

Abstract
Background
Compliant, self-adjusting compression technology is a novel approach for durable prosthetic fixation of the knee. However, the long-term survival of these constructs is unknown.
Questions/purposes
We therefore determined the survival of the Compress® prosthesis (Biomet Inc, Warsaw, IN, USA) at 5 and 10 actuarial years and identified the failure modes for this form of prosthetic fixation.
Methods
We retrospectively reviewed clinical and radiographic records for all 82 patients who underwent Compress® knee arthroplasty from 1998 to 2008, as well as one patient who received the device elsewhere but was followed at our institution. Prosthesis survivorship and modes of failure were determined. Followup was for a minimum of 12 months or until implant removal (median, 43 months; range, 6–131 months); 28 patients were followed for more than 5 years.
Results
We found a survivorship of 85% at 5 years and 80% at 10 years. Eight patients required prosthetic revision after interface failure due to aseptic loosening alone (n = 3) or aseptic loosening with periprosthetic fracture (n = 5). Additionally, five periprosthetic bone failures occurred that did not require revision: three patients had periprosthetic bone failure without fixation compromise and two exhibited irregular prosthetic osteointegration patterns with concomitant fracture due to mechanical insufficiency.
Conclusions
Compress® prosthetic fixation after distal femoral tumor resection exhibits long-term survivorship. Implant failure was associated with patient nonadherence to the recommended weightbearing proscription or with bone necrosis and fracture. We conclude this is the most durable FDA-approved fixation method for distal femoral megaprostheses.
Level of Evidence
Level IV, therapeutic study. See Instructions for Authors for a complete description of levels of evidence.
Electronic supplementary material
The online version of this article (doi:10.1007/s11999-012-2635-6) contains supplementary material, which is available to authorized users.
Introduction
Megaprostheses need improved bone fixation to reduce the rate of aseptic loosening associated with stemmed implants. Young patients cured of tumors have a long life expectancy and a compelling need for prosthetic fixation that is equally long-lasting. A recently developed strategy is compliant compressive fixation that uses compression, via a short traction bar, to stimulate osteointegration at the bone-prosthetic interface, promote hypertrophy of the loaded bone, and avoid stress bypass of the host bone around a stiff intramedullary stem [2]. The Compress® Compliant Pre-Stress Implant (Biomet Inc, Warsaw, IN, USA), a rotating-hinge knee prosthesis, was approved by the FDA based on data from an unpublished short-term feasibility study, conducted by the manufacturer, that showed no difference in the acute complication rate and equivalent functional outcome scores compared with a cemented stem coupled to the same rotating-hinge articulation (Orthopaedic Salvage System [OSS™]; Biomet). Published studies of this device include an investigation in 26 patients, among whom only 10 had followup longer than 24 months [4], a study of 26 patients followed for a period of 0.3 to 9.2 years [23], and a study of 41 patients followed for 3 to 97 months [9]. These studies suggest projected 10-year prosthetic survival is at least 80%, but the number of cases is small and the number followed for this duration is miniscule.
We therefore determined the survival of the Compress® prosthesis at 5 and 10 actuarial years and identified the failure modes for this form of prosthetic fixation. Finally, the results were compared with those reported in a comprehensive review of the literature to establish the superiority of this method of fixation compared to those previously reported.
Patients and Methods
We retrospectively reviewed all 82 patients treated for distal femoral reconstructions after major bone resection from January 1998 to November 2008 at our institution. This implant was used for all primary and secondary (revision) femoral reconstructions, except for cases in which the remaining bone was inadequate due to insufficient cortical thickness, patient age of more than 70 years, metastatic disease, or prior irradiation of the femur (Table 1). Surgery was performed for tumor reconstruction in 80 patients and for noncancer revision TKA with massive bone loss in two patients. Followup was for a minimum of 12 months or until implant removal (mean, 48.4 months; median, 43 months; range, 6–131 months). Twenty-eight patients (> 33%) were followed for longer than 5 years. This study cohort includes the 41 patients in our earlier study who were followed for a mean of 45 months (range, 3–97 months) [9]. One additional patient underwent knee arthroplasty elsewhere and was followed at our institution. This patient was included for illustrative purposes because of an unusual complication (Type IIB bone failure, see below) that helped to establish our classification scheme of periprosthetic bone failure. The patient was not included in our patient cohort total or in the survivorship analysis. Patients were operated on for a variety of cancer diagnoses (Table 2). Our institutional review board approved this study.
Table 1.
Contraindications for use of the Compress® device for knee arthroplasty
| Cortical thickness of less than 2.5 mm |
| Pre- or postoperative bone irradiation, precluding osteointegration |
| Extraarticular resection of knee (an articulated implant, such as the Burstein-Lane® implant, would be indicated) |
| Inadequate or unreconstructable soft tissue envelope (a very low-profile implant, such as the GUEPAR® implant, would be indicated) |
| Metastatic disease that mandates immediate weightbearing (precludes the requisite 3 months of protected weightbearing) |
| Inability to cooperate with the postoperative program of early, protected weightbearing |
Table 2.
