

Abstract
Background:
Several recent studies have demonstrated that microRNAs (miRNAs) are stably detectable in plasma/serum. We tested miR-221 and miR-375, which are frequently reported to be highly and poorly expressed in pancreatic cancer (PCa), as candidates for plasma biomarkers in PCa.
Methods:
This study was divided into three parts: (1) Confirmation of higher miR-221 levels in primary PCa tissue and cell lines than normal pancreatic tissues. (2) Evaluation of plasma miR-221 and miR-375 concentrations by comparing results from 47 consecutive PCa patients and 30 healthy volunteers. (3) Evaluation of the assay for monitoring tumour dynamics in PCa patients.
Results:
(1) Expression of miR-221 was significantly higher in PCa tissues and cell lines than normal pancreatic tissues. (2) Plasma miR-221 concentrations were significantly higher in PCa patients than that in benign pancreatic tumours (P=0.016) and controls (P<0.0005), while plasma miR-375 concentrations tended to be lower in PCa patients (P=0.064), and the miR-221/miR-375 ratio was significantly higher (P<0.0001) in PCa patients than in controls. (3) Plasma miR-221 concentrations were significantly reduced in postoperative samples (P=0.018). Furthermore, PCa patients with high plasma miR-221 concentrations had significant correlation with distant metastasis (P=0.041), and non-resectable status (P=0.021).
Conclusion:
Plasma miR-221 could be a useful biomarker for cancer detection, monitoring tumour dynamics and predicting malignant outcomes in PCa patients, and may contribute to clinical decision making in PCa treatments.
Keywords: pancreatic cancer, microRNA, plasma, biomarker
Pancreatic cancer (PCa) is the fifth leading cause of cancer death in Japan and the fourth leading cause of cancer-related death in the United States (Hirata et al, 2007; Jemal et al, 2009). Recent improvements in surgical techniques and perioperative management have reduced operation-related death during perioperative periods; however, PCa still has extremely poor prognosis. Even now, median survival is 5–8 months and a 5-year survival rate is <5% because PCa develops local invasiveness and metastases to distant organs in the early stage of clinical course (Heinemann et al, 2008; Sultana et al, 2008; Jemal et al, 2009). Although curative pancreatectomy for PCa has been one of the most aggressive surgeries among digestive cancers, the only chance for cure is surgical resection with macroscopic tumour clearance. Nonetheless, <20% of patients could obtain the benefit of curative resection (Bilimoria et al, 2007; Jemal et al, 2009). Therefore, primary tumours must be detected at an early stage with curative intent to improve survival rates, and patients with advanced disease must be diagnosed preoperatively to avoid impairments in quality of life, although chemotherapy or chemoradiotherapy remain the only treatment choices for these patients (Shrikhande et al, 2007).
Since identifying molecular targets for PCa treatment may help to improve the survival of patients with this lethal disease, several studies have attempted to determine the biological factors involved in the malignant potential of PCa (Thayer et al, 2003; Jones et al, 2008). In clinical settings, however, few cancer-associated molecules have been assayed as therapeutic and/or diagnostic biomarkers. Conventional serum tumour markers, such as carcinoembryonic antigen and carbohydrate antigen 19-9 (CA19-9), have been used as convenient diagnostic assays (Satake et al, 1985) for early detection and monitoring tumour status of PCa. These serum tumour markers, however, lack sufficient sensitivity and specificity to facilitate the early detection of cancer. Therefore, the importance of detecting novel biomarkers using a less invasive diagnostic assay for PCa should be emphasised.
MicroRNAs (miRNAs), which are small non-coding RNAs, regulate the translation of specific protein-coding genes. Since their discovery in 1993 (Lee et al, 1993), altered expressions of miRNAs have been associated with several diseases, and tumour miRNAs are involved in tumourigenesis and the development of various cancers. In recent years, several studies have shown that miRNAs are detectable in plasma/serum (Calin and Croce, 2006; Chen et al, 2008; Filipowicz et al, 2008). Mitchell et al (2008) clearly demonstrated that circulating miRNAs originate from cancerous tissues and are protected from endogenous RNase activity by unknown mechanisms. Tumour-derived miRNAs are resistant to endogenous ribonuclease activity because these may be binding some protein, such as the Argonaute 2 protein and high-density lipoproteins (Arroyo et al, 2011; Vickers et al, 2011), or packaged by some kinds of secretory particles including apoptotic bodies and exosomes in plasma/serum (Hasselmann et al, 2001; Mitchell et al, 2008; Cocucci et al, 2009; Kosaka et al, 2010). Therefore, miRNAs can be present in a remarkably stable form (Mitchell et al, 2008; Zhu and Fan, 2011) and the expression level of serum miRNAs is reproducible and consistent among individuals (Chen et al, 2008; Mitchell et al, 2008). Furthermore, secretory vesicles including miRNAs can function as intercellular transmitters (Valadi et al, 2007; Skog et al, 2008).
Concerning PCa, some researchers including us have reported the potential utility in the clinical application of circulating miRNAs such as miR-16, miR-18a, miR-21, miR-155, miR-196a, and miR-210 (Wang et al, 2009; Ho et al, 2010; Morimura et al, 2011; Liu et al, 2012). These circulating miRNAs may be somewhat valuable to PCa detection; however, they were insufficient to predict malignant potential and resectability of PCa. In clinical settings, the clinical behaviours of this lethal disease are extremely important in decision making for patients with PCa. However, to date, there have been no reports on clinically useful roles of circulating miRNAs in plasma/serum of patients with PCa.
