

Abstract
A typical approach to categorizing substance users for epidemiologic purposes or to identify substance use problems at treatment admission is by indicating the primary substance used and/or for which treatment is sought. But does such singular focus on the primary drug limit the validity of conclusions from longitudinal analysis of drug use patterns over time? This analysis combined data from five longitudinal studies conducted in California and examined 10-year patterns of heroin, cocaine, methamphetamine (meth), marijuana, and alcohol use for primary users of heroin (n=629), cocaine (n=694), and meth (n=474). Results suggest relatively low levels of use of non-primary heroin, cocaine, and meth, but moderate levels of alcohol and marijuana use. Growth models showed declining primary drug levels for heroin and meth users and relatively consistent levels over 10 years for cocaine users, while levels of non-primary drugs remained at consistently low levels or declined in tandem with the primary drug. Results indicate that group descriptions of primary heroin, cocaine, or meth use trajectories over time may present valid information about drug use patterns in general.
Keywords: epidemiology, poly-drug abuse, trajectories, trends, growth models
1. Introduction
A typical approach to categorizing substance users for epidemiologic purposes or to identify substance use problems at treatment admission is by indicating the primary substance used and/or for which treatment is sought. Classification by primary substance allows both comparative analyses across primary users of different substances and clinical individualization of treatment since many neurophysiologic and psychosocial differences exist across drugs. However, a weakness of such a classification approach is the possibility that substance users may use more than one substance within any specified observation period. In practical terms, it is easier to compare and interpret differences among primary substance use typologies (e.g. opiates vs. stimulants vs. marijuana) as opposed to multiple categories representing all possible combinations of such substances in differing frequency of use. However, use of multiple substances may complicate some aspects of the assessment and understanding of dependence (Gossop, 2001). For example, focusing on a single primary substance may obscure the overall picture of substance use behavior if there is considerable polydrug use; and studies suggest that multiple dependencies may present a barrier to successful treatment intervention (e.g. Bovasso and Cacciola, 2003; Downey et al., 2000; Williamson et al., 2006).
But do these issues reduce the validity of studies of drug use patterns over time and related treatment outcomes? This may become an important issue when considering longitudinal patterns of substance use if “drug switching” is commonplace. In such a case, a researcher may conclude based on the primary drug that substance use is declining (e.g. as a result of treatment), but may miss observing an increase in the use of an alternative substance. While patterns of multiple substances can be analyzed simultaneously, the required analytic models can easily become too complex for reliable estimation and results may be difficult to interpret. To help elucidate these issues, we focus on the following questions: 1) to what extent do primary users of opiates, cocaine, and methamphetamine also use others of these substances or use marijuana or alcohol during the same periods observed over time, and 2) are trajectories of primary substance use over time related to trajectories of use of other substance. Results from the second question allow indirect inferences related to whether users tend to change to other drugs as use of their primary drug declines or whether a general use trajectory applies to all their drugs. Additional exploration targets the relationship of levels of use between different drugs at different points throughout the observation period.
Considerable polydrug use has been reported among substance users, from treatment and community samples (e.g. Booth et al., 2006; Byqvist, 2006; Darke et al., 2007; Flannery et al., 2004; Gossop et al., 2002; Hubbard et al., 1997; Leri et al., 2003; Malcolm et al., 2006; Martin et al., 1996). For example, in several studies one-third to over half of substance misusers or treatment samples (of primarily cocaine or heroin users) reported misuse of more than one class of substances (Gossop et al. 2003; Grella et al., 1995, 1997; Leri et al. 2005; Substance Abuse and Mental Health Services Administration [SAMHSA], 2007). Darke and Hall (1995) found that primary heroin users also used an average of 5.2 other classes of substances in the six months prior to treatment admission; primary methamphetamine (meth) users averaged 6.3 classes of other drugs in addition to meth (Brecht et al., 2005).
Research results also support the clinical and treatment implications of polydrug use, in terms of greater psychopathology (Beswick et al., 2001; Booth et al 2006; Malcolm et al., 2006; also Medina and Shear, 2007; Sumnall et al., 2004); higher levels of health risk behaviors (Patterson et al., 2005); and difficulties in engaging in treatment (John et al., 2001). There are also challenges in developing effective treatment approaches for polydrug users because of the different psychological and physiological effects of different substances (Kenna et al., 2007). While evidence is not consistent (Prendergast et al., 2002), several studies focusing primarily on heroin and cocaine use found polydrug use to be negatively related to treatment outcomes (Bovasso and Cacciola, 2003; DeMaria, et al., 2000; Downey et al., 2000; Williamson et al., 2006). Among meth users, secondary use of cocaine or heroin was a predictor of not completing treatment (Brecht et al., 2005). But the impact of polydrug use on treatment outcomes may also be dependent on the specific combinations of substances; for example, Epstein and Preston (2003) found little evidence of poorer treatment outcomes for heroin users who also used cannabis.
Evidence relevant to the issue of possible drug switching comes from several perspectives. A community prevalence study documented an increase in cocaine use following a heroin shortage in Australia (Topp et al., 2003). Jones and Weatherburn (2001) asked cannabis users directly whether they would switch drugs if cannabis became harder to get: about 1/3 said that they would switch to more alcohol use; fewer than 10% said that they would be likely to switch to other drugs. Studies of treatment outcomes (primarily for heroin and cocaine users) suggest that while some individuals may switch use (Gossop et al., 2002), drug switching may not be the norm. For example, Darke et al. (2006) found that among primary heroin users declines in weekly heroin use within the month preceding each interview (four observations over 24 months following treatment) coincided with decreasing use of other illegal drugs and with stability in alcohol use patterns. These results were similar to earlier studies (e.g. DeMaria et al., 2000; Fairbank et al. 1993; Gossop et al. (2003). Simpson et al. (2002) reported that among primary cocaine users, there were overall decreases in cocaine use as well as decreases in heroin and alcohol use at one- and five-year follow-up compared with treatment intake. However, the coincidence of patterns of use for primary and non-primary drugs may also be affected by other factors including type of treatment; for example, Hubbard et al. (1997) reported a stronger effect of residential treatment on non-primary drug use than that seen from outpatient methadone maintenance.