Patient demographic and clinical characteristics
| Characteristic | Value |
|---|---|
| Number of patients | 82 |
| Age (years)* | 20.4 (14–63) |
| Sex (number of patients) | |
| Male | 40 |
| Female | 42 |
| Reconstruction surgery (number of patients) | |
| Primary | 64 |
| Revision | 18 |
| Tumor diagnosis (number of patients) | |
| High-grade osteogenic sarcoma | 64 |
| Chondrosarcoma | 5 |
| Malignant fibrohistiocytoma | 5 |
| Giant cell tumor | 3 |
| Low-grade osteogenic sarcoma | 2 |
| Other tumor | 1 |
| No tumor (arthroplasty revision) | 2 |
* The value is expressed as the median, with range in parentheses.
All reconstructions at our institution were performed by the authors (JHH, CDM, EAA, PJB). The procedure followed the manufacturer’s recommended technique and has been described elsewhere [21]. Briefly, it entailed a sequence of steps after tumor or bone resection. The medullary canal was reamed just enough to accept the smallest anchor plug diameter of 12 mm or until there was endosteal contact for wider medullary canals. The anchor plug and traction bar were inserted into the canal. The muscle was bluntly split proximally to gain access to drill the bone, rather than disrupting the periosteal blood supply by stripping the bone. Using the outrigger for orientation (Fig. 1), three holes were drilled sequentially through the bone and anchor plug. After each hole was drilled, the drill bit was left in place to transfix both cortices and the anchor plug. After all three holes were drilled, the drill bits were replaced with fixation pins, which were tapped into place. We obtained a fluoroscopic image to confirm appropriate pin placement and length. Next, we used the conical reamer to prepare the surface of the host bone, constantly irrigating to prevent burning the bone and maintaining the periosteum as much as possible. The appropriate spindle size (small or large) and compressive force (400–800 pounds [181–363 kg]) varied according to the bone size and cortical thickness; compressive force levels recommended by the manufacturer were used (400 pounds [181 kg] for cortices 2.5–4.0 mm, 600 pounds [272 kg] for those 4.0–5.4 mm, 800 pounds [363 kg] for those ≥ 5.5 mm). The spindle and sleeve were placed over the intramedullary traction bar. The compression nut was tightened, approximately one half-turn beyond the point that initial resistance was felt, to compress the Belleville washers within the implant’s compression chamber. Although the manufacturer does not precisely specify the amount of torque required, the audible squeak of the washers signals that an appropriate level of tightening has been achieved (Video 1; supplemental materials are available with the online version of CORR). The remainder of the segmental knee arthroplasty was assembled as for the Orthopaedic Salvage System (OSS™) implant. In all patients, we used standard components, including an overall 8-cm anchor plug-traction bar construct; we did not use recently available options such as the 5-cm intramedullary implant. A typical case is illustrated, in which the implant was indicated for a short resection at the proximal femoral level (Fig. 2).
Fig. 1A–B.

(A) A diagram illustrates the outrigger that aligns the external drill guide with the intramedullary anchor plug. (B) A diagram demonstrates how the drill bits (through the outer two holes) and ultimately the fixation pins (through the central three holes) align. Reprinted with permission of Biomet Inc from Compress® Compliant Pre-Stress Device Orthopaedic Salvage System: surgical technique. Available at: http://www.biomet.com/orthopedics/getfile.cfm?id=1711&rt=inline. ©2012 Biomet Inc.
Fig. 2A–B.
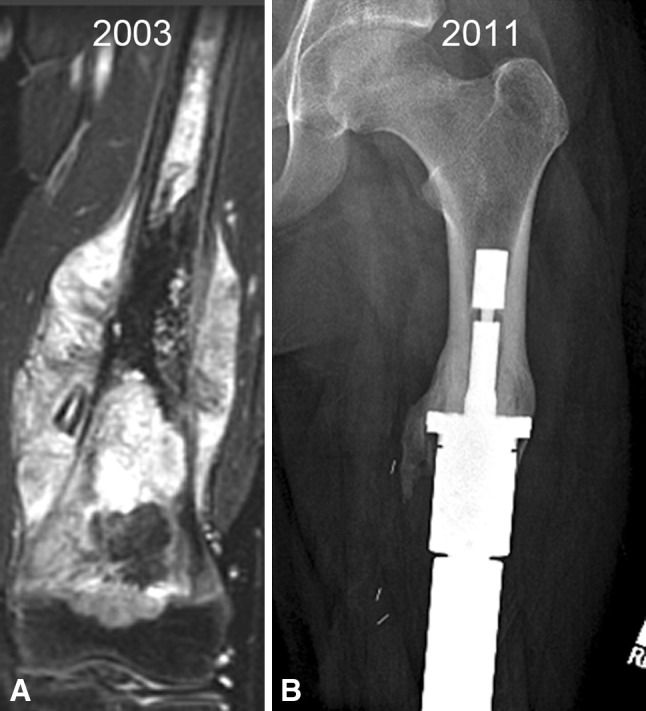
The Compress® is ideally suited for situations where there is a short remaining intramedullary canal that can only accommodate a short stem and fixation would be compromised. (A) An image shows the femur of a 15-year-old patient who had resection of a 25-cm osteogenic sarcoma of the distal femur that extended into the proximal 1/3 of the diaphysis and required a 28-cm resection. (B) A radiograph demonstrates how the surrounding bone responds to the compliant force over time.