In this study, we tested miR-221 and miR-375 (Bloomston et al, 2007; Lee et al, 2007), which have been frequently reported to be highly and poorly expressed in PCa, respectively. In particular, miR-221 has an oncogenic function in various tumours, with its elevation either being caused by genome amplification or transcriptional activation. Also, in primary PCa tissue or PCa cell lines, several researchers have reported overexpression of miR-221 (Volinia et al, 2006; Lee et al, 2007; Szafranska et al, 2007). Therefore, we hypothesised that circulating miR-221 could be detected in plasma and predict tumour characteristics, which could contribute to decision making for PCa treatment. Consequently, we clearly demonstrated that preoperative miR-221 concentrations in plasma are useful to detect PCa, monitor tumour dynamics, and predict distant metastasis and resectability. Our results provided evidence that plasma levels of miR-221 contribute to clinical decision making in PCa treatments to a clinically satisfactory degree.
Materials and methods
Patients and samples
The study was approved by the Institutional Review Board of both Kyoto Prefectural University of Medicine and Kyoto Second Red Cross Hospital, and each subject provided signed informed consent. Between January 2010 and November 2011, 47 plasma samples of consecutive PCa patients and 30 control samples were collected at Kyoto Prefectural University of Medicine and Kyoto Second Red Cross Hospital. Patient characteristics with respect to age, sex, histopathology, and stages of disease are described in Supplementary Table S1. Preoperative plasma samples were collected from 47 patients with PCa, including 37 who underwent pancreatectomy, 10 non-resectable patients, including 7 patients who underwent only gastrointestinal bypass, and 3 non-operative patients, who had advanced disease. Eleven patients underwent chemotherapy before collecting plasma samples. No patients underwent chemoradiotherapy. All patients were pathologically diagnosed as having PCa using surgical specimens or biopsies. Two patients were diagnosed with adenosquamous carcinoma, one patient with anaplastic carcinoma, one patient with intraductal papillary-mucinous carcinoma, and one patient with endocrine cell carcinoma. The remaining 42 patients were diagnosed with adenocarcinoma.
From the patients who underwent surgery, a total of 18 PCa specimens were collected. We also collected five normal tissue specimens from an adjacent benign pancreatic tumour resected as other pancreatic disease, such as insulinoma, in order to exclude the influence of atypical or precancerous status of pancreas tissue on the assay. As a control, plasma was collected from 30 volunteers. Volunteers were medical personnel and hospitalised patients with benign disease such as an inguinal hernia. They underwent medical examinations and did not have any pancreatic disease or other cancerous disease. The stage of tumours was assessed according to the Union for International Cancer Control classification (Sobin and Wittekind, 2009).
Collection of heparin-treated blood plasma and pancreatic tissue
Blood was collected from patients and controls in sodium heparin tubes (BD Vacutainer, Franklin Lakes, NJ, USA) and immediately subjected to the three-spin protocol (1500 r.p.m. for 30 min, 3000 r.p.m. for 5 min, and 4500 r.p.m. for 5 min) to prevent contamination by cellular nucleic acids. Plasma samples were then stored at −80 °C until further processing. All resected specimens were fixed in formalin and embedded in paraffin for pathological diagnosis. Tissues adjacent to specimens were evaluated histologically according to the criteria of the World Health Organization. In all cases, two pathologists were in agreement regarding pathological features and both confirmed diagnoses.
RNA extraction
Total RNA was extracted from cultured cells and 400 μl of plasma using a mirVana PARIS Kit (Ambion, Austin, TX, USA) and eluted into 100 μl of preheated (95 °C) Elution Solution according to the manufacturer's directions. For formalin-fixed paraffin-embedded tissues, total RNA was extracted from four slices 15 μm thick (total thickness of 60 μm) using a RecoverAll Total Nucleic Acid Isolation Kit (Ambion), and eluted finally into 60 μl of Elution Solution according to the manufacturer's instructions.
Protocol for the detection of miRNAs
The amounts of miRNAs were quantified in duplicate via quantitative RT–PCR using the human TaqMan MicroRNA Assay Kit (Applied Biosystems, Foster City, CA, USA). The reverse transcription reaction was carried out with a TaqMan MicroRNA Reverse Transcription Kit (Applied Biosystems) in 15 μl containing 5 μl of RNA extract, 0.15 μl of 100 mℳ dNTPs, 1 μl of Multiscribe Reverse Transcriptase (50 U μl−1), 1.5 μl of 10 × Reverse Transcription Buffer, 0.19 μl of RNase inhibitor (20 U μl−1), 3 μl of gene-specific primer, and 4.16 μl of Nuclease-free water. For the synthesis of cDNA, reaction mixtures were incubated at 16 °C for 30 min, at 42 °C for 30 min, and at 85 °C for 5 min and then held at 4 °C. Next, 1.33 μl of cDNA solution was amplified using 10 μl of TaqMan 2 × Universal PCR Master Mix with no AmpErase UNG (Applied Biosystems), 1 μl of gene-specific primers/probe, and 7.67 μl of nuclease-free water in a final volume of 20 μl. Quantitative PCR was run on a 7300 Real-time PCR system (Applied Biosystems) and reaction mixtures were incubated at 95 °C for 10 min, followed by 40 cycles of 95°C for 15 s, and 60 °C for 1 min. Cycle threshold (Ct) values were calculated with SDS 1.4 software (Applied Biosystems).