Thus, while polydrug use appears to be common among substance abusers, the longitudinal patterns of use of multiple substances, particularly in relation to the use of different types of primary substances, remain understudied. The current study expands the existing research base to include drug use trajectories covering 10-year substance abuse histories for primary users of heroin, cocaine, or methamphetamine. Together, these three drugs were the primary substance for 36% of admissions to treatment for substance use nationwide in 2005 (Substance Abuse and Mental Health Services Administration, 2007) and for 63% of California admissions in 2006 (CA Department of Alcohol and Drug Programs [CA ADP], 2007).
2. Methods
2.1 Sample/Data
To provide detailed data on patterns of substance use from a comprehensive sample of drug users, the current analysis combined non-overlapping samples from five studies that collected longitudinal information using the Natural History Instrument (described below). All studies were conducted in California. We selected from each study those subjects who reported a primary drug problem of heroin, cocaine, or meth.
Studies included the following (with numbers in parentheses of subjects selected for the current analysis): 1) 33-year Heroin Follow-up Study (n=472), in which subjects were originally sampled because of their participation in the California Civil Addict Program for their heroin use (Hser et al., 2001; data collected in 1996–97); 2) the Cocaine Treatment Evaluation (n=319), where the primary drug for treatment at study baseline assessment was cocaine (Hser et al., 2006; data collected in 1989–91 and 2002–2003); 3) Methamphetamine Natural History Study (n=350), in which subjects were originally sampled from treatment admissions for meth use (Brecht et al., 2004; data collected in 1998–2002); 4) Treatment Process Study (n=391), which sampled those treated for primary use of one of several types of substances (Hser et al., 2004; data collected in 1996); 5) Treatment Utilization and Effectiveness study (n=265), which included subjects recruited from non-treatment settings (emergency rooms, sexually transmitted disease clinics, and jails) and the primary drug type was self-identified (Hser et al., 2003; data collected in 1995–96). Each database provided sufficient numbers of cases of the primary drug type; when data were pooled (N=1,797), the number of subjects was 629 for heroin (35%), 694 for cocaine (39%), and 474 for meth (26%). See Hser et al., (under review) for additional detail comparing patterns of drug use.
2.2 Instruments
Data were collected using the Natural History Instrument (NHI) (McGlothlin et al, 1977; Nurco, et al., 1975). The NHI contains sections on personal and family background, physical and mental health, drug use and treatment, criminal history, and risk behaviors. A time-line follow-back type of approach for part of the interview collects a continuous history describing drug use and other behaviors from first substance use until the interview. Using a time line, the interviewee notes major events for reference and then identifies time periods associated with specific behaviors, with periods delineated by changes in behavior. These reported data are translated to time series-type data of behaviors for each month (including number of days of use of each designated substance). Test-retest and pattern reliability for NHI have been shown acceptable, for reported behaviors for a specified period recalled from initial and follow-up interviews (Anglin et al., 1993; Chou et al., 1996; Hser et al., 1992).
2.3 Variables
The term polydrug use has been applied to several different substance use contexts and definitions, which are important to differentiate in order to provide a context for the current analysis (e.g. Earleywine and Newcomb, 1997; McCabe et al., 2006; Schensul et al., 2005). The broadest interpretation relates to the substance user’s historical drug use, indicating previous use of other drugs, but not necessarily during relatively short specified observation periods. A narrower usage indicates use of other drugs during the same specified observation period (e.g. past 30 days, past year), including use of different drugs on different occasions within that period; this is sometimes labeled concurrent usage. A still narrower definition relates to simultaneous use of other drugs (that is, drugs consumed or administered together), also sometimes labeled co-ingestion or co-use. Our analyses focus on the second of these definitions, which also picks up the general levels of drug use from the third (narrowest) definition, but not specifically the co-use of drugs.
Levels of use of five substances (heroin, cocaine, methamphetamine, marijuana, and alcohol) were each measured in terms of number of days per month of use. For each substance, available monthly measures were averaged over annual periods beginning at initiation of the reported primary drug. The current analysis used data from the first 10 years following initiation of the primary drug. The primary drug was self-identified, either as a basis for treatment admission and a recruitment criterion for the study or as part of the interview process. These five substances are the most common substances for treatment admission in California (CA ADP, 2007).
Other measures for sample description included selected user characteristics (e.g., age, gender, race/ethnicity), drug use history (ages of initiation and regular use), drug treatment history (age of initial treatment, cumulative months of treatment for the entire period), and criminal history (age at first arrest, months incarcerated).
2.4 Analyses
For each of the three primary drug subsamples (heroin, cocaine, meth), a random effects growth model was estimated using Mplus (Muthen and Muthen, 2007). Models included random intercept and slope parameters for all five substances (i.e. patterns for each of five substances over time) as well as variance and covariance parameters among intercepts and slopes. From these models, covariances between slope parameters can be interpreted as indicating whether the directions of change in use of other substances parallel or differ from that of the primary drug. To further explore the relationships of levels of use of the various substances across time, a second set of growth models were estimated. This second set of models (one for each primary drug) included random intercept and slope parameters for the primary drug, with levels of use of the other substances considered as time-dependent covariates. Thus, there were parameters indicating the relationship of the level of use of the primary drug with levels of use of each of the other substances at each of the 10 observations across time.
