

Abstract
Introduction:
Periodontal diseases are becoming ever growing problem, not only for stomatology, but also for medicine overall, as the final result from this disease is loss of the teeth. The main cause for the emergence of the periodontal disease is bacterial activity from dental plaque. CPI index / Community Periodontal Index is recommended from the World Health Organization for epidemiological research, and for its application, graded probe WHO for periodontal tissue, which on the top has a ball with radius of 0.5mm, is essential.
The purpose of the research:
The purpose of the research was to determine the status of periodontal tissue for the sixth, seventh and eighth-grade students, and to examine if continuous education about oral hygiene has a direct impact on the change on the value of CPI-index.
The examinees and methods:
The examinees and methods of research: during the research 300 schoolchildren (1994, 1995 and 1996 generations, (100 schoolchildren of each generation)) were examined, and these were split into three groups. In the first group, there was no education, in the second group at the beginning of the research a session was held on proper tooth - brushing and importance of oral hygiene and in the third group continuous sessions were held in the period of six months, as per pre-determined timetable (i.e. at the beginning, after seven days, after one month, after three months). The schoolchildren were examined and their CPI - index was determined at the beginning and the end of the research.
The result:
The result of the research has been shown in a tabular and graphic form. For the schoolchildren, where there was a continuous education about the importance of the oral hygiene, the values of CPI - index have significantly changed.
Conclusion:
The status of periodontal tissue for the sixth-, seventh and eighth-grade schoolchildren is unacceptable, but the continuous education about the importance of the oral hygiene is giving very good results in the prevention of emergence of oral diseases.
Key words: prevention of periodontal disease, CPI - index, significance of continuous education.
1. INTRODUCTION
Periodontal diseases are becoming ever growing problem, not only for stomatology, but also for medicine overall, as the final result from this disease is loss of the teeth (1, 2, 3). The main cause for the emergence of the periodontal disease is bacterial activity from dental plaque (4, 5, 6, 7).
According to the World Health Organization (WHO) definition, 1978, the periodontal diseases are defined as inflammatory processes in periodontal tissue as a result of infection caused by the activity of local microbes. The development of the disease is the result of the activity of various groups of microorganisms. The development and effect of the disease are influenced by specific internal and external predisposed factors.
According to the postulate of the World Health Commission from 1961, which reads: “when the subgingival plaque is formed then gingival sulcus becomes the pathological pocket”, the prevalence of periodontal disease for our population is 100%. Also, oral diseases emerge frequently with children. After dental caries, gingivitis is mostly spread disease. Prevalence of periodontal disease for the schoolchildren under 14 years of age is 51,54%.
CPI index/Community Periodontal Index (7):
Recommended by the World Health Organization for epidemiological research.
Application of graded probe WHO for periodontal tissue, which on the top has a ball with radius of 0,5mm.
-
Indications for the determination of the index are (7):
Gingival bleeding,
Dental calculus,
Periodontal pockets.
Mouth cavity is divided into six sextants: 18-14, 13-23, 24-28, 38- 34, 33-43, and 44-48. Sextants can be examined only if there are minimum two teeth, which are not indicated for extraction.
For children under fifteen years of age, the depth of periodontal pockets was not examined. Only gingival bleeding and dental calculus were examined.
2. THE PURPOSE OF THE RESEARCH
Determine the status of periodontal tissue for the sixth, seventh and eighth grade schoolchildren.
Examine if continuos education about oral hygiene has a direct impact on the change of the value of CPI-index.
3. THE EXAMINEES AND METHODS
Total number of 300 schoolchildren 1996, 1997 and 1998 generations (100 schoolchildren of each generation) were split into three groups. In the first group there was no education, in the second group at the beginning of the research was held education on proper toothbrushing, nutrition, importance of oral hygiene and hygiene index was determined. In the third group five sessions for continuous education were held in the period of six months as per pre-determined timetable (at the beginning, after seven days, after one month, after three months). The students were examined and their CPI-index was determined at the beginning and end of the research.
For schoolchildren under fifteen years of age the depth of periodontal pockets was not examined. Only gingival bleeding and dental calculus were examined. Probing with periodontal probe was applied on the index teeth 16, 11, 26, 36, 31, 46 . In cases where one of index teeth was not present, the remaining teeth in the sextant were examined and the poorest finding was taken into consideration.
Attention was paid to apply the testing force not higher than 25 g (compliant with WHO - probe below the thumb nail until white circles emerge). The least possible force was applied for the examination of subgingival calculus because it provides the top of the periodontal probe to move along the tooth surface. During the application of the top of the probe anatomic configutaion of the rooth surface is followed.