The amounts of miRNAs in plasma were calculated on a standard curve constructed with the use of synthetic miRNAs, mirVana miRNA Reference Panel (Ambion). Standard reference miRNAs were amplified for each reaction. However, expression of miRNAs from tissue samples and cultured cells was normalised using the 2−2ΔΔCt method relative to U6 small nuclear RNA (RNU6B). ΔCt was calculated by subtracting the Ct values of RNU6B from the Ct values of the miRNAs of interest. ΔΔCt was then calculated by subtracting the ΔCt of normal pancreatic tissue from the ΔCt of PCa tissues. The change in gene expression was calculated with the equation 2−2ΔΔCt (Livak and Schmittgen, 2001; Pfaffl, 2001).
PCa cell lines and culture
Pancreatic cancer cell lines PK-45H, PANC-1, PK-59 KP4-1, PK-1, and NOR-P1 were purchased from RIKEN Cell Bank (Tsukuba, Japan). NOR-P1 cells were cultured in Dulbecco's Minimum Essential Medium: F12 medium and the others in Roswell Park Memorial Institute (RPMI)-1640 medium (Sigma, St Louis, MO, USA). All media were purchased from Sigma and supplemented with 100 ml l−1 FBS (Trace Scientific, Melbourne, Australia). All cell lines were cultured in 50 ml l−1 carbon dioxide at 37 °C in a humidified chamber.
Statistical analysis
The Mann–Whitney U-test for unpaired data was performed to compare differences in plasma miRNA concentrations and miRNA ratios between cancer patients and healthy volunteers. The Wilcoxon test was used to compare the paired plasma samples obtained before and 1 month after pancreatectomy. A P-value <0.05 was considered significant. The χ2 test or Fisher's exact probability test was used to evaluate correlations between the results of plasma miR-221 concentrations and clinicopathological factors. Receiver-operating characteristic (ROC) curves and the area under the ROC curve (AUC) were used to assess the feasibility of plasma miRNA as a diagnostic tool for detecting PCa. The Younden index was used to determine the cutoff value for the plasma miR-221 concentrations (Akobeng, 2007).
Results
Study design to develop a novel biomarker of plasma miRNA
The study design is summarised in Figure 1A. In this study, we tested an oncogenic miRNA; miR-221 and a tumour suppressive miRNA; miR-375, as candidate targets for this plasma miRNA assay. MiR-221 has been frequently demonstrated to have an oncogenic function in PCa (Volinia et al, 2006; Szafranska et al, 2007; Zhang et al, 2009; Basu et al, 2011). Also, miR-375 was reported to have a tumour suppressive function in PCa (Basu et al, 2011). This study was divided into three parts: (1) Confirmation of higher miR-221 levels in primary PCa tissue and cell lines than normal pancreatic tissues. We compared miR-221 levels between primary pancreas cancer tissues and normal pancreatic tissues. Also, we compared miR-221 levels between PCa cell lines and normal pancreatic tissues. (2) Evaluation of plasma miR-221 concentrations and ratios of miR-221/miR-375 concentrations using quantitative RT–PCR by comparing results from 47 patients with PCa and 30 volunteers. (3) Evaluation of whether plasma miR-221 expression could be used to monitor tumour dynamics by the plasma miR-221 assay in patients with PCa.
Figure 1.

(A) Study design to develop a novel biomarker of plasma miRNA. (B) Expression of miR-221 in PCa tissues. Differential expression of miR-221 in PCa tissues was compared with that in normal tissues by a waterfall plot. Levels of miR-221 were significantly higher in cancer tissues (P=0.005). (C) Expression of miR-221 in PCa cell lines. Differential expression of miR-221 in PCa cell lines was compared with that in normal tissues by a waterfall plot. In pancreatic cell lines, expression levels of miR-221 were significantly higher than those in normal pancreatic tissues (P=0.019). The upper and lower limits of the boxes and the lines inside the boxes indicate the 75th and 25th percentiles and the median, respectively. Upper and lower horizontal bars denote the 90th and 10th percentiles. *Normal means normal pancreatic tissues.
MiR-221 in primary PCa tissues and PCa cell lines
To confirm previously reported high miR-221 expression levels in primary PCa tissue and PCa cell lines (Volinia et al, 2006; Lee et al, 2007; Szafranska et al, 2007), expression of miR-221 in 18 PCa tissues and 5 normal pancreatic tissues was determined by quantitative RT–PCR. Human PCa cell lines, PK-45H, PANC-1, PK-59 KP4-1, PK-1, and NOR-P1 were also evaluated by quantitative RT–PCR. The result of expression levels normalised with RNU6B expression in PCa tissue and PCa cell lines compared with normal pancreas tissue are shown in Figure 1. Expression levels of miR-221 in PCa tissues were significantly higher than those in normal pancreatic tissues (P=0.005) (Figure 1B). Expression levels of miR-221 in PCa cell lines were also significantly higher than those in normal pancreatic tissues (P=0.019) (Figure 1C).
