

Abstract
Pneumorachis or epidural emphysema is defined as free air in the spinal canal which is seen following trauma, head trauma, manipulations, epidural injections, and spinal surgery. We report on the case of a 62-year-old with cervical and thoracic pneumorachis following a traffic accident.
Keywords: pneumorachis, epidural, emphysema
Introduction
Pneumorachis or epidural emphysema is defined as free air in the spinal canal. It has been described following chest trauma, head trauma, manipulations, epidural injections, spinal surgery, ERCP and/or which occurs iatrogenically.1-11 We report on a 62-year-old with isolated cervical and thoracic pneumorachis following a traffic accident.
Case Report
A 62-year-old male driver was involved in a head-on collision with another car in a high-speed traffic accident. He was evacuated from the scene and transferred to the regional hospital. CT of the chest and abdomen, per-formed as a part of the trauma series due to the mechanism of injury, revealed pneumorachis in the cervical and thoracic spine without any spinal fractures. Air was noted in the epidural space and neural foraminae (Figures 1, 2). There was a large amount of subcutaneous emphysema in the paraspinal muscles (Figure 1). No neurological deficit could be elicited. He was examined by a spinal surgeon who clinically cleared his cervical spine. The pneumorachis was managed conservatively and the pa-tient subsequently made an uneventful recovery.
Figure 1. Axial ct of the upper thoracic spine and sagittal reconstruction of the cervical spine demonstrating air in the epidural space (arrow) and within the paraspinal muscles.
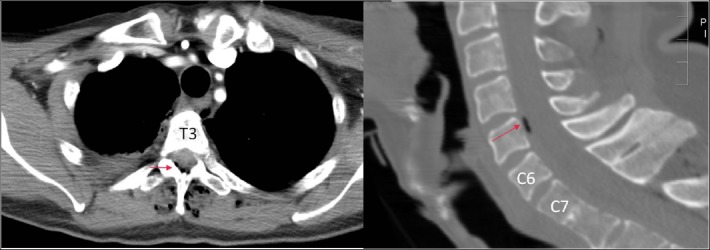
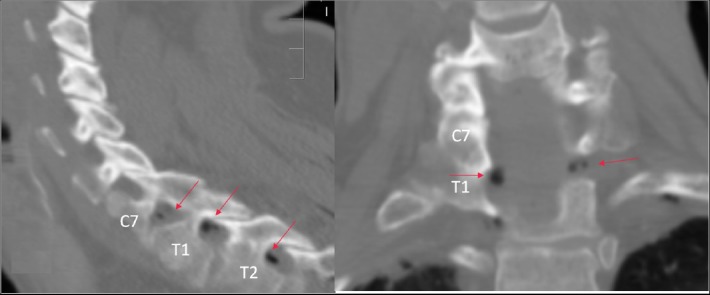
Figure 2. Sagittal ct and coronal reconstruction of the cervicothoracic spine demonstrating epidural emphysema tracking into the neural foramina.
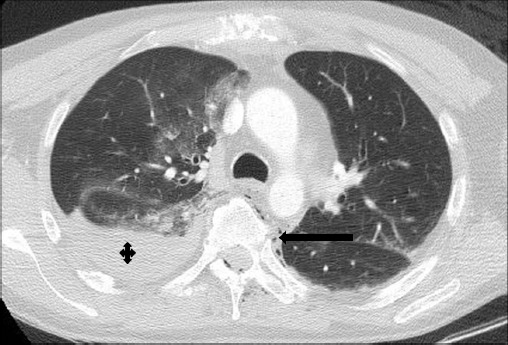
There was no associated pneumothorax or free intraabdominal air. The patient had a right hemothorax and a non-displaced sternal fracture with a small amount of pneumomediastinum (Figure 3). The hemothorax was treated with an intercostal chest drain. He had sustained a right femoral fracture as well which was managed with an intramedullary nail.
Figure 3. Axial contrast-enhancedct (lung windows) showing large right hemothorax (+) with pneumomediastinum (arrow).