3. Results
3.1 Sample Description
The combined sample was 73% male, and 34% white, 32% African American, 30% Hispanic, and 4% Asian or other racial/ethical groups. The average age of initiation into use of the primary drug use was 20.7 years (standard deviation=6.1) with regular use beginning at an average age of 22.9 (sd=6.9). The average age of first drug treatment was 28.9 years (sd=7.6), and the average time in treatment during the first 10 years of primary substance use was 4.5 months (sd=9.3). Criminal involvement resulted in an average of 17.3 months (sd=24.1) in prison or jail during the first 10 years of primary substance use.
3.2 Levels of Use of Primary and Other Substances
The trajectories of average number of days per month with use of each of the five substances appear in Figure 1 for each of the primary drug subsamples: heroin, cocaine, and meth. Results show that there was very low usage of non-primary heroin, cocaine, or meth measured during periods concurrent with use of these primary drugs. For primary heroin users, usage of cocaine or meth averaged less than 1.5 days per month across the entire period. Likewise, for primary cocaine users, usage levels of heroin or meth were low, averaging less than one day per month; and for primary meth users, heroin usage was at that same very low level. Cocaine usage by primary meth users was slightly higher, at around 2.5–3.0 days per month.
Figure 1.
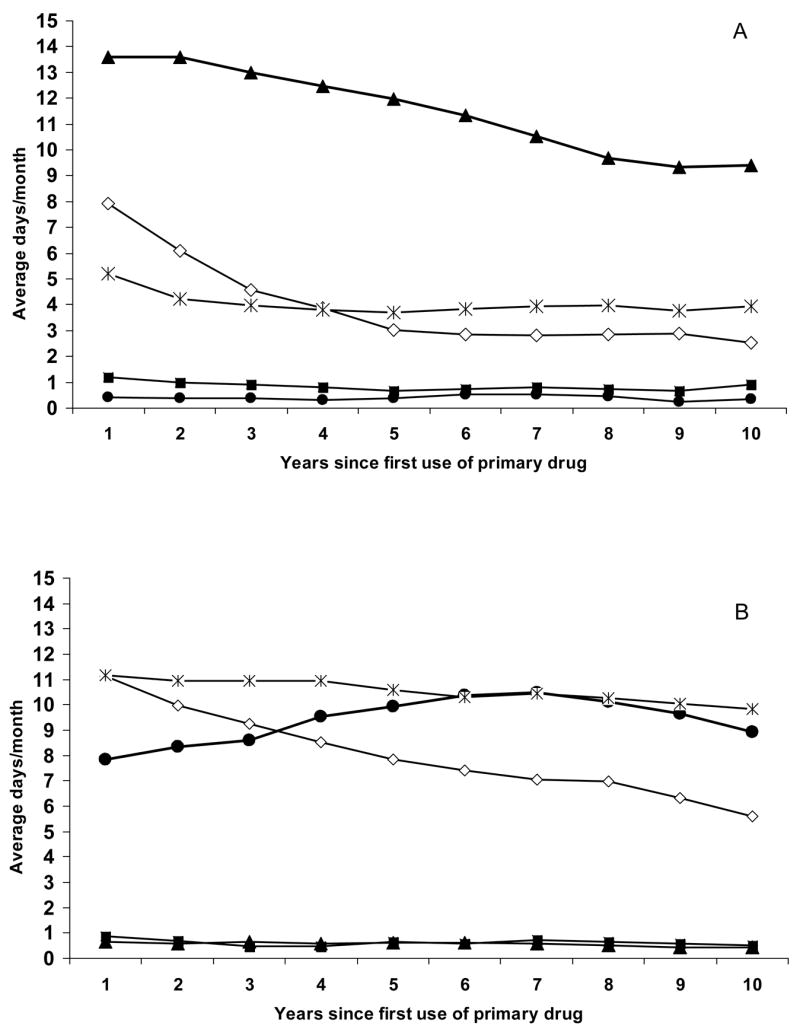

Observed Average Number of Days per Month of Use of Five Substances by Primary Drug Subsample. A) Primary Heroin Users (N=629). B) Primary Cocaine Users (N=724). C) Primary Methamphetamine Users (N=474)
However, for users of all three primary drugs, their concurrent usage of marijuana and alcohol was consistently at a moderate level. The biggest discrepancy between usage of the primary drug and other substances occurred for primary heroin users, with alcohol and marijuana quite low at 3–4 days per month after the first two years. For primary cocaine users, alcohol use was actually higher than their primary cocaine use for most of the 10-year period; and marijuana usage, while less than that of cocaine for most of the observation period, was still at moderate levels of 7–11 days per month. For primary meth users, alcohol and marijuana use was at a moderate level of about 6–11 days per month across the observation period, but lower than the reported levels of meth use.
3.3 Differing Trajectories of Use across Time
Results in Table 1 show the estimated trajectories and relationships across drugs for each of the primary drug subsamples. Results show that for heroin users their use of their primary drug generally declined across the 10-year observation period (slope=−0.56), while no significant pattern of linear change occurred in their cocaine, meth, or alcohol use. While their marijuana use also declined overall (slope=−0.38), the decrease was at a lower rate than for heroin, resulting in a significant negative covariance between the slopes (−0.28). For cocaine users, use of their primary drug showed no significant linear trend over time, and their use of heroin and meth remained at consistently low levels; but their use of marijuana and alcohol declined significantly over time (slopes=−0.59 and −0.21, respectively). For meth users, use of their primary substance declined (slope=−0.58), as did their use of cocaine (slope=−0.15), marijuana (slope=−0.72), and alcohol (slope=−0.25), while their use of heroin remained at consistently low levels.
Table 1.