Evaluation of miR-221 and miR-375 expression using quantitative RT–PCR in plasma of PCa patients
Next, we hypothesised that higher miR-221 expression in primary PCa tumours would influence plasma levels of miR-221 in PCa patients. Also, we hypothesised that lower miR-375 expression in primary PCa tumours would influence plasma levels of miR-375 in PCa patients. To evaluate the appropriateness of this assay, we first conducted amplification by real-time RT–PCR of a 10-fold serial dilution of the mirVana miRNA Reference Panel. The linearity of quantitative RT–PCR was confirmed from concentrations of 1 fmol to 0.0001 fmol of each synthetic miRNA, such as miR-221 (y=−3.9005x+11.836; R2=0.9968) and miR-375 (y=−3.7384x+13.242; R2=0.9995) between the logarithm of the amount of input miRNAs and Ct values (Supplementary Figure S1). Although some investigators have determined quantities of plasma miRNAs by comparing internal control miRNAs (Ng et al, 2009; Resnick et al, 2009), it remains controversial which miRNAs are suitable as internal controls for plasma assays. Therefore, we confirmed a linear correlation between the logarithm of the amount of input synthetic miRNA and the cycle threshold value on real-time PCR, as well as the feasibility of extracting total RNA and amplifying specific miRNA in plasma samples. Based on these findings, we utilised the absolute concentration for measuring plasma miRNA in this study.
Using this assay, circulating miRNA, such as miR-221 and miR-375, were detectable in all samples from the 47 PCa patients and 30 volunteers. Plasma concentrations of these two miRNAs in PCa patients were compared with those in normal volunteers by waterfall plots (Figure 2). The plasma concentration of miR-221 in PCa patients was significantly higher than in normal volunteers (P<0.0005) (Figure 2A), and the AUC based on plasma concentrations of miR-221 was 0.743 (Figure 2A). Plasma concentrations of miR-375 tended to be lower in PCa patients than in normal controls (P=0.064) (Figure 2B). The AUC based on plasma concentrations of miR-375 was 0.573 (Figure 2B). These phenomena were also detected in our previous reports (Tsujiura et al, 2010; Komatsu et al, 2011). To investigate more sensitive diagnostic biomarkers in plasma, we analysed the ratio of circulating miRNAs levels, dividing plasma concentrations of miR-221 by these of miR-375, as a combined biomarker (Figure 3). As a result, the ratio of miR-221/miR-375 was significantly higher in PCa patients than that in controls (P<0.0001) (Figure 3A) and the AUC based on the miR-221/miR-375 ratio was 0.762 (Figure 3B). Moreover, although the sample size was small, we found that plasma miR-221 concentrations in patients with pancreatic benign lesions, such as intraductal papillary-mucinous neoplasm (IPMN), serous cystadenoma, and pancreatitis were almost similar to that in healthy volunteers (P=0.539) and significantly lower than that in patients with PCa (P=0.016) (Supplementary Table S2). The sensitivity, specificity, accuracy to distinguish PCa patients from benign tumour patients are 74%, 78%, and 75%, respectively.
Figure 2.

Plasma miR-221 and miR-375 concentrations in 47 consecutive PCa patients and 30 healthy volunteers. (A) Using a real-time RT–PCR assay, circulating miRNA such as miR-221 was detectable in all samples from 47 PCa patients and 30 volunteers. Differential expression of plasma miR-221 with PCa patients was compared with that of normal healthy volunteers by a waterfall plot. Concentrations of miR-221 were significantly higher in plasma from cancer patients than volunteers (P<0.0005). ROC curve analysis in the miR-221 assay for detecting PCa showed a high AUC of 0.743. (B) Plasma concentrations of miR-375 tended to be lower in PCa patients than in normal controls (P=0.092) (B). The AUC based on plasma concentrations of miR-375 was 0.573 (B). Upper and lower limits of the boxes and the lines inside the boxes indicate the 75th and 25th percentiles and the median, respectively. The upper and lower horizontal bars denote the 90th and 10th percentiles.
Figure 3.

Plasma concentration ratios of miR-221/miR-374 in 47 consecutive PCa patients and 30 healthy volunteers. (A) The combined biomarker based on the ratio of miR-221/miR-375 was significantly higher in PCa patients than in controls (P<0.0001). (B) The AUC based on ROC curve analysis of the miR-221/miR-375 ratio was 0.762.
Evaluation of the application of the plasma assay for monitoring tumour dynamics in patients with PCa
We determined a cutoff value of 4.047 × 10−2 amol μl−1 for plasma miR-221 concentration based on the mean value+2 s.d. in healthy volunteer controls to distinguish high miR-221 concentration patients (high group) from low concentration patients (low group). Six patients were categorised into the high group and we compared the expression level of miR-221 between plasma and PCa tissues in each patient of the high group. As a result, in all patients categorised into the high group, expression levels of miR-221 in primary PCa tissues showed higher (100%) than the cutoff value of 1.00 for the miR-221/RNU6B ratio based on the median value in normal pancreatic tissues (Supplementary Table S3). Moreover, we evaluated plasma miR-221 concentrations in paired samples, pre- and postoperative (almost 1 month after surgery) plasma samples from seven PCa patients who underwent curative pancreatectomy, and they were found to be significantly reduced in postoperative samples (P=0.018) (Figure 4). These results indicated that expression levels of plasma miR-221 may reflect tumour dynamics in PCa patients.
Figure 4.
