-gluteal’ be revisited as a description for IM injections in the lateral hip region as the current description is perhaps misleading, validating a suggestion made by previous authors.7
Footnotes
PEER REVIEW
Not commissioned. Externally peer reviewed.
CONFLICTS OF INTEREST
The author declares that they have no competing interests.
FUNDING
Source of funding if applicable. Nil.
ETHICS COMMITTEE APPROVAL
Departmental ethical approval given. School of Nursing, Otago Polytechnic, Dunedin, New Zealand.
Please cite this paper as: Cornwall, J. Are nursing students safe when choosing gluteal intramuscular injection locations? AMJ 2011, 4, 6, 315-321 http//dx.doi.org/10.4066/AMJ.2011.764
References
- 1.Gillies FH, Matson DD. Sciatic nerve injury following misplaced gluteal injection. J Pediatr. 1970;76(2):247–254. doi: 10.1016/s0022-3476(70)80170-6. [DOI] [PubMed] [Google Scholar]
- 2.Greenblatt DJ, Allen MD. Intramuscular injection-site complications. JAMA. 1978;240(6):542–544. [PubMed] [Google Scholar]
- 3.Kline DG, Kim D, Midha R, Harsh C, Tiel R. Management and results of sciatic nerve injuries: a 24-year experience. J Neurosurg. 1998;89(1):13–23. doi: 10.3171/jns.1998.89.1.0013. [DOI] [PubMed] [Google Scholar]
- 4.Nicoll LH, Hesby A. Intramuscular injection: An integrative research review and guideline for evidence-based practice. Appl Nurs Res. 2002;16(2):149–162. doi: 10.1053/apnr.2002.34142. [DOI] [PubMed] [Google Scholar]
- 5.Kim DH, Murovic JA, Tiel R, Kline DG. Management and outcomes in 353 surgically treated sciatic nerve lesions. J Neurosurg. 2004;101(8):8–17. doi: 10.3171/jns.2004.101.1.0008. [DOI] [PubMed] [Google Scholar]
- 6.Wynaden D, Landsborough I, McGowan S, Baigmohamad Z, Finn M, Pennebaker D. Best practice guidelines for the administration of intramuscular injections in the mental health setting. International Journal of Mental Health Nursing. 2006;15:195–200. doi: 10.1111/j.1447-0349.2006.00423.x. [DOI] [PubMed] [Google Scholar]
- 7.Mishra P, Stringer MD. Sciatic nerve injury from intramuscular injection: A persistent and global problem. Int J Clin Pract. 2010;16(11):1573–1579. doi: 10.1111/j.1742-1241.2009.02177.x. [DOI] [PubMed] [Google Scholar]
- 8.Brown B. Sciatic injection neuropathy. Calif Med. 1972;116:13–15. [PMC free article] [PubMed] [Google Scholar]
- 9.Plewnia C, Wallace C, Zochodne D. Traumatic sciatic neuropathy: A novel cause, local experience, and a review of the literature. J Traum. 1999;47(5):986–992. doi: 10.1097/00005373-199911000-00036. [DOI] [PubMed] [Google Scholar]
- 10.Buhroo AM, Mir SA, Arshad S. Management of foot drop due to post injection sciatic nerve injury. Ind J Phys Med Rehabil. 2007;18(2):44–47. [Google Scholar]
- 11.Senes FM, Campus MD, Becchetti F, Catena N. Sciatic nerve injection palsy in the child: early microsurgical treatment and long-term results. Microsurg. 2009;29:443–448. doi: 10.1002/micr.20632. [DOI] [PubMed] [Google Scholar]
- 12.Rodger MA, King L. Drawing up and administering intramuscular injections: a review of the literature. J Adv Nurs. 2000;31:574–582. doi: 10.1046/j.1365-2648.2000.01312.x. [DOI] [PubMed] [Google Scholar]
- 13.Small SP. Preventing sciatic nerve injury from intramuscular injections: literature review. J Adv Nurs. 2004;47:287–296. doi: 10.1111/j.1365-2648.2004.03092.x. [DOI] [PubMed] [Google Scholar]
- 14.Malkin B. Are techniques used for intramuscular injection based on research evidence? Nursing Times. 2008;104:48–51. [PubMed] [Google Scholar]