The results were recorded in the following way:
0 – healthy periodont.
1 – gingival bleeding, clearly visible, or examined with the dental mirror.
2 – dental calculus.
X – sextant excluded, as a result of less than two teeth in the sextant.
4. RESULTS
Prevalence of the periodontal disease at the beginning of the research for 12-yearold schoolchildren in examined sample was 57%. For 13-year-old schoolchildren the value was 61%, and for 14-year-old schoolchildren this value was 62% (Graph 1).
Graph 1.

Values of CPI- index for examined sample
There is no significant change by sex for the prevalence of the periodontal disease (Chi2=1.280, p=0.258). There is no significant change for the emergence of gingival bleeding between boys and girls (Chi2=0.157, p=0.692, but there is a significant statistical change for the emergence of dental calculus between boys and girls (Chi2=3.350, p=0.067) as shown in the Graph 2.
Graph 2.

Changes of CPI-index values by sex.
Individual values of CPI-index by sex and age at the beginning of the research are shown in the Graph 3.
Graph 3.

Values of CPI- index
The impact of continuous education on values of CPI- index also researched. At the beginning of the research the schoolchildren were split into three groups. In the first group threre was no education, in the second group one session was held at the beginning. In the third group continuous education was held as per pre-determined timetable: at the beginning, after seven days, after one month, after three months and after six months. All schoolchildren were examined at the beginning and end of the research and their CPI-index was determined.
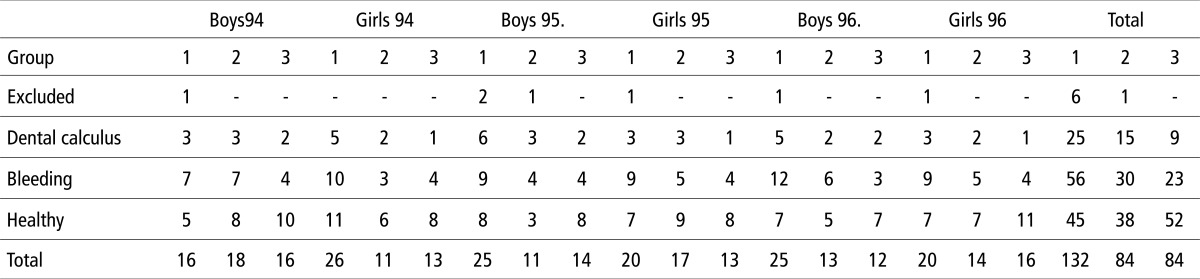
The values of CPI – index at the beginning of the research are shown in the Table 1 and the Graph 4.
Table 1.
Values of CPI - index at the beginning ot the research
 |
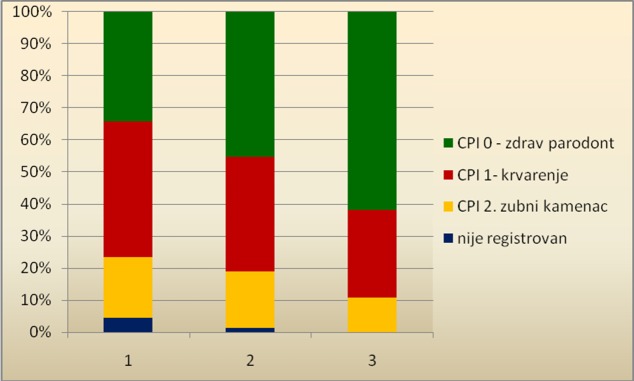
Graph 4.
Valuse of CPI- index by groups at the beginning of the research
Significant changes between groups at the beginning of the research were not recorded.
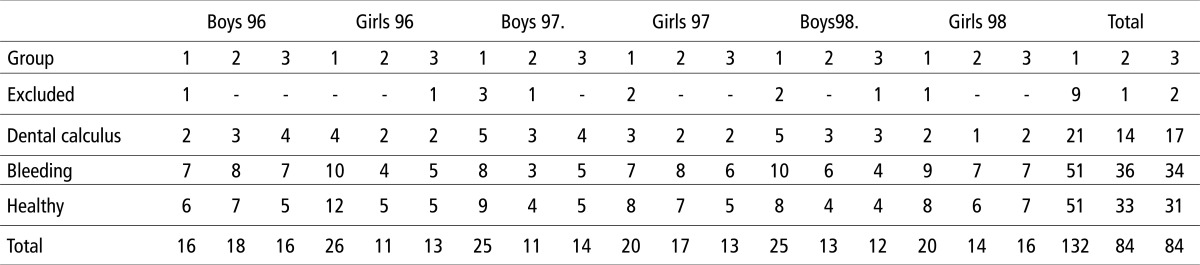
The results at the end of the research are shown in the Table 2 and the Graph 5.