All patients underwent a similar rehabilitation regimen. Continuous passive motion was initiated on Postoperative Day 2 if there was no visible evidence of wound necrosis and continued for approximately 2 weeks for approximately 18 hours/day. Patients started walking on the first postoperative day using toe-touch weightbearing for 6 weeks, 50% weightbearing for an additional 6 weeks, and then progressive weightbearing as tolerated. All were fully weightbearing within a month. Patient adherence to these guidelines was presumed. However, at least one patient did not comply with recommended weightbearing proscription and sustained a periprosthetic fracture and implant failure after carrying a boat, necessitating revision. Chemotherapy was resumed 2 to 3 weeks postoperatively when appropriate for a patient’s diagnosis.
Patients were seen on a variable schedule based on the patient’s diagnosis and disease activity. For high-grade cancers, this was initially every 2 months and ultimately once per year after a 4-year disease-free interval. Patients with benign disease were seen every 3 to 6 months initially and then annually after 4 years. Standard AP and lateral radiographs were obtained at each visit. Radiographs were examined for any deformation of the implant that suggested bending or breaking of the device or fracture of the bone. Any new or increased pain was noted. Radiographic signs of loosening were not specifically quantified because, to our knowledge, there is no suitable methodology for evaluating loosening for this construct. Compress® fixation failure was defined as revision of the fixation mechanism (anchor plug, traction bar, spindle, sleeve, or fixation pin) for any reason. Revision of intraarticular components (eg, polyethylene tibial bearing) that did not affect the bony fixation was not counted as a fixation or implant failure. Symptoms and signs of periprosthetic bone failure were noted and typically manifested as patient complaints of thigh pain and tenderness at the spindle-bone junction or reports of thigh pain during examination when the hip was rotated in the 90–90 position (supine, hip flexed 90°, knee flexed 90°). In such instances, radiographs were examined for evidence of a lack of osteointegration (ie, lack of hypertrophy in the bony segment between the spindle and the anchor plug and the presence of radiolucent lines at the spindle-bone interface). The presence of implant, bone, or symptomatic worsening prompted surgery.
In three patients who underwent revision surgery, we analyzed the bone adjacent to the junction site, both by visual inspection of the interface during surgery and by microscopic analysis of standard hematoxylin and eosin staining of decalcified samples.
Prosthesis-independent complications occurred but seemingly at a rate similar to what we have observed for other joint megaprostheses. There were three local recurrences; two were managed by local excision that did not affect the prosthesis and one required an amputation that removed the intact fixation. There were five prosthetic infections, including four primary infections and one secondary infection. The primary infections were successfully treated with washout, a change of intercalary segments, and retention of the Compress® fixation; there were no recurrences of infection. The secondary infection necessitated amputation that included removal of the intact prosthesis. The intact implants removed by the two amputations were considered censored at the time of the removal.
We performed survival analysis of the device by the Kaplan-Meier log-rank technique using SPSS® Version 14.0 (SPSS Inc, Chicago, IL, USA). Survival was defined as the time from the date of surgical implantation to the date of prosthesis removal or latest followup.
A comprehensive review of the literature was performed to place our results in context. A total of 718 articles were systematically read and reviewed. These were selected by performing a PubMed search on July 14, 2012, using the following key words: “megaprosthesis”, “femoral prosthesis”, “knee replacement”, and “tumor”. Articles that reported on the results of at least 20 patients for a mean of 5 years’ followup were considered. The results were further stratified based on studies that specified the number of distal femoral resections/reconstruction, the diagnoses for the surgical indications, and the prosthetic survivorship.
Results
Survivorship of the Compress® fixation was 85% at 5 years and 80% at 10 years (Fig. 3). There were three fixation failures in the first 2 years and five thereafter. Failures occurred throughout the followup period. Nevertheless, only one failure occurred among the 28 patients with more than 5 years of followup.
Fig. 3.

The Kaplan-Meier survival analysis of the Compress® prosthesis shows implant survivorship is 85% at 5 years (dashed line) and 80% at 10 years (dotted line).
The modes of prosthetic failure that required revision surgery varied (Fig. 4). There were eight failures of the interface, due to aseptic loosening alone (three implants) or aseptic loosening with periprosthetic fractures that affected the interface (five implants).
Fig. 4.