Results of growth model estimation for use of five substances over a 10-year period following initiation of primary drug1
| Primary Drug2 | ||||
|---|---|---|---|---|
| Parameters | Heroin (N=629) | Cocaine (N=694) | Methamphetamine (N=474) | |
| Regression coefficients3 | ||||
| Heroin | Intercept | 14.56* | 0.70* | 0.34 |
| Slope | −0.56* | −0.03 | 0.02 | |
| Cocaine | Intercept | 0.45* | 8.36* | 2.97* |
| Slope | −0.02 | 0.14 | −0.15* | |
| Methamphetamine | Intercept | 1.01* | 0.63* | 13.61* |
| Slope | −0.03 | −0.01 | −0.58* | |
| Marijuana | Intercept | 5.86* | 11.04* | 11.74* |
| Slope | −0.38* | −0.59* | −0.72* | |
| Alcohol | Intercept | 4.40* | 11.46* | 8.94* |
| Slope | −0.08 | −0.21* | −0.25* | |
| Covariances of slopes across substances4 | ||||
| Heroin | Cocaine | 0.03 | 0.06 | −0.03 |
| Methamphetamine | −0.01 | −0.01 | −0.11 | |
| Marijuana | −0.28* | −0.04 | −0.01 | |
| Alcohol | −0.10 | −0.03 | −0.01 | |
| Cocaine | Methamphetamine | −0.01 | −0.09 | −0.23 |
| Marijuana | 0.03* | −0.19 | −0.10 | |
| Alcohol | −0.003 | 0.47* | 0.19* | |
| Methamphetamine | Marijuana | 0.12* | 0.06 | 0.35* |
| Alcohol | 0.06* | 0.02 | 0.31* | |
| Marijuana | Alcohol | 0.11* | 0.52* | 0.39* |
p<.01
Results are from multiple trajectory growth models; parameters included random intercept and slope for each of five substances, plus their variances and covariances.
Each column represents a separate analysis (of the specified primary drug subsample).
Interpret the parameter estimates as regression coefficients. Note that all variance parameters for intercept and slope were significant at p<.01 and are not shown in the table.
Interpret the parameter estimates as relationships between slopes of growth curves for the different pairs of drugs (e.g. the slope of heroin use pattern with the slope of cocaine use pattern). Note that all intercept-with-slope covariances for each drug were negative and significant at p<.01 and are not shown in the table.
3.4 Associations of Levels of Use between Substances
Table 2 displays estimates of relationships between levels of use for pairs of substances at each year of the drug histories. Note that coefficients can be interpreted similarly to correlation coefficients. Results showed that for primary heroin users, higher levels of their heroin use were associated with higher levels of alcohol use beginning at year 5 of the observation period (significant positive coefficient of 0.21), with the relationship continuing through year 10. Their levels of heroin use were also associated with levels of cocaine use in years 4 and 6–8. There was no relationship of levels of their heroin use with meth use. The relationship with marijuana use was inconsistent, negative at the beginning of the period (year 1) and positive toward the end of the period (in year 9).
Table 2.
Further exploration of patterns of use of five drugs over a 10 year period: relationships of levels of use at each year1
| Primary Drug2 | |||
|---|---|---|---|
| Time-dependent covariate (i.e. level of non-primary substance use at each time period)3 | Heroin (N=629) | Cocaine (N=694) | Methamphetamine (N=474) |
| Year 1 | |||
| Heroin | -- | −0.05 | 0.30 |
| Cocaine | 0.13 | -- | −0.07 |
| Methamphetamine | 0.06 | 0.06 | -- |
| Marijuana | −0.12* | −0.09* | 0.21* |
| Alcohol | −0.01 | 0.22* | 0.22* |
| Year 2 | |||
| Heroin | -- | 0.08 | 0.40 |
| Cocaine | 0.18 | -- | −0.10 |
| Methamphetamine | 0.07 | 0.01 | -- |
| Marijuana | −0.04 | −0.08* | 0.23* |
| Alcohol | 0.01 | 0.23* | 0.23* |
| Year 3 | |||
| Heroin | -- | 0.10 | 0.16 |
| Cocaine | 0.09 | -- | −0.15 |
| Methamphetamine | 0.09 | −0.09 | -- |
| Marijuana | −0.04 | −0.02 | 0.26* |
| Alcohol | 0.07 | 0.23* | 0.28* |
| Year 4 | |||
| Heroin | -- | 0.19 | 0.04 |
| Cocaine | 0.44* | -- | −0.13 |
| Methamphetamine | 0.10 | −0.26 | -- |
| Marijuana | −0.01 | −0.01 | 0.27* |
| Alcohol | 0.14 | 0.27* | 0.29* |
| Year 5 | |||
| Heroin | -- | 0.20 | 0.13 |
| Cocaine | 0.31 | -- | −0.10 |
| Methamphetamine | −0.03 | −0.24* | -- |
| Marijuana | 0.04 | 0.02 | 0.27* |
| Alcohol | 0.21* | 0.32* | 0.27* |
| Year 6 | |||
| Heroin | -- | 0.35* | 0.10 |
| Cocaine | 0.40* | -- | −0.07 |
| Methamphetamine | −0.19 | −0.24 | -- |
| Marijuana | 0.06 | 0.08* | 0.32* |
| Alcohol | 0.25* | 0.34* | 0.27** |
| Year 7 | |||
| Heroin | -- | 0.35* | 0.09 |
| Cocaine | 0.34* | -- | −0.04 |
| Methamphetamine | −0.16 | −0.23* | -- |
| Marijuana | 0.05 | 0.09* | 0.29* |
| Alcohol | 0.27* | 0.37* | 0.30* |
| Year 8 | |||
| Heroin | -- | 0.49* | 0.05 |
| Cocaine | 0.53* | -- | 0.02 |
| Methamphetamine | −0.10 | −0.05 | -- |
| Marijuana | 0.10 | 0.07 | 0.37* |
| Alcohol | 0.22* | 0.38* | 0.27* |
| Year 9 | |||
| Heroin | -- | 0.41* | 0.07 |
| Cocaine | 0.01 | -- | 0.01 |
| Methamphetamine | −0.07 | −0.10 | -- |
| Marijuana | 0.15* | 0.06 | 0.36* |
| Alcohol | 0.22* | 0.40* | 0.31* |
| Year 10 | |||
| Heroin | -- | 0.28 | −0.06 |
| Cocaine | −0.11 | -- | −0.12 |
| Methamphetamine | 0.14 | −0.31 | -- |
| Marijuana | 0.11 | 0.08 | 0.39* |
| Alcohol | 0.33* | 0.38* | 0.32* |
p<.01
Results are from three growth models; parameters included random intercept and slope of primary drug over time and levels of use of non-primary substances as time-dependent covariates.