Table 2.
Values of: CPI - index at the end of the research
 |
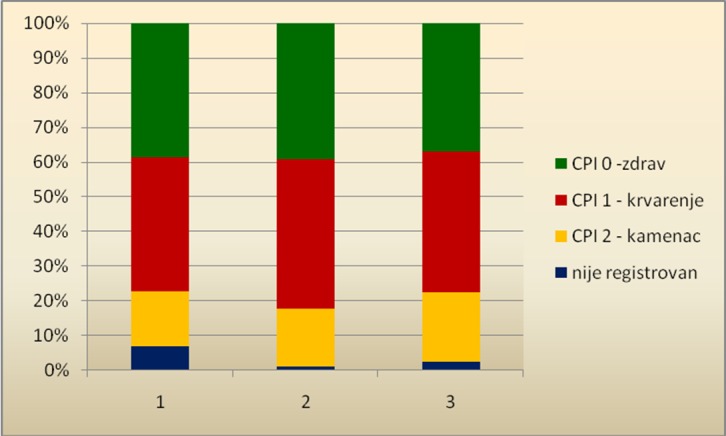
Graph 5.
Values of CPI- index at the end of the research
In the first group in which education was not held, no significant changes were found (Chi2=0.868, p=0.351), in the second group also, no significant changes were found (Chi2=0.615, p=0,433), but in the third group significant improvement of CPI-index was recorded (Chi2= 9.640, p= 0.002), as shown in the Graph 5.
5. DISCUSSION
Recording of CPI index was done in accordance with the World Health Organization guidelines for the population group under 15 years of age. Prevalnce of periodontal diseases was in the range from 57% for the 12-year-old schoolchildren to 63% for the 14-year-old schoolchildren. For 18% schoolchildren the emergence of dental calculus in the mouth cavity was recorded, while about 39.7% schoolchildren had gingival bleeding during probing.
The results of the former research in Bosnia and Herzegovina:
In 2000, Sulejmanagic H. et al. suggested that the periodontal status for 12-year-old schoolchildren in Bosnia and Herzegovina was: 54.4% of healthy sextants, 23.87% had the gingival bleeding and 17.95% sextants had dental calculus (3).
In 2008, Muratbegovic A. et al. (8) carried out the research in the entire area of Bosnia and Herzegovina and found out that 43% 12-yearold schoolchildren had healthy periodontal tissue, 43% had gingival bleeding and 12% had dental calculus (6, 7, 8).
The research in Sarajevo showed that 54.83% of children in Sarajevo had healthy periodont, 27.66% had gingival bleeding and 6% examinees had dental calculus. For children who were not born but moved to live in Sarajevo 66.66% had healthy periodont, 28% had gingival bleeding and 3.33% had dental calculus (1, 3, 5).
The results obtained in this research are similar to the results obtained in the reserach in Italy, in which 47.5% 12-year-old schoolchildren had CPI-0, i.e. signs of periodontal disease were not recorded. Bleeding was recorded in 23.8% examinees, and dental calculus was recorded in 28.7% cases (1, 9, 10, 11). In Germany, the situation is more acceptable, 80% od 12-year-old schoolchildren were recorded to have healthy periodont, 10.8% had gingival bleeding and 9.2% were recored to have dental calculus (4, 12, 13).
The major etiological cause for the emergence of dental caries and periodontal disease is the dental plaque. Plaque is the aggregation of bacteria and thier products on the tooth surfaces. Dental plaque is non-mineralized organized group of microorganisms in the organic matrix of mucopolysacharides (if tooth surface is polished and free from any dental deposits, in the period ranging from 15 minutes to two hours, a thin, soft, sticky, acellular, abacterial glucoprotein deposit called pellicle will be formed. Pellicle emerges as a result of the activity of bacterial enzyme on saliva mucine, while saliva glucoproteins have high affinity to dental enamel hydroxylapatite). It looks like mucous squama on the tooth surface, difficult to remove. It can be removed mechanically, it is colorless, eye invisible, but with painting (eg. “geniciana-violet”) it can be clearly seen. It is localized supragingivally on the tooh surfaces (where it causes dental caries) and subgingivally in the sulcus and periodontal pockets (where it causes paradontitis). The quantity of plaque and number of bacteria in saliva directly affect every individual. Streptococcus mutans, Lactobacillus acidophilus and Actinomyieces viscosus are mostly responsible for the emergence of cariogenic components of the plaque.