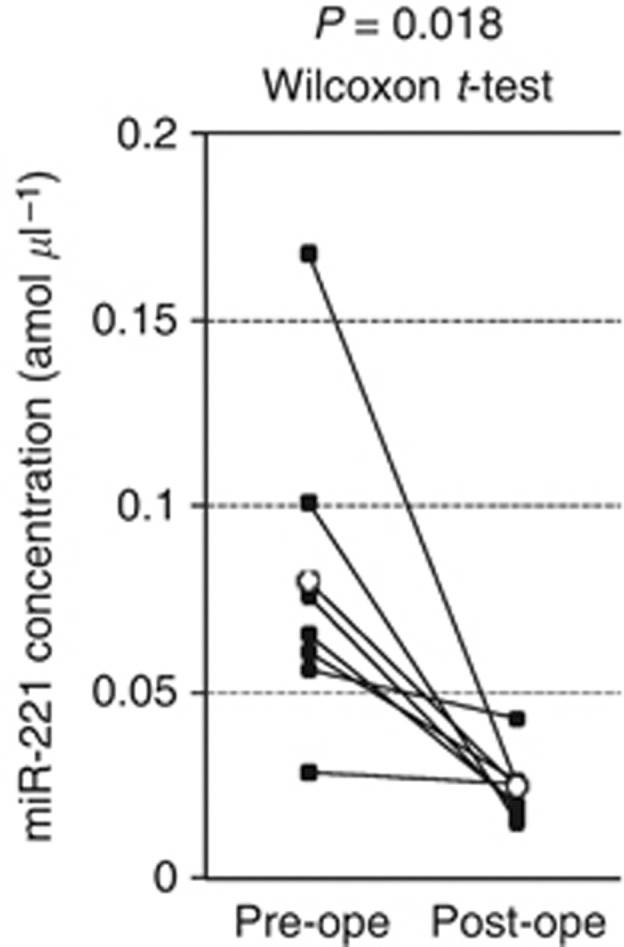
Comparison of plasma miR-221 concentrations between pre- and postoperative samples from PCa patients. Concentrations of miR-221 in plasma were significantly lower in postoperative samples than in preoperative samples (P=0.018).
Correlation between plasma miR-221 concentrations and hematocytes of peripheral blood
A recent report demonstrated that some circulating miRNAs may be derived from peripheral blood cells (Pritchard et al, 2012). Therefore, we determined the correlation between plasma miR-221 concentrations and hematocytes of peripheral blood in 47 PCa patients. As a result, there was no significant correlation between plasma miR-221 concentrations and any types of hematocyte in peripheral blood (Figure 5). Therefore, these data imply that plasma miR-221 may not be derived from any type of hematocyte.
Figure 5.

Correlation between plasma miR-221 concentrations and hematocytes of peripheral blood in PCa patients. There was no significant correlation between plasma miR-221 concentrations and any types of peripheral hematocyte and plasma.
Correlation between plasma miR-221 concentrations and clinicopathological factors in 47 consecutive PCa patients
Finally, we evaluated the correlation between plasma miR-221 concentrations and clinicopathological factors in 47 consecutive PCa patients (Table 1). From the results, patients who presented with high plasma miR-221 concentrations, with a cutoff value of 2.097 × 10−2amol μl−1 calculated by the Younden index (Akobeng, 2007), showed significant correlations with the presence of distant metastasis (P=0.041) and non-resectable status (P=0.021). Although the stage tended to be associated with the plasma level of miR-221, other clinicopathological factors show no significant correlation with the plasma level of miR-221. Moreover, serum markers such as CA19-9, amylase, and bilirubin, which are indicators of tumour presence and pancreatic-biliary tract obstruction, were not correlated with the plasma level of miR-221 (Supplementary Figure S2). Interestingly, of 10 non-resectable lesions, 7 could not be predicted preoperatively by conventional imaging modalities. In contrast, preoperative plasma level of miR-221 could distinguish all non-resectable patients from resectable patients (Table 1). Therefore, the plasma miR-221 level might be a useful clinical biomarker in borderline resectable patients diagnosed by imaging modalities.
Table 1. Correlation between plasma miR-221 concentrations and clinicopathological factors in 47 consecutive PCa patients.
| |
|
miR-221 concentration (amol μl−1)a |
||
|---|---|---|---|---|
|
Variables |
n |
Low |
High |
P-valueb |
| Age (years) | Mean (range) | 67 (42–84) | ||
| ⩽65 | 16 | 4 (29%) | 12 (36%) | 0.7422 |
| ⩾66 |
31 |
10 (71%) |
21 (64%) |
|
|
Sex | ||||
| Male | 27 | 9 (64%) | 18 (55%) | 0.7679 |
| Female |
20 |
5 (36%) |
15 (45%) |
|
|
Histopathology | ||||
| Adenocarcinoma | 42 | 13 (93%) | 29 (88%) | 1 |
| Othersc |
5 |
1 (7%) |
4 (12%) |
|
|
Locationd | ||||
| Ph | 34 | 11 (79%) | 23 (70%) | 0.7255 |
| Pb/Pt |
13 |
3 (21%) |
10 (30%) |
|
|
Depth of invasion | ||||
| T0/1/2 | 7 | 2 (14%) | 5 (15%) | 1 |
| T3/4 |
40 |
12 (86%) |
28 (85%) |
|
|
Lymph node metastasis | ||||
| Negative | 17 | 7 (50%) | 10 (30%) | 0.3404 |
| Positive |
30 |
7 (50%) |
23 (70%) |
|
|
Distant metastasis | ||||
| Negative | 38 | 14 (100%) | 24 (73%) | 0.0417 |
| Positive |
9 |
0 (0%) |
9 (27%) |
|
|
Stagee | ||||
| 0–IIA | 16 | 8 (57%) | 8 (24%) | 0.0657 |
| IIB–IV |
31 |
6 (43%) |
25 (76%) |
|
|
Treatment | ||||
| Resectable | 37 | 14 (100%) | 23 (70%) | 0.0218 |
| Non-resectable | 10 | 0 (0%) | 10 (30%) | |
Abbreviations: PCa=pancreatic cancer; IPMC=intraductal papillary-mucinous carcinoma.