Each column represents a separate analysis (of the specified primary drug subsample).
Results in the table are estimates of parameters for each time period and indicate the relationship of the level of use of the primary drug to that of each of the non-primary drugs. Note that for simplicity, other parameters in the models are not shown in table (intercept, slope, variance, covariance).
For primary cocaine users, higher levels of primary drug use were associated with higher levels of alcohol use across the entire observation period, higher levels of heroin use in years 6–9, and lower levels of meth use in years 5 and 7. In addition, an inconsistent relationship occurred between levels of cocaine and marijuana use, much like that for heroin users: negative at the outset (years 1–2) and positive later in the observation period (for cocaine users at years 6–7).
For primary meth users, higher levels of meth use were associated consistently with higher levels of alcohol and marijuana. But no significant relationships were seen with levels of heroin or cocaine.
4. Discussion
4.1 Summary
Results show relatively low frequencies of use of non-primary heroin, cocaine, and meth by primary users of these drugs. This suggests that while individuals may differ, group descriptions of primary drug trajectories over time may present valid information about overall use of these three types of drugs. However, results indicate that there are subgroups of these users who do use other drugs; this supports a need for future targeted subgroup examination in order to provide additional detail to guide the development of specialized services for subgroups that continue use of multiple drugs.
While a main conclusion of relatively low levels of non-primary use of heroin, cocaine, and meth is supported for all three primary drug subsamples, their levels of alcohol and marijuana use were considerably higher. This is consistent with prior studies (e.g. Byqvist, 2006; SAMHSA, 2001, 2005). In addition, differences between the primary drug subsamples were seen in their use of alcohol and marijuana. Levels of marijuana and alcohol use were comparable to those of the primary drug for primary cocaine and meth user subsamples. However, primary heroin users had overall levels of alcohol and marijuana use considerably lower than levels of their primary drug and also lower than alcohol and marijuana use by primary cocaine and meth users. Primary cocaine and meth users had almost identical patterns of marijuana use over time, while cocaine users had slightly higher levels of alcohol use than did meth users. The general picture from these analyses remains consistent with continuing concern about polydrug use, at least for subgroups of users and for certain substances (e.g., Community Epidemiology Work Group [CEWG], 2007; SAMHSA, 2005).
Analysis results complement several earlier studies in showing the aggregate picture of use of most substances declining in tandem over time (Darke et al., 2006; DeMaria et al., 2000; Fairbank et al., 1993; Gossop et al., 2002, 2003). Our results showed generally that primary heroin and meth use gradually declined over the 10-year period, whereas cocaine use showed no overall change (although levels increased slightly for five years and then began to decline slightly). Our results were also similar to earlier studies in showing that use of other non-primary drugs (heroin, cocaine, and meth) declined, but there was less decrease or continuing stability in alcohol and marijuana use. The lack of reciprocal trends suggests little switching of drugs for this sample within the 10-year period following initiation of primary drug. Note that while results show overall patterns for the sample, it is important to consider that there are individuals who diverge from the general pattern and may exhibit drug switching (e.g. Bovasso and Cacciola, 2003; Gossop et al., 2002). In addition, patterns may be related to other individual or contextual characteristics; this should be explored in further work.
When examined as time-dependent variables, levels of use of non-primary and primary substances were more often not related than related; that is, more days of use of the primary drug did not necessarily mean more days of use of non-primary substances. However, significant relationships were seen at some specific time points. Days of use of heroin and cocaine were positively related for both primary heroin and cocaine users several years after their initiation of primary substance use, albeit the level of non-primary use of both of these drugs was very low overall. This suggests that for heroin and cocaine users in the earlier phases of their use trajectories, treatment focus on the primary substance may be adequate. However, users with longer use histories may profit from treatment which includes prevention/intervention for other drugs as well. Use of alcohol for cocaine users and use of alcohol and marijuana for meth users, on the other hand, were more consistently positively related to the use of the primary substance. This might suggest users’ desire to counterbalance stimulant effects. Therefore, treatment for cocaine and meth users should also consider addressing alcohol and marijuana use, particularly among those with higher usage levels of the primary drug.
Overall, relationships (when they existed) were usually positive rather than negative between levels of primary and non-primary drug use. Thus, polydrug use in our sample suggests primarily concurrent patterns of use, rather than drug-switching. The differential patterning of the relationships for the primary drug groups, as well as the level of use of non-primary substances, suggest specific intervention targets identifiable through levels of the primary drug; e.g. heroin users later in their use careers (five years or later) with higher levels of heroin use may benefit from attention to their possible cocaine use; cocaine and meth users with higher levels of their primary drug may benefit from interventions related to alcohol and marijuana use at any point in the first 10 years of their primary drug use. But the other sporadically occurring relationships suggest that interventions should always consider the possible subgroups of users who may be using multiple substances during any given period. Future analyses should consider in more detail what individual user characteristics might be associated with specific types, patterns, or timing of polydrug use; e.g. national treatment data suggest more polydrug use among younger age groups (SAMHSA, 2005).