The flowchart shows the failure modes, treatment, and outcomes of the 13 patients who experienced bone and/or device failure after Compress® implantation. ORIF = open reduction and internal fixation.
Ten patients had periprosthetic bone failure. Five of the eight patients with aseptic loosening had bone failure, characterized by the absence of bone growth into the porous spindle, collapse of the bone prosthesis interface, and associated fracture between the anchor pins and the spindle. As described above, revision was necessary. We classified this mode of bone failure as Type I: affecting the interface (Fig. 5). A second type of bone failure did not require prosthetic revision and had two subtypes. The first, Type IIA, included three fractures proximal to the implant that did not disrupt the fixation (Fig. 6). These fractures were treated and healed without any disruption of the prosthetic-bone interface. Two patients had fractures that healed uneventfully and retained their prosthesis with its original Compress® fixation after further followup of 5 and 9 years, respectively. One patient healed her fracture but had an amputation for resultant osteomyelitis. Type IIB bone failure, which did not disrupt the interface or extend proximal to the anchor plug fixation pins, exhibited a unique pattern (Fig. 7). The spindle showed ingrowth at the posterior, but not anterior, aspect of the femur-spindle interface. Fracture occurred in a coronal plane. The integrated portion of the spindle remained attached to the posterior bone that fractured off as a segmental piece between the spindle and the anchor plug. There was some anterior angulation of the fracture, associated with a bent or broken traction bar. The anterior bone remained intact but had not integrated into the device, and a small separation was visible radiographically between anterior bone and the spindle. The displacement was not enough to require reduction. One patient from our cohort of 82 patients and the additional patient who underwent distal femoral reconstruction elsewhere had Type IIB failures. The first patient underwent an open bone-grafting procedure, at which time the fracture had already healed spontaneously. Because the second patient exhibited the same pattern, the fracture was allowed to heal without surgery, using only a functional fracture cast brace.
Fig. 5A–C.

Type I failure is a combination of interface and bone failure. At (A) 3 and (B) 6 months, the bone has not integrated at the prosthetic interface, and (C) at 10 months, it has fractured between the spindle and the anchor plug (arrow). Notably, the sleeve and tension bar acted like an inadequate stem and the traction bar broke.
Fig. 6A–B.

Type IIA failures are fractures proximal to the anchor plug fixation, perhaps at a stress transition point or, as in (A) this case where the bone was thin due to endosteal erosion from a failed prior stemmed implant (arrow). (B) The followup radiograph shows the fracture healed with a dynamic hip screw fixation and onlay allograft struts.
Fig. 7A–B.
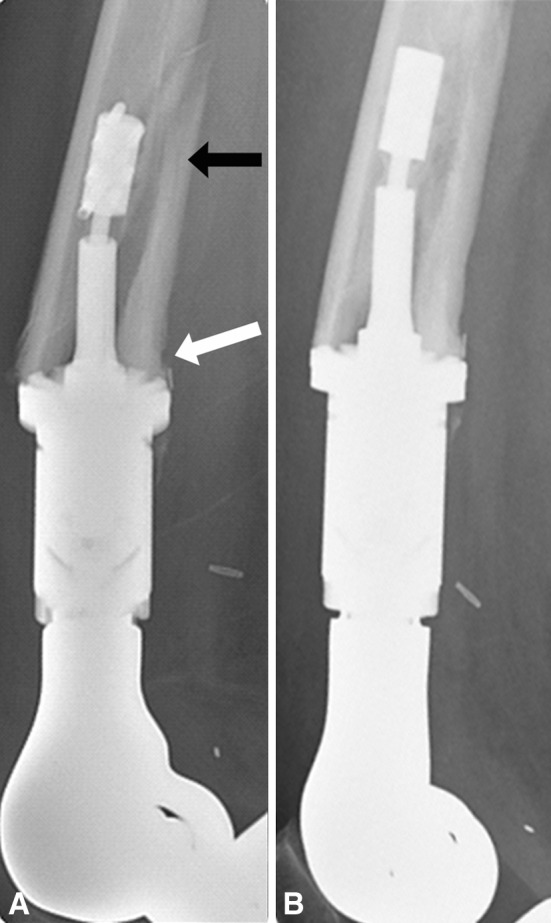
(A, B) Lateral radiographs taken 3 months apart show a Type IIB failure. (A) The black arrow points to the fracture of the posterior cortical segment that has moved with the spindle and the megaprosthesis, and the white arrow points to the intact bone-spindle interface where there has been some bone hypertrophy. Notably, the anterior cortex has not integrated and there is no hypertrophy. (B) The fracture healed spontaneously.
We performed a retrieval analysis of tissue in three patients from whom additional bone was removed, and there was no infection or cancer recurrence. Clinically, each patient had pain and radiographic failure. No well-fixed implants were analyzed. The specimens showed extensive osteonecrosis at the bone adjacent to the interface in each of the three specimens studied to date (Fig. 8). No other diagnostic histologic abnormalities were present.