NOTE: Significant values are in boldface type.
Cutoff values for plasma miR-221 concentrations were determined by the Younden index (Akobeng, 2007).
P-values are from χ2 or Fisher's exact probability test and were considered significant at 0.05.
Anaplastic, adenosquamous, endocrine cell carcinoma, IPMC.
Ph=pancreas head; Pb=pancreas body; Pt=pancreas tail.
TNM 7th ed. classification.
Discussion
Numerous genetic and epigenetic alterations are known to be involved in carcinogenesis and tumour progression of various cancers. Of these alterations, non-coding RNAs, so-called miRNAs, have been proven to regulate gene expression by targeting several mRNAs for translational repression or cleavage. MicroRNAs have been demonstrated to contribute to carcinogenesis and progression of various cancers (He et al, 2005; Lu et al, 2005; Calin and Croce, 2006) and, as a result, miRNAs have recently become known as new factors in oncogenesis and provide new therapeutic strategies such as biomarkers and therapeutic targets for cancers.
Several studies have identified tumour-specific alterations in circulating nucleic acids in plasma/serum of cancer patients and have demonstrated the feasibility of circulating nucleic acids as non-invasive biomarkers in patients with various cancers (Sidransky, 1997; Diehl et al, 2008). Particularly, miRNAs were demonstrated to be present in a remarkably stable form in plasma/serum and expression levels of serum/plasma miRNAs are reproducible and consistent among individuals (Chen et al, 2008; Mitchell et al, 2008). Indeed, accumulating reports have suggested overexpression of circulating miRNAs in plasma/serum and clinical application as novel biomarkers of various cancers, such as prostate cancer (Mitchell et al, 2008), leukaemia (Lawrie et al, 2008), oral cancer (Wong et al, 2008), colorectal cancer (Ng et al, 2009), ovarian cancer (Resnick et al, 2009), lung cancer (Hu et al, 2010), and breast cancer (Heneghan et al, 2010) including our reports in gastric cancer (Tsujiura et al, 2010) and oesophageal cancer (Komatsu et al, 2011).
Regarding circulating miRNAs in plasma/serum of PCa, several researchers including us have demonstrated the presence and potential utility of circulating miRNAs such as miR-16, miR-18a, miR-21, miR-155, miR-196a, and miR-210 (Wang et al, 2009; Ho et al, 2010; Morimura et al, 2011; Liu et al, 2012). The main role of these reported miRNAs was cancer detection of PCa by distinguishing cancer patients from healthy individuals. To date, however, there has been no report on the predictive value of circulating miRNAs for malignant outcomes in plasma of patients with PCa. These findings encouraged us to detect more clinically useful miRNAs which facilitate better decision making for PCa treatments.
In this study, we tested an oncogenic miRNA; miR-221 and a tumour suppressive miRNA; miR-375, as candidate targets for this plasma miRNA assay. Of several oncogenic miRNAs, miR-221 has been frequently demonstrated to have an oncogenic function in PCa (Volinia et al, 2006; Szafranska et al, 2007; Zhang et al, 2009; Basu et al, 2011). Also, miR-375 was reported to have a tumour suppressive function in PCa (Basu et al, 2011). Consequently, we demonstrated the feasibility of clinical application using circulating miR-221 for cancer detection, monitoring tumour dynamics, and predicting values of metastatic involvement and surgical resectability in plasma of patients with PCa.
First, we confirmed miR-221 overexpression in primary PCa tissue and PCa cell lines as shown in previous reports (Volinia et al, 2006; Szafranska et al, 2007; Zhang et al, 2009; Basu et al, 2011). Then, we proved that plasma concentrations of miR-221 in PCa patients were significantly higher than healthy volunteers (P<0.001). To investigate more sensitive diagnostic biomarkers in plasma, we further analysed the ratio of circulating miRNA levels, dividing plasma concentrations of miR-221 by that of miR-375, as a combined biomarker shown in previous reports (Tsujiura et al, 2010; Komatsu et al, 2011). As a result, the miR-221/miR-375 ratio was significantly higher in PCa patients than in controls (P<0.0001). The AUCs based on plasma miR-221 concentrations, miR-375 concentrations, and miR-221/miR-375 ratios were 0.743, 0.573, and 0.762, respectively. Although these results were not necessarily outstanding among previously reported circulating miRNAs in PCa patients, plasma miR-221 concentration may have PCa specificity for cancer detection because we could not detect higher miR-221 expression in plasma of patients with oesophageal cancer than healthy volunteers despite its higher expression in oesophageal cancer tissue (Komatsu et al, 2011). Similarly, according to our previous study, we suggest that expression of plasma miRNAs does not always reflect overexpression of all miRNAs in cancer tissue (data not shown). Pancreatic cancer specificity among various cancers is very important for clinical application. These issues are currently under evaluation in an array-based study using large numbers of candidate miRNAs and will be reported in the near future.