4.2 Limitations
Interpretation of results should occur within the context of limitations of this study. The inclusion of only first-order growth parameters (linear/slope) limits the interpretation to that of general trend over time; further detail in patterns of change within the general trend required complex models whose lack of parsimony resulted in unreliable estimation. While the study considered use of multiple substances within the same observation period, it did not distinguish simultaneity or co-use of drugs (Shensul et al., 2004). Such simultaneous use of multiple substances may distinguish a subset of users whose patterns should be considered in detail in future research. While analysis models included individual trajectory variability, results describe an aggregate picture. Analyses estimated a single summary pattern for use of each substance for each subsample by primary drug. However, it may be that there exist subgroups with different patterns and combinations of patterns. Further analyses can explore this issue in more detail. Interpretation of results is constrained to the 10-year drug use histories used in the analyses. For example, longer-term follow-up with heroin users suggest a continuing decline in use (but at a slowing rate) in later years (Hser et al., 2001). Note also that level of substance use was measured as days of use per month; future analyses should also include detail on frequency and/or quantity of use, particularly for alcohol.
Interpretation should also consider potential limitations of the data sets. Contributing studies were done in California, with most data collected from 1996–2003 (and one study additionally in 1989–91). However, the 10-year trajectories for individual users occurred at different calendar times even within studies. No adjustment was made in the current analyses for contextual effects occurring as a result of the era or decade during which the user initiated the primary drug. Note, however, that while treatment admission fractions have shifted across primary drugs, polydrug use reported at treatment admission has changed little in California during the past 15 years (Brecht et al., 2005; CA ADP, 2007). Polydrug use may differ geographically, so the California data may not represent national trends or other specific geographic locations (CEWG, 2007). The studies were quasi-experimental as opposed to clinical trials. The data represent trajectories of substance use for individuals who were sampled because of their drug treatment participation or who self-identified a primary drug problem; thus, the results do not reflect substance use patterns for a general population. In addition, there may be selection factors influencing choice of primary drug that may, in turn, influence longitudinal patterns of both primary and non-primary drugs; selection models could be incorporated into future analyses.
4.3 Conclusions
In summary, analyses support the validity of longitudinal analysis results relating to drug use over time based on classification by use of primary drug for heroin, cocaine, and meth users. Use of the non-primary drugs (of heroin, cocaine, and meth) were at considerably lower levels than the primary drug across the entire trajectories, and use levels of alcohol and marijuana varied across the primary drug subgroups. Relationships between trajectories suggest general declines (more or less in tandem) or consistent levels across the various substances. However, future focus on individuals who diverge from the general patterns may be helpful in identifying strategies for prevention or intervention.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Anglin MD, Hser YI, Chou CP. Reliability and validity of retrospective behavioral self-report by narcotics addicts. Eval Rev. 1993;17:90–107. [Google Scholar]
- Beswick T, Best D, Rees S, Coomber R, Gossop M, Strang J. Multiple drug use: patterns and practices of heroin and crack use in a population of opiate addicts in treatment. Drug Alcohol Rev. 2001;20:201–204. [Google Scholar]
- Booth B, Leukefeld C, Falck R, Wang J, Carlson R. Correlates of rural methamphetamine and cocaine users: results from a multistate community study. J Stud Alcohol. 2006;67:493–501. doi: 10.15288/jsa.2006.67.493. [DOI] [PubMed] [Google Scholar]
- Bovasso G, Cacciola J. The long-term outcomes of drug use by methadone maintenance patients. J Behav Health Serv Res. 2003;30:290–303. doi: 10.1007/BF02287318. [DOI] [PubMed] [Google Scholar]
- Brecht ML, Greenwell L, Anglin MD. Methamphetamine treatment: trends and predictors of retention of completion in a large state treatment system 1992–2002. J Subst Abuse Treat. 2005;29:295–306. doi: 10.1016/j.jsat.2005.08.012. [DOI] [PubMed] [Google Scholar]
- Brecht M-L, O’Brien A, Mayrhauser C, Anglin MD. Methamphetamine use behaviors and gender differences. Addict Behav. 2004;29:89–106. doi: 10.1016/s0306-4603(03)00082-0. [DOI] [PubMed] [Google Scholar]
- Byqvist S. Patterns of drug use among drug misusers in Sweden. Gender Differences Subst Use Misuse. 2006;41:1817–1835. doi: 10.1080/10826080601006805. [DOI] [PubMed] [Google Scholar]
- California Department of Alcohol and Drug Programs (CA ADP) California Outcomes Measurement System: Treatment Admissions, Substance Use. Sacramento, CA: CA Dept. of Alcohol and Drug Programs; 2007. [Accessed on 12/17/07]. Available at http://www.adp.ca.gov/oara/pdf/AOD_Use.pdf. [Google Scholar]