Fig. 8A–C.

Type IIB failure shows (A) atrophy radiographically and (B, C) osteonecrosis histologically in two patient samples (Stain, hematoxylin and eosin; original magnification, ×40).
Discussion
Compliant, self-adjusting compression technology is a novel approach for durable prosthetic fixation of the knee. Early results have been encouraging, but longer followup reports are required from different centers. We therefore determined the survival of the Compress® prosthesis at 5 and 10 actuarial years and identified the fracture-associated failure modes for this novel form of prosthetic fixation.
Several factors limit the interpretation of this study. First, the absence of a control group makes it impossible to compare results directly with fixation from conventional cemented or uncemented intramedullary stems. This study does not prove this fixation method is better than historic options, even though the authors believe this is generally true. Previously, we had hoped to address this question through a prospective study protocol that would have compared Compress® fixation with press-fit and cemented stems. The protocol was proposed to a musculoskeletal oncology society, but the option of randomizing patients to the Compress® was rejected by the society’s surgeons; hence, definitive comparative conclusions may never be possible. However, in this study, we noted all 18 patients who were revised to a Compress® explicitly stated they were more comfortable with this implant, suggesting it was more stable and well fixed. Second, we only used the compliant fixation with a single design of rotating-hinge knee arthroplasty. Webber and Seidel [32] recently reported combining compliant fixation with a different body and articular design for pediatric limb salvage. Although the results are unlikely to have been different if a different knee design had been used, this question cannot be answered by this study. Patients in our cohort were treated over the course of a decade, and unrecognized differences in the population or surgical technique could have occurred. This problem plagues reviews of all low-incidence conditions that require many years to accumulate enough cases for analysis. Third, the minimum followup was set at only 1 year to allow inclusion of the two Type IIB cases of periprosthetic bone failure. The Kaplan-Meier method and survival curves allow the reader to see the time course of fixation failures and how the duration of followup may affect the prosthetic survival.
We found the survivorship of Compress® implants for distal femoral reconstruction remained high, as confirmed in nearly twice as many patients as we previously reported and with followup extending to as long as 13 years. Eighty percent of patients retained their prosthesis after an actuarial 10 years of followup. These results extend our earlier report of 41 patients with a mean followup of 45 months (range, 3–97 months) [9]. The durability exceeds the survival of distal femoral/TKAs reported in most series, as reviewed by Bhangu et al. [4] and summarized in our systematic review (Table 3). Since 80% of patients with osteogenic sarcoma are currently expected to survive 10 years, prosthetic survival has yet to exceed patient survival. While the Compress® implant performs at least as well over time as prostheses with other forms of bone fixation, further improvement of prosthetic durability is needed, especially for young patients with good long-term prognosis from their cancer. This high rate of prosthetic survival is encouraging but also suggests there may be factors regarding the patients, the surgery, or the subsequent management that influence the durability of the prosthesis. Notably, this analysis may be site specific and may not apply to compliant compression fixation in other sites [22] or under different clinical circumstances [2]. The time course of failure sheds some light on the nature of the fixation and its durability. Contrary to our previous report, on more than one occasion, the implant failed after the first year. Failures continued throughout the followup period. Indeed, five needed revision more than 2 years after implantation. However, only one of 28 implanted for more than 5 years subsequently failed. Thus, the concept that this form of biologic fixation would be long-lasting if it had a chance to become established was neither proven nor disproven in this cohort. It highlights how the durability is time dependent and the results can apparently be different depending on the time frame of the analysis.
Table 3.