Next, we investigated whether plasma miR-221 concentrations could reflect tumour dynamics in PCa by two different analyses. One was the comparison between expression of miR-221 in plasma and primary tumour tissue, which demonstrated that plasma and primary PCa tissue samples showing high levels of plasma miR-221 represented higher expressions in primary PCa tissues than in normal mucosa in all patients analysed (100%) (Supplementary Table S3). Some patients, however, showed different patterns of miRNA levels, low plasma miR-221 with high expression in PCa tissue (data not shown). The reasons for discrepancies in some patients remain to be identified; however, one possible explanation for this finding is the heterogeneity of primary tumours. Second analysis involves comparison of plasma miR-221 concentrations in paired plasma obtained before and after surgery. Consequently, concentrations of miR-221 were significantly reduced postoperatively in patients with high preoperative plasma miR-221 (Figure 4). These findings imply that plasma miR-221 may be released from PCa and reflect tumour dynamics and are available as a new plasma biomarker for monitoring tumour status, such as tumour residue and recurrence of PCa.
We demonstrated the predictive values of plasma miR-221 concentrations for clinicopthological outcomes in patients with PCa; namely, that the preoperative plasma miR-221 concentrations might be a useful clinical biomarker to predict distant metastasis and tumour respectability (Table 1). Also, we found that the plasma level of miR-221 could distinguish PCa patients from patients with pancreatic benign tumours, such as IPMN, serous cystadenoma, and pancreatitis (Supplementary Table S2), and is correlated with the clinical outcomes in patients with PCa. However, our sample size was small. Therefore, we will confirm these clinical findings using plasma samples of large number patients.
Pritchard CC, Tewari M, and their colleagues recently suggested caution in a cancer biomarker study of circulating miRNAs because some circulating miRNAs may be derived from peripheral blood cells (Pritchard et al, 2012). Therefore, we investigated the correlation between plasma miR-221 concentrations and hematocytes of peripheral blood in 47 PCa patients. As a result, there was no significant correlation between plasma miR-221 concentrations and any types of peripheral hematocyte (Figure 4). This result indicated that miR-221 expression in plasma may not be derived from hematocytes, but PCa tissue, and it reflected tumour dynamics in PCa patients. However, the detail mechanisms of secretion, kinetics, and metabolism in plasma miRNAs have not been clearly elucidated and these issues are currently under evaluation.
Taken together, so-called ‘bench-to-bedside' medicine has been aspired for a long time. A non-invasive assay using circulating miRNAs opens up a new and interesting field in the screening and monitoring of cancer patients. Plasma miR-221 concentrations may serve as next-generation biomarkers for cancer detection, monitoring tumour dynamics, and prediction of clinical outcomes such as metastatic involvement and surgical resectability in PCa patients. Plasma miR-221 may contribute to reasonable clinical decision making in PCa treatments. However, many issues must be addressed before these findings can be translated into a clinically useful, non-invasive screening strategy for PCa patients. These issues are currently under detailed evaluation and we will report on them in the near future.
Footnotes
Supplementary Information accompanies this paper on British Journal of Cancer website (http://www.nature.com/bjc)
This work is published under the standard license to publish agreement. After 12 months the work will become freely available and the license terms will switch to a Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License.
Supplementary Material
References
- Akobeng AK. Understanding diagnostic tests 3: receiver operating characteristic curves. Acta Paediatr. 2007;96 (5:644–647. doi: 10.1111/j.1651-2227.2006.00178.x. [DOI] [PubMed] [Google Scholar]
- Arroyo JD, Chevillet JR, Kroh EM, Ruf IK, Pritchard CC, Gibson DF, Mitchell PS, Bennett CF, Pogosova-Agadjanyan EL, Stirewalt DL, Tait JF, Tewari M. Argonaute2 complexes carry a population of circulating microRNAs independent of vesicles in human plasma. Proc Natl Acad Sci USA. 2011;108 (12:5003–5008. doi: 10.1073/pnas.1019055108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Basu A, Alder H, Khiyami A, Leahy P, Croce CM, Haldar S. MicroRNA-375 and microRNA-221: potential noncoding RNAs associated with antiproliferative activity of benzyl isothiocyanate in pancreatic cancer. Genes Cancer. 2011;2 (2:108–119. doi: 10.1177/1947601911409212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bilimoria KY, Bentrem DJ, Ko CY, Stewart AK, Winchester DP, Talamonti MS. National failure to operate on early stage pancreatic cancer. Ann Surg. 2007;246 (2:173–180. doi: 10.1097/SLA.0b013e3180691579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bloomston M, Frankel WL, Petrocca F, Volinia S, Alder H, Hagan JP, Liu CG, Bhatt D, Taccioli C, Croce CM. MicroRNA expression patterns to differentiate pancreatic adenocarcinoma from normal pancreas and chronic pancreatitis. JAMA. 2007;297 (17:1901–1908. doi: 10.1001/jama.297.17.1901. [DOI] [PubMed] [Google Scholar]