- Chou CP, Hser Y-I, Anglin MD. Pattern reliability of narcotics addicts’ self reported data: A confirmatory assessment of construct validity and consistency. Subst Use Misuse. 1996;31:1189–1216. doi: 10.3109/10826089609063972. [DOI] [PubMed] [Google Scholar]
- Community Epidemiology Work Group (CEWG) Epidemiologic Trends in Drug Abuse. Bethesda, MD: National Institutes of Drug Abuse; 2007. [Accessed 12/17/07]. Available at http://www.drugabuse.gov/PDF/CEWG/Vol1_107.pdf. [Google Scholar]
- Darke S, Hall W. Levels and correlates of polydrug use among heroin users and regular amphetamine users. Drug Alcohol Depend. 1995;39:231–235. doi: 10.1016/0376-8716(95)01171-9. [DOI] [PubMed] [Google Scholar]
- Darke S, Ross J, Teesson M. The Australian Treatment Outcome Study ATOS: what have we learnt about treatment for heroin dependence? Drug Alcohol Rev. 2007;26:49–54. doi: 10.1080/09595230601036986. [DOI] [PubMed] [Google Scholar]
- Darke S, Williamson A, Ross J, Teesson M. Reductions in heroin use are not associated with increases in other drug use: 2-year findings from the Australian Treatment Outcome Study. Drug Alcohol Depend. 2006;84:201–205. doi: 10.1016/j.drugalcdep.2006.03.004. [DOI] [PubMed] [Google Scholar]
- DeMaria P, Sterling R, Weinstein S. The effect of stimulant and sedative use on treatment outcome of patients admitted to methadone maintenance treatment. Am J Addict. 2000;9:145–155. doi: 10.1080/10550490050173217. [DOI] [PubMed] [Google Scholar]
- Downey K, Helmus T, Schuster C. Treatment of heroin-dependent poly-drug abusers with contingency management and buprenorphine maintenance. Exp Clin Psychopharmacol. 2000;8:176–184. doi: 10.1037//1064-1297.8.2.176. [DOI] [PubMed] [Google Scholar]
- Earleywine M, Newcomb M. Concurrent versus simultaneous polydrug use; prevalence, correlates, discriminant validity, and prospective effects on health outcomes. Exp Clin Psychopharmacol. 1997;5:353–364. doi: 10.1037//1064-1297.5.4.353. [DOI] [PubMed] [Google Scholar]
- Epstein D, Preston D. Does cannabis use predict poor outcome for heroin-dependent patients on maintenance treatment? Past findings and more evidence against. Addiction. 2003;98:269–279. doi: 10.1046/j.1360-0443.2003.00310.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fairbank J, Dunteman G, Condelli W. Do methadone patients substitute other drugs for heroin? Predicting substance use at 1-year follow-up. Am J Drug Alcohol Abuse. 1993;19:465–474. doi: 10.3109/00952999309001635. [DOI] [PubMed] [Google Scholar]
- Flannery B, Morgenstern J, McKay J, Wechsberg W, Litten R. Co-occurring alcohol and cocaine dependence: recent findings from clinical and field studies. Alcohol Clin Exp Res. 2004;28:976–981. doi: 10.1097/01.alc.0000128232.30331.65. [DOI] [PubMed] [Google Scholar]
- Gossop M. A web of dependence. Addiction. 2001;96:677–678. doi: 10.1046/j.1360-0443.2001.9656771.x. [DOI] [PubMed] [Google Scholar]
- Gossop M, Manning V, Ridge G. Concurrent use of alcohol and cocaine: differences in patterns of use and problems among users of crack cocaine and cocaine powder. Alcohol Alcohol. 2006;41:121–125. doi: 10.1093/alcalc/agh260. [DOI] [PubMed] [Google Scholar]
- Gossop M, Marsden J, Stewart D, Kidd T. Changes in use of crack cocaine after drug misuse treatment: 4–5 year follow-up results from the National Treatment Outcome Research Study NTORS. Drug Alcohol Depend. 2002;66:21–28. doi: 10.1016/s0376-8716(01)00178-8. [DOI] [PubMed] [Google Scholar]
- Gossop M, Marsden J, Stewart D, Kidd T. The National Treatment Outcome Research Study NTORS: 4–5 year follow-up results. Addiction. 2003;98:291–303. doi: 10.1046/j.1360-0443.2003.00296.x. [DOI] [PubMed] [Google Scholar]
- Grella C, Anglin MD, Wugalter S. Patterns and predictors of cocaine and crack use by clients in standard and enhanced methadone maintenance treatment. Am J Drug Alcohol Abuse. 1997;23:15–42. doi: 10.3109/00952999709001685. [DOI] [PubMed] [Google Scholar]
- Grella C, Anglin MD, Wugalter S. Cocaine and crack use and HIV risk behavior among high-risk methadone maintenance clients. Drug Alcohol Depend. 1995;37:15–21. doi: 10.1016/0376-8716(94)01059-t. [DOI] [PubMed] [Google Scholar]
- Hser YI, Anglin MD, Chou CP. Reliability of retrospective self-report by narcotics addicts. Psychol Assess. 1992;4:207–213. [Google Scholar]
- Hser YI, Hoffman V, Grella CE, Anglin MD. A 33-year follow-up of narcotics addicts. Arch Gen Psychiatry. 2001;58:503–508. doi: 10.1001/archpsyc.58.5.503. [DOI] [PubMed] [Google Scholar]
- Hser YI, Stark ME, Paredes A, Huang D, Anglin MD, Rawson R. A 12-year follow-up of a treated cocaine-dependent sample. J Subst Abuse Treat. 2006;30:219–26. doi: 10.1016/j.jsat.2005.12.007. [DOI] [PubMed] [Google Scholar]
- Hser YI, Huang D, Teruya C, Anglin MD. Diversity of drug abuse treatment utilization patterns and outcomes. Evaluation and Program Planning. 2004;27:309–319. [Google Scholar]
- Hser YI, Huang D, Teruya C, Anglin MD. Gender differences in drug abuse treatment outcomes and correlates. Drug Alcohol Depend. 2003;72:255–264. doi: 10.1016/j.drugalcdep.2003.07.005. [DOI] [PubMed] [Google Scholar]
- Hser Y-I, Evans E, Huang D, Brecht M-L, Li L. Comparing the dynamic course of heroin, cocaine, and methamphetamine use over 10 years. doi: 10.1016/j.addbeh.2008.07.024. Under review. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hubbard R, Craddock S, Flynn P, Anderson J, Etheridge R. Overview of 1 year follow-up outcomes in the Drug Abuse Treatment Outcome Study DATOS. Psychol Addict Behav. 1997;11:261–278. [Google Scholar]