Summary of peer-reviewed literature reporting megaprosthesis survivorship
| Study | Year | Number of patients | Site | Prosthesis* | Implant survival (%) | Followup (years) |
|---|---|---|---|---|---|---|
| Unwin et al. [31] | 1993 | 218 | Distal femur | Stanmore | 65 | 10 |
| Langlais et al. [15] | 2006 | 26 | Distal femur | GUEPAR® II or custom press-fit cemented | 92 | 12.5 |
| Myers et al. [20] | 2007 | 332 | Distal femur | Stanmore | 67 | 10 |
| Zimel et al. [33] | 2009 | 47 | Distal femur | Howmedica 39 OSS™ 8 | 36 | 10 |
| Farfalli et al. [9] | 2009 | 50 | Distal femur | OSS™ uncemented | 71 | 10 |
| Shehadeh et al. [27] | 2010 | 101 | Distal femur | MSRS™ | 70 | 10 |
| Bergin et al. [3] | 2012 | 93 | Distal femur | MRS™/GMRS™ | 73 | 10 |
| Tan et al. [28] | 2012 | 78 | Distal femur | Custom | 71 | 10 |
| Roberts et al. [26] | 1991 | 135 | Distal femur | Stanmore | 72 | 5 |
| Horowitz et al. [11] | 1993 | 61 | Distal femur | Burstein-Lane® | 78 | 5 |
| Kawai et al. [12] | 1999 | 25 | Distal femur | Finn® | 88 | 5 |
| Griffin et al. [10] | 2005 | 74 | Distal femur | KMFTR™ uncemented | 70 | 14 |
| Bruns et al. [8] | 2007 | 13 | Distal femur | MUTARS® | 87 | 7 |
| Kinkel et al. [13] | 2010 | 49 | Distal femur | MUTARS® | 57 | 5 |
| Matsumine et al. [17] | 2011 | 69 | Distal femur | Kyocera | 85 | 5 |
| Ritschl et al. [25] | 1992 | 206 | Mixed | KMFTR™ | 73 | 10 |
| Unwin et al. [31] | 1993 | 218 | Mixed | Stanmore | 65 | 10 |
| Unwin et al. [30] | 1996 | 1001 | Mixed | Stanmore | 67.4 | 10 |
| Mascard et al. [16] | 1998 | 90 | Mixed | GUEPAR® | 60 | 10 |
| Mittermayer et al. [18] | 2001 | 41 | Mixed | KMFTR™ | 53 | 11 |
| Plötz et al. [24] | 2002 | 64 | Mixed | Custom | 25 | 10 |
| Bickels et al. [6]† | 2002 | 110 | Mixed | MSRS™ | 88 | 10 |
| Biau et al. [5] | 2006 | 56 | Mixed | Custom | 50 | 11 |
| Morgan et al. [19] | 2006 | 105 | Mixed | HMRS™ | 59 | 10 |
| Current study | 2012 | 82 | Distal femur | Compress® | 80 | 10 |
* Prostheses include Stanmore (Stanmore Implants Worldwide Ltd, Elstree, UK); GUEPAR® II (Stryker France, Lyon, France); OSS™ = Orthopaedic Salvage System (Biomet Inc, Warsaw, IN, USA); MSRS™ = Modular Segmental Reconstruction System (Stryker Howmedica, Mahwah, NJ, USA); MRS™/GMRS™ = Modular Replacement System/Global Modular Replacement System stems (Stryker Howmedica); Burstein-Lane® implant (Biomet Inc, Warsaw, IN, USA); Finn® (Biomet Inc); KMFTR™ = Kotz Modular Femur Tibia Reconstruction System (Howmedica, Rutherford, NJ, USA); MUTARS® = Modular Universal Tumour And Revision System (Implantcast GmbH, Buxtehude, Germany); Kyocera (Kyocera Medical Corp, Osaka, Japan); HMRS™ = Howmedica Modular Replacement System (Howmedica); †patients in this study were also included in the analysis by Shehadeh et al. [27].
The unique fixation method of this prosthesis showed a unique spectrum of failure mechanisms. Aseptic loosening, commonly reported with other cemented and uncemented prostheses, also occurred with this implant. However, the aseptic loosening differed from that seen with other implants since bone ingrowth failed despite the continuously adjusting compression generated by the Belleville washers in the compression chamber. Retrieval specimens of these failures showed avascular necrosis of the underlying bone, in distinction to the viable bone found in well-fixed implants that were explanted for other reasons such as infection or tumor recurrence [7, 14]. A second, perhaps related unique finding was fracture or crumbling of the underlying bone between the anchor plug and the spindle. This was present in one patient who was included as part of a multicenter report on periprosthetic fractures around Compress® devices [29]. The phenomenon has not been singled out for analysis. It could not be determined whether the osteonecrosis led to fatigue failure of the bone or the fracture caused osteonecrosis near the interface. The pathophysiology of these failures is unproven. Treatment of fractures related to prosthetic failure was not the focus of this study but is reportedly relatively easy and yields pain-free, functional reconstructions with few complications [1, 29].
Our analysis demonstrates a survivorship of 80% for Compress® knee arthroplasty; the only published report demonstrating better survivorship after 10 years is that of Langlais et al. [15], who utilized custom-made press-fit femoral revision stems in 20 of the 26 joint arthroplasties. Thus, this report is the most comprehensive to date on an FDA-approved device for this unique form of prosthetic fixation.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Acknowledgments
The authors thank the Major Fellowship in Musculoskeletal Oncology, the Pearlman Oncology Fund, and the Limb Preservation Fund for providing financial support.