- Calin GA, Croce CM. MicroRNA signatures in human cancers. Nat Rev Cancer. 2006;6 (11:857–866. doi: 10.1038/nrc1997. [DOI] [PubMed] [Google Scholar]
- Chen X, Ba Y, Ma L, Cai X, Yin Y, Wang K, Guo J, Zhang Y, Chen J, Guo X, Li Q, Li X, Wang W, Zhang Y, Wang J, Jiang X, Xiang Y, Xu C, Zheng P, Zhang J, Li R, Zhang H, Shang X, Gong T, Ning G, Wang J, Zen K, Zhang J, Zhang CY. Characterization of microRNAs in serum: a novel class of biomarkers for diagnosis of cancer and other diseases. Cell Res. 2008;18 (10:997–1006. doi: 10.1038/cr.2008.282. [DOI] [PubMed] [Google Scholar]
- Cocucci E, Racchetti G, Meldolesi J. Shedding microvesicles: artefacts no more. Trends Cell Biol. 2009;19 (2:43–51. doi: 10.1016/j.tcb.2008.11.003. [DOI] [PubMed] [Google Scholar]
- Diehl F, Schmidt K, Choti MA, Romans K, Goodman S, Li M, Thornton K, Agrawal N, Sokoll L, Szabo SA, Kinzler KW, Vogelstein B, Diaz LA. Circulating mutant DNA to assess tumor dynamics. Nat Med. 2008;14 (9:985–990. doi: 10.1038/nm.1789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Filipowicz W, Bhattacharyya SN, Sonenberg N. Mechanisms of post-transcriptional regulation by microRNAs: are the answers in sight. Nat Rev Genet. 2008;9 (2:102–114. doi: 10.1038/nrg2290. [DOI] [PubMed] [Google Scholar]
- Hasselmann DO, Rappl G, Tilgen W, Reinhold U. Extracellular tyrosinase mRNA within apoptotic bodies is protected from degradation in human serum. Clin Chem. 2001;47 (8:1488–1489. [PubMed] [Google Scholar]
- He L, Thomson JM, Hemann MT, Hernando-Monge E, Mu D, Goodson S, Powers S, Cordon-Cardo C, Lowe SW, Hannon GJ, Hammond SM. A microRNA polycistron as a potential human oncogene. Nature. 2005;435 (7043:828–833. doi: 10.1038/nature03552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heinemann V, Boeck S, Hinke A, Labianca R, Louvet C. Meta-analysis of randomized trials: evaluation of benefit from gemcitabine-based combination chemotherapy applied in advanced pancreatic cancer. BMC Cancer. 2008;8:82. doi: 10.1186/1471-2407-8-82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heneghan HM, Miller N, Lowery AJ, Sweeney KJ, Newell J, Kerin MJ. Circulating microRNAs as novel minimally invasive biomarkers for breast cancer. Ann Surg. 2010;251 (3:499–505. doi: 10.1097/SLA.0b013e3181cc939f. [DOI] [PubMed] [Google Scholar]
- Hirata K, Egawa S, Kimura Y, Nobuoka T, Oshima H, Katsuramaki T, Mizuguchi T, Furuhata T. Current status of surgery for pancreatic cancer. Dig Surg. 2007;24 (2:137–147. doi: 10.1159/000102067. [DOI] [PubMed] [Google Scholar]
- Ho AS, Huang X, Cao H, Christman-Skieller C, Bennewith K, Le QT, Koong AC. Circulating miR-210 as a novel hypoxia marker in pancreatic cancer. Transl Oncol. 2010;3 (2:109–113. doi: 10.1593/tlo.09256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu Z, Chen X, Zhao Y, Tian T, Jin G, Shu Y, Chen Y, Xu L, Zen K, Zhang C, Shen H. Serum microRNA signatures identified in a genome-wide serum microRNA expression profiling predict survival of non-small-cell lung cancer. J Clin Oncol. 2010;28 (10:1721–1726. doi: 10.1200/JCO.2009.24.9342. [DOI] [PubMed] [Google Scholar]
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer J Clin. 2009;59 (4:225–249. doi: 10.3322/caac.20006. [DOI] [PubMed] [Google Scholar]
- Jones S, Zhang X, Parsons DW, Lin JC, Leary RJ, Angenendt P, Mankoo P, Carter H, Kamiyama H, Jimeno A, Hong SM, Fu B, Lin MT, Calhoun ES, Kamiyama M, Walter K, Nikolskaya T, Nikolsky Y, Hartigan J, Smith DR, Hidalgo M, Leach SD, Klein AP, Jaffee EM, Goggins M, Maitra A, Iacobuzio-Donahue C, Eshleman JR, Kern SE, Hruban RH, Karchin R, Papadopoulos N, Parmigiani G, Vogelstein B, Velculescu VE, Kinzler KW. Core signaling pathways in human pancreatic cancers revealed by global genomic analyses. Science. 2008;321 (5897:1801–1806. doi: 10.1126/science.1164368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Komatsu S, Ichikawa D, Takeshita H, Tsujiura M, Morimura R, Nagata H, Kosuga T, Iitaka D, Konishi H, Shiozaki A, Fujiwara H, Okamoto K, Otsuji E. Circulating microRNAs in plasma of patients with oesophageal squamous cell carcinoma. Br J Cancer. 2011;105 (1:104–111. doi: 10.1038/bjc.2011.198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kosaka N, Iguchi H, Yoshioka Y, Takeshita F, Matsuki Y, Ochiya T. Secretory mechanisms and intercellular transfer of microRNAs in living cells. J Biol Chem. 2010;285 (23:17442–17452. doi: 10.1074/jbc.M110.107821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lawrie CH, Gal S, Dunlop HM, Pushkaran B, Liggins AP, Pulford K, Banham AH, Pezzella F, Boultwood J, Wainscoat JS, Hatton CS, Harris AL. Detection of elevated levels of tumour-associated microRNAs in serum of patients with diffuse large B-cell lymphoma. Br J Haematol. 2008;141 (5:672–675. doi: 10.1111/j.1365-2141.2008.07077.x. [DOI] [PubMed] [Google Scholar]
- Lee EJ, Gusev Y, Jiang J, Nuovo GJ, Lerner MR, Frankel WL, Morgan DL, Postier RG, Brackett DJ, Schmittgen TD. Expression profiling identifies microRNA signature in