- John D, Kwiatkowski C, Booth R. Differences among out-of-treatment drug injectors who use stimulants only, opiates only or both: implications for treatment entry. Drug Alcohol Depend. 2001;64:165–172. doi: 10.1016/s0376-8716(01)00120-x. [DOI] [PubMed] [Google Scholar]
- Jones C, Weatherburn D. Reducing cannabis consumption. Crime and Justice Bulletin, NSW Bureau of Crime Statistics and Research. No.60; November, 1–8.2001. [Google Scholar]
- Kenna G, Nielsen D, Mello P, Schiesl A, Swift R. Pharmacotherapy of dual substance abuse and dependence. CNS Drugs. 2007;21:213–237. doi: 10.2165/00023210-200721030-00003. [DOI] [PubMed] [Google Scholar]
- Leri F, Bruneau J, Stewart J. Understanding polydrug use: review of heroin and cocaine co-use. Addiction. 2003;98:7–22. doi: 10.1046/j.1360-0443.2003.00236.x. [DOI] [PubMed] [Google Scholar]
- Leri F, Stewart J, Fischer B, Jurgen R, Marsh D, Brissette S, Bruneau J, El-Guebaly N, Noel L, Tyndall M, Wild TC. Patterns of opioid and cocaine co-use: A descriptive study in a Canadian sample of untreated opioid-dependent individuals. Exp Clin Psychopharmacol. 2005;13:303–310. doi: 10.1037/1064-1297.13.4.303. [DOI] [PubMed] [Google Scholar]
- McCabe S, Cranford J, Morales M, Young A. Simultaneous and concurrent polydrug use of alcohol and prescription drugs: prevalence, correlates, and consequences. J Stud Alcohol. 2006;67:529–537. doi: 10.15288/jsa.2006.67.529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGlothlin WH, Anglin MD, Wilson BD. A follow-up of admissions to the California Civil Addict Program. Am J Drug Alcohol Abuse. 1977;4:179–199. doi: 10.3109/00952997709002759. [DOI] [PubMed] [Google Scholar]
- Malcolm B, Hesselbrock M, Segal B. Multiple substance dependence and course of alcoholism among Alaska Native Men and Women. Subst Use Misuse. 2006;51:729–741. doi: 10.1080/10826080500391803. [DOI] [PubMed] [Google Scholar]
- Martin C, Clifford P, Maisto S, Earleywine M, et al. Polydrug use in an inpatient treatment sample of problem drinkers. Alcohol Clin Exp Res. 1996;20:413–417. doi: 10.1111/j.1530-0277.1996.tb01067.x. [DOI] [PubMed] [Google Scholar]
- Medina K, Shear P. Anxiety, depression, and behavioral symptoms of executive dysfunction in ecstasy users: contributions of polydrug use. Drug Alcohol Depend. 2007;87:303–311. doi: 10.1016/j.drugalcdep.2006.09.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthen B, Muthen L. Mplus, User’s Guide, Version 4.1. Los Angeles: Muthen & Muthen; 2007. [Google Scholar]
- Nurco DN, Bonito AJ, Lerner M, Balter M. Studying addicts over time: Methodology and preliminary findings. Am J Drug Alcohol Abuse. 1975;2:183–196. doi: 10.3109/00952997509002733. [DOI] [PubMed] [Google Scholar]
- Patterson T, Semple S, Zians J, Strathdee S. Methamphetamine-using HIV-positive men who have sex with men: correlates of polydrug use. J Urban Health. 2005;82(Supplement 1):i120–126. doi: 10.1093/jurban/jti031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prendergast M, Podus D, Chang E, Urada D. The effectiveness of drug abuse treatment: a meta-analysis of comparison group studies. Drug Alcohol Depend. 2002;67:53–73. doi: 10.1016/s0376-8716(02)00014-5. [DOI] [PubMed] [Google Scholar]
- Substance Abuse and Mental Health Services Administration (SAMHSA) The DASIS Report, Polydrug Use Among Treatment Admissions: 1998. Rockville, MD: SAMHSA; 2001. October 5, 2001. [Accessed 12/18/07]. Available at http://www.oas.samhsa.gov/2k1/polydrugTX/polydrugTX.pdf. [Google Scholar]
- Substance Abuse and Mental Health Services Administration (SAMHSA) Rockville, MD: SAMHSA; 2005. March 25, 2005. [Accessed 12/18/07]. The DASIS Report, Polydrug Admissions: 2002. Available at http://www.oas.samhsa.gov/2k5/polydrugTX/polydrugTX.pdf. [Google Scholar]
- Substance Abuse and Mental Health Services Administration (SAMHSA) Rockville, MD: SAMHSA; 2007. [Accessed 12/18/07]. Treatment Episode Data Set (TEDS): 1995–2005. National Admissions to Substance Abuse Treatment Services, DASIS Series: S-37, DHHS Publication No. (SMA) 07–4234. Available at http://wwwdasis.samhsa.gov/teds05/tedsad2k5web.pdf. [Google Scholar]
- Schensul J, Convey M, Burkholder G. Challenges in measuring concurrency, agency and intentionality in polydrug research. Addict Behav. 2005;30:571–574. doi: 10.1016/j.addbeh.2004.05.022. [DOI] [PubMed] [Google Scholar]
- Simpson D, Joe G, Broome K. A national 5-year follow-up of treatment outcomes for cocaine dependence. Arch Gen Psychiatry. 2002;59:538–544. doi: 10.1001/archpsyc.59.6.538. [DOI] [PubMed] [Google Scholar]
- Sumnall H, Wagstaff G, Cole J. Self-reported psychopathology in polydrug users. J Psychopharmacol. 2004;18:75–82. doi: 10.1177/0269881104040239. [DOI] [PubMed] [Google Scholar]
- Topp L, Day C, Degenhardt L. Changes in patterns of drug injection concurrent with a sustained reduction in the availability of heroin in Australia. Drug Alcohol Depend. 2003;70:275–286. doi: 10.1016/s0376-8716(03)00013-9. [DOI] [PubMed] [Google Scholar]
- Williamson A, Darke S, Ross J, Teesson M. The effect of persistence of cocaine use on 12-month outcomes for the treatment of heroin dependence. Drug Alcohol Depend. 2006;81:293–300. doi: 10.1016/j.drugalcdep.2005.08.010. [DOI] [PubMed] [Google Scholar]