- 15.Elsom S, Kelly T. Need for clinical practice guidelines for i.m. injections (letter) The Royal Australian and New Zealand College of Psychiatrists. 2009;43(9):877–878. doi: 10.1080/00048670903107633. [DOI] [PubMed] [Google Scholar]
- 16.Mansoor F, Hamid S, Mir T, Abdul Hafiz R, Mounts A. Incidence of traumatic injection neuropathy among children in Pakistan. EMHJ. 2005;11:798–804. [PubMed] [Google Scholar]
- 17.Drake RL, Vogl AW, Mitchell AWM, editors. 2. Sydney: Churchill Livingstone; 2010. Gray's Anatomy for Students; pp. 552–555. [Google Scholar]
- 18.Otago Polytechnic School of Nursing Curriculum 2010. Otago Polytechnic, Dunedin; New Zealand: Unpublished. [Google Scholar]
- 19.Ezeukwu AO. Injection-induced sciatic nerve injury among children managed in a Nigerian physiotherapy clinic: a five year review. J Rehabil Med. 2007;1(1):22–4. [Google Scholar]
- 20.Nemacheck B. A better injection site (letter) Am J Nurs. 2010;110(8):13. doi: 10.1097/01.NAJ.0000387666.51318.ad. [DOI] [PubMed] [Google Scholar]
- 21.Carter-Templeton H, McCoy T. Are we on the same page?: A comparison of intramuscular injection explanations in nursing fundamental texts. Medsurg Nurs 2008. 17:237–240. [PubMed] [Google Scholar]
- 22.Pandian JD, Bose S, Daniel V, Singh Y, Abraham AP. Nerve injuries following intramuscular injections: a clinical and neurophysiological study from Northwest India. J Periph Nerv Syst. 2006;11:165–171. doi: 10.1111/j.1085-9489.2006.00082.x. [DOI] [PubMed] [Google Scholar]
- 23.Fatunde OJ, Familusi JB. Injection-induced sciatic nerve injury in Nigerian children. Cent Afr J Med. 2001;47:35–38. doi: 10.4314/cajm.v47i2.8590. [DOI] [PubMed] [Google Scholar]
- 24.Ahuja B. Post injection sciatic nerve injury. Indian Pediatr. 2003;40:368–369. [PubMed] [Google Scholar]
- 25.Adetunji OO, Olusola EP, Joseph AO, Dare OJ, Ademola OG, Segun O. Injection-induced sciatic nerve injuries among children seen at a Nigerian physiotherapy unit. Internet J Third World Med. 2006;3 Available from: http://www.ispub.com/journal/the_internet_journal_of_thi rd_world_medicine/volume_3_number_2_53/article/injecti on_induced_sciatic_nerve_injuries_among_children_seen_ at_a_nigerian_physiotherapy_unit.html. [Google Scholar]
- 26.Tak SR, Dar GN, Halwai MA, Mir MR. Post-injection nerve injuries in Kashmir: a menace overlooked. J Res Med Sci. 2008;13:244–247. [Google Scholar]
- 27.Salisbury D, Ramsay M, Noakes K, editors. London: Department of Health; 2006. Immunisation Against Infectious Disease; p. 27. [Google Scholar]
- 28.American Academy of Pediatrics. Active Immunization. In: Red Book: 2006 Report of the Committee on Infectious Diseases. In: Pickering LK, Baker CJ, Long SS, McMillan JA, editors. 27. Elk Grove Village, IL: American Academy of Pediatrics; 2006. pp. 19–20. [Google Scholar]
- 29.Australian Technical Advisory Group on Immunisation of the Australian Government Department of Health and Ageing. 9. Australian Government; 2008. The Australian Immunisation Handbook; pp. 45–46. [Google Scholar]
- 30.Chan VO, Colville J, Persaud T, Buckley O, Hamilton S, Torreggiani WC. Intramuscular injections into the buttocks: are they truly intramuscular? Eur J Radiol. 2006;58:480–484. doi: 10.1016/j.ejrad.2006.01.008. [DOI] [PubMed] [Google Scholar]
- 31.Floyd S, Meyer A. Intramuscular injections - what's best practice? Why is there such a gap between what is taught in nursing schools about the best sites end technique for intramuscular injections and what actually happens in practice? Two nurses decided to find out. NZ Nurs J. 2007;13:20–22. [PubMed] [Google Scholar]