Open Access
This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Footnotes
One of the authors (JHH) certifies that he has received, during the study period, funding from the Major Fellowship in Musculoskeletal Oncology, the Pearlman Oncology Fund, and the Limb Preservation Fund. Each author certifies that he or she, or a member of his or her immediate family, has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA approval status, of any drug or device before clinical use.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
References
- 1.Abrams GD, Gajendran VK, Mohler DG, Avedian RS. Surgical technique: methods for removing a Compress® Compliant Pre-Stress Implant. Clin Orthop Relat Res. 2012;470:1204–1212. doi: 10.1007/s11999-011-2128-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Avedian RS, Goldsby RE, Kramer MJ, O’Donnell RJ. Effect of chemotherapy on initial compressive osseointegration of tumor endoprostheses. Clin Orthop Relat Res. 2007;459:48–53. doi: 10.1097/BLO.0b013e3180514c66. [DOI] [PubMed] [Google Scholar]
- 3.Bergin PF, Noveau JB, Jelinek JS, Henshaw RM. Aseptic loosening rates in distal femoral endoprostheses: does stem size matter? Clin Orthop Relat Res. 2012;470:743–750. doi: 10.1007/s11999-011-2081-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bhangu AA, Kramer MJ, Grimer RJ, O’Donnell RJ. Early distal femoral endoprosthetic survival: cemented stems versus the Compress implant. Int Orthop. 2006;30:465–472. doi: 10.1007/s00264-006-0186-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Biau D, Faure F, Katsahian S, Jeanrot C, Tomeno B, Anract P. Survival of total knee replacement with a megaprosthesis after bone tumor resection. J Bone Joint Surg Am. 2006;88:1285–1293. doi: 10.2106/JBJS.E.00553. [DOI] [PubMed] [Google Scholar]
- 6.Bickels J, Wittig JC, Kollender Y, Henshaw RM, Kellar-Graney KL, Meller I, Malawer MM. Distal femur resection with endoprosthetic reconstruction: a long-term followup study. Clin Orthop Relat Res. 2002;400:225–235. doi: 10.1097/00003086-200207000-00028. [DOI] [PubMed] [Google Scholar]
- 7.Bini SA, Johnston JO, Martin DL. Compliant prestress fixation in tumor prostheses: interface retrieval data. Orthopedics. 2000;23:707–711. doi: 10.3928/0147-7447-20000701-18. [DOI] [PubMed] [Google Scholar]
- 8.Bruns J, Delling G, Gruber H, Lohmann CH, Habermann CR. Cementless fixation of megaprostheses using a conical fluted stem in the treatment of bone tumours. J Bone Joint Surg Br. 2007;89:1084–1087. doi: 10.1302/0301-620X.89B8.19236. [DOI] [PubMed] [Google Scholar]
- 9.Farfalli GL, Boland PJ, Morris CD, Athanasian EA, Healey JH. Early equivalence of uncemented press-fit and Compress femoral fixation. Clin Orthop Relat Res. 2009;467:2792–2799. doi: 10.1007/s11999-009-0912-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Griffin AM, Parsons JA, Davis AM, Bell RS, Wunder JS. Uncemented tumor endoprostheses at the knee: root causes of failure. Clin Orthop Relat Res. 2005;438:71–79. doi: 10.1097/01.blo.0000180050.27961.8a. [DOI] [PubMed] [Google Scholar]
- 11.Horowitz SM, Glasser DB, Lane JM, Healey JH. Prosthetic and extremity survivorship after limb salvage for sarcoma: how long do the reconstructions last? Clin Orthop Relat Res. 1993;293:280–286. [PubMed] [Google Scholar]
- 12.Kawai A, Healey JH, Boland PJ, Athanasian EA, Jeon DG. A rotating-hinge knee replacement for malignant tumors of the femur and tibia. J Arthroplasty. 1999;14:187–196. doi: 10.1016/S0883-5403(99)90124-9. [DOI] [PubMed] [Google Scholar]
- 13.Kinkel S, Lehner B, Kleinhans JA, Jakubowitz E, Ewerbeck V, Heisel C. Medium to long-term results after reconstruction of bone defects at the knee with tumor endoprostheses. J Surg Oncol. 2010;101:166–169. doi: 10.1002/jso.21441. [DOI] [PubMed] [Google Scholar]
- 14.Kramer MJ, Tanner BJ, Horvai AE, O’Donnell RJ. Compressive osseointegration promotes viable bone at the endoprosthetic interface: retrieval study of Compress implants. Int Orthop. 2008;32:567–571. doi: 10.1007/s00264-007-0392-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Langlais F, Belot N, Ropars M, Lambotte JC, Thomazeau H. The long-term results of press-fit cemented stems in total knee prostheses. J Bone Joint Surg Br. 2006;88:1022–1026. doi: 10.1302/0301-620X.88B8.17722. [DOI] [PubMed] [Google Scholar]