Discussion
Pneumorachis is a rare and under-diagnosed condition.1,5 Air has been described in the literature in epidural, extradural and subarachnoid spaces.1,3,5 New-bold described pneumorachis following basilar skull fractures.11 Epidural emphysema is also described following epidural and spinal injections. Asthma is also one of the etiological factors. 6 Other causes can include blunt trauma, tumor, abscess and vacuum disc. 3,4,7 Kon et al. reported epidural air in all patients with spontaneous pneumomediastinum.8 These are usually asymptomatic. Radicular symptoms are a rare presentation of epidural emphysema3, and are managed conservatively, though Krasoudakis and colleagues suggested percutaneous aspiration of air in patients with a neurological deficit.3 The presence of intrathecal air following trauma should be managed as an open injury due to the risk of meningitis.12
In this case, a large amount of air was noted in the paravertebral soft tissues. Air was also noted in multiple neural foraminae and in the spinal canal. We hypothesize that air from the subcutaneous emphysema tracked along the meningeal covering of the nerves, and even-tually tracked into the spinal canal. The patient was managed conservatively as he was asymptomatic. He made an uneventful and full recovery.
We feel that practitioners need to be aware of pneumorachis, especially in patients with blunt trauma, and that such patients should be managed with expectant treatment.
References
- 1.Sharma M, Garg S, Gupta S. Thoraco-abdominal pneumorrhachis following pneumomediastinum pneumoretroperitoneum, cervical, thoracic and abdominal wall subcutaneous emphysema after retroduodenal perforation: Case report of a rare ra-diologic fnding. European Journal of Radiology Extra. 2009;71(3):e131–e134. [Google Scholar]
- 2.Coskun S, Sahin M, Cobanoglu M, Kilicaslan I. Entire pneumorrhachis due to isolated head trauma. Am J Emerg Med. 2009;27(7):902.e3–6. doi: 10.1016/j.ajem.2008.11.004. [DOI] [PubMed] [Google Scholar]
- 3.Krasoudakis A, Marathianos S, Tsiminikakis N, Chavredakis E, Arhontakis G. Intraspinal air after blunt thoracic trauma. J Indian Assoc Pediatr Surg. 2006;11:248–9. [Google Scholar]
- 4.Gautschi OP, Hermann C, Cadosch D. Spinal epidural air after severe pelvic and abdominal trauma. Am J Emerg Med. 2008;26(6):740.e3–5. doi: 10.1016/j.ajem.2007.11.042. [DOI] [PubMed] [Google Scholar]
- 5.Lin MB, Cheah FK, Ng SE, Yeo TT. Tension pneumocephalus and pneumorachis secondary to subarachnoid pleural fstula. BJR. 2000;73(867):325–7. doi: 10.1259/bjr.73.867.10817052. [DOI] [PubMed] [Google Scholar]
- 6.Manden PK, Siddiqui AH. Pneumorrhachis, pneumomediastinum, pneumopericardium and subcutaneous emphysema as complications of bronchial asthma. Ann Thorac Med. 2009;4(3):143–5. doi: 10.4103/1817-1737.53352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kim CH. Pneumorrhachis and paraspinal air with vacuum disc : case report and literature review. J Korean Neurosurg Soc. 2007;42(6):490–1. doi: 10.3340/jkns.2007.42.6.490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kono T, Kuwashima S, Fujioka M, Kobayashi C, Koike K, Tsuchida M, Seki I. Epidural air associated with spontaneous pneumomediastinum in children: uncommon complication? Pediatr Int. 2007;49(6):923–7. doi: 10.1111/j.1442-200X.2007.02480.x. [DOI] [PubMed] [Google Scholar]
- 9.Sharp EA. Ar tifcial pneumorachis in acute infections of the meninges. Arch. Neur. 4' Psych. 1921;6:669–73. [Google Scholar]
- 10.Ristagno ROSS l., Hiratzka LOREN f., Rost RAYMOND c., Jr An Unusual Case of Pneumorrhachis Following Resection of Lung Carcinoma. Chest. 2002;121:1712–1714. doi: 10.1378/chest.121.5.1712. [DOI] [PubMed] [Google Scholar]
- 11.Newbold RG, Wiener MD, Vogler Ill JB, Martinez S. Traumatic Pneumorrhachis. AJR. 1987;148:615–616. doi: 10.2214/ajr.148.3.615. [DOI] [PubMed] [Google Scholar]
- 12.North JW. On the importance of intracranial air. Br J Surg. 1971;58:826–82. doi: 10.1002/bjs.1800581106. [DOI] [PubMed] [Google Scholar]