Removal of plaque, the main purpose of tooth- brushing.
Tooth-washing has been one of the main parts of the program for prevention of dental caries.
In the Western countries about 90% populations wash teeth regularly and in a correct manner. Unfortunately, Bosnia and Herzegovina is still far from this standard. Therefore, education of children and parents should be the first step in the struggle for prevention of dental caries. For that purpose basic information and guidelines for prevention of tooth health, such as oral hygiene, regular visits to the dentist for examination are given to children and their parents in nursery schools, schools, pediatric clinics, visiting-nurse services, and other health institutions.
Control of tooth deposits (plaque) and reduction of cariogenic bacteria is the most important step for the prevention of the emergence of dental caries. Regular and complete oral hygiene is the most accessible, the most effective and the most cost-effective means to accomplish this objective. Through everyday practice in dental offices we meet patients who preserve their tooth health with correct oral hygiene and regular dentist examination. Regular and correct oral hygiene assume tooth-washing, regular tooth-brushing, optimal three times a day (in the evening before going to bed, in the morning after breakfast, after lunch, and desirable after eating sweets). In addition, cleaning of interdental space with dental thread and washing with mouth solutions are necessary.
6. CONCLUSION
The status of periodontal tissue for the sixth, seventh, and eighth grade schoolchildren is unsatisfactory.
Continuous education on the importance of oral health accomplishes good results for prevention of emergence of the oral diseases.
Timely diagnosis of the periodontal status and therapy for the status to be tretated, such as gingival bleeding and dental calculus prevent the emergence of serious complications that might lead to the loss of the teeth.
Prevention and promotion of oral health should start as soon as possible to avoid the emergence of the oral diseases.
Conflict of interest
None declared.
REFERENCES
- 1.Tahmišcija H, Ganibegovic-Selimovic M, Kobašlija S. Sarajevo: Svjetlost; 1998. Prevention in Child Stomatology. [Google Scholar]
- 2.Maglajlic N. Oral health – prevention aspects. Faculty of dental medicine of the University of Sarajevo. 2001.
- 3.Sulejmanagic H, Kobašlija S, Sadikovic M, Huseinbegovic A, Selimovic-Dragaš M, et al. Stomatology today in Bosnia and Herzegovina. Bulletin of Doctor’s Chamber in Zenica-Doboj Canton. 2001 Jun;2:41–6. [Google Scholar]
- 4.Brauner K. Jena: Friedrich-Schiller-Universitaet Jena; 2005. Territorialdiagnose zur Mundgesundheit und ihren Einflussfaktoren bei Kindern und Jugendlichen (dissertation) [Google Scholar]
- 5.de Almeida C, Petersen PE, André S, Toscano A. Changing oral health status of 6- and 12-year-old schoolchildren in Portugal. Community Dental Health. 2003;(20):211–216. [PubMed] [Google Scholar]
- 6.Selimovic-Dragaš M. Sarajevo: University of Sarajevo; 2002. The Impact of Environment on Oral Health of Displaced Children (Master thesis) [Google Scholar]
- 7.Deljo E. Sarajevo: University of Sarajevo; 2009. Epidemiological Studies and Application of Preventive Measures for Oral Diseases in Bosnia-Podrinje Canton (Master thesis) [Google Scholar]
- 8.Muratbegovic A, Markovic N, Kobašlija S, Zukanovic A. Oral Health Index and Hypo mineralization of Molars and Incisors of Bosnian 12 years of age. Acta Stomatol Croat. 2008;42(2):155–163. [Google Scholar]
- 9.Papanon PN, Lindke J. Zagreb: “Globus”; 2004. Clinical Periodontology and Dental Implantology; pp. 60–178. [Google Scholar]
- 10.Topic B. Sarajevo: “Svjetlost”; 1990. Periodontology. [Google Scholar]
- 11.Matsson L. Periodontal Status of Children and Adolescents. In: Ured Koch G, Poulsen S, editors. Pedodontics – clinical approach. Zagreb, Naklada: „Slap“; 2005. pp. 235–252. [Google Scholar]
- 12.Ainamo J, Holloway PJ. Principal requirements for controlled clinical trials of caries preventive agents and procedures; Technical report No 1. Third edition; Commission on Oral Health, Research and epidemiology. Int Dent J. 1982 Sep;32(3):293–305. [PubMed] [Google Scholar]
- 13.Ainamo J, Nordblad A, Kallio D. Use of CPITN in population under 20 years of age. Int Dent J. 1984 Dec;34(4):285–91. [PubMed] [Google Scholar]