- 16.Mascard E, Anract P, Touchene A, Pouillart P, Tomeno B. [Complications from the hinged GUEPAR prosthesis after resection of knee tumor: 102 cases] [in French] Rev Chir Orthop Reparatrice Appar Mot. 1998;84:628–637. [PubMed] [Google Scholar]
- 17.Matsumine A, Ueda T, Sugita T, Yazawa Y, Isu K, Kawai A, Abe S, Yakushiji T, Hiraga H, Sudo A, Japanese Musculoskeletal Oncology Group Clinical outcomes of the KYOCERA Physio Hinge Total Knee System Type III after the resection of a bone and soft tissue tumor of the distal part of the femur. J Surg Oncol. 2011;103:257–263. doi: 10.1002/jso.21823. [DOI] [PubMed] [Google Scholar]
- 18.Mittermayer F, Krepler P, Dominkus M, Schwameis E, Sluga M, Heinzl H, Kotz R. Long-term followup of uncemented tumor endoprostheses for the lower extremity. Clin Orthop Relat Res. 2001;388:167–177. doi: 10.1097/00003086-200107000-00024. [DOI] [PubMed] [Google Scholar]
- 19.Morgan HD, Cizik AM, Leopold SS, Hawkins DS, Conrad EU., 3rd Survival of tumor megaprostheses replacements about the knee. Clin Orthop Relat Res. 2006;450:39–45. doi: 10.1097/01.blo.0000229330.14029.0d. [DOI] [PubMed] [Google Scholar]
- 20.Myers GJ, Abudu AT, Carter SR, Tillman RM, Grimer RJ. Endoprosthetic replacement of the distal femur for bone tumours: long-term results. J Bone Joint Surg Br. 2007;89:521–526. doi: 10.1302/0301-620X.89B4.18631. [DOI] [PubMed] [Google Scholar]
- 21.O’Donnell RJ. Compressive osseointegration of modular endoprostheses. Curr Opin Orthop. 2007;18:590–603. doi: 10.1097/BCO.0b013e3282f0dafc. [DOI] [Google Scholar]
- 22.O’Donnell RJ. Compressive osseointegration of tibial implants in primary cancer reconstruction. Clin Orthop Relat Res. 2009;467:2807–2812. doi: 10.1007/s11999-009-0986-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Pedtke AC, Wustrack RL, Fang AS, Grimer RJ, O’Donnell RJ. Aseptic failure: how does the Compress® implant compare to cemented stems? Clin Orthop Relat Res. 2012;470:735–742. doi: 10.1007/s11999-011-2159-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Plötz W, Rechl H, Burgkart R, Messmer C, Schelter R, Hipp E, Gradinger R. Limb salvage with tumor endoprostheses for malignant tumors of the knee. Clin Orthop Relat Res. 2002;405:207–215. doi: 10.1097/00003086-200212000-00027. [DOI] [PubMed] [Google Scholar]
- 25.Ritschl P, Capanna R, Helwig U, Campanacci M, Kotz R. [KMFTR (Kotz Modular Femur Tibia Reconstruction System) modular tumor endoprosthesis system for the lower extremity] [in German] Z Orthop Ihre Grenzgeb. 1992;130:290–293. doi: 10.1055/s-2008-1039620. [DOI] [PubMed] [Google Scholar]
- 26.Roberts P, Chan D, Grimer RJ, Sneath RS, Scales JT. Prosthetic replacement of the distal femur for primary bone tumours. J Bone Joint Surg Br. 1991;73:762–769. doi: 10.1302/0301-620X.73B5.1894662. [DOI] [PubMed] [Google Scholar]
- 27.Shehadeh A, Noveau J, Malawer M, Henshaw R. Late complications and survival of endoprosthetic reconstruction after resection of bone tumors. Clin Orthop Relat Res. 2010;468:2885–2895. doi: 10.1007/s11999-010-1454-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Tan PX, Yong BC, Wang J, Huang G, Yin JQ, Zou CY, Xie XB, Tang QL, Shen JN. Analysis of the efficacy and prognosis of limb-salvage surgery for osteosarcoma around the knee. Eur J Surg Oncol. 2012 July 16 [Epub ahead of print]. [DOI] [PubMed]
- 29.Tyler WK, Healey JH, Morris CD, Boland PJ, O’Donnell RJ. Compress® periprosthetic fractures: interface stability and ease of revision. Clin Orthop Relat Res. 2009;467:2800–2806. doi: 10.1007/s11999-009-0946-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Unwin PS, Cannon SR, Grimer RJ, Kemp HB, Sneath RS, Walker PS. Aseptic loosening in cemented custom-made prosthetic replacements for bone tumours of the lower limb. J Bone Joint Surg Br. 1996;78:5–13. [PubMed] [Google Scholar]
- 31.Unwin PS, Cobb JP, Walker PS. Distal femoral arthroplasty using custom-made prostheses: the first 218 cases. J Arthroplasty. 1993;8:259–268. doi: 10.1016/S0883-5403(06)80087-2. [DOI] [PubMed] [Google Scholar]
- 32.Webber NP, Seidel M. Combining advanced technologies: the Compress-Repiphysis prosthesis for pediatric limb salvage. Orthopedics. 2010;33:823. doi: 10.3928/01477447-20100924-18. [DOI] [PubMed] [Google Scholar]
- 33.Zimel MN, Cizik AM, Rapp TB, Weisstein JS, Conrad EU., 3rd Megaprosthesis versus condyle-sparing intercalary allograft: distal femoral sarcoma. Clin Orthop Relat Res. 2009;467:2813–2824. doi: 10.1007/s11999-009-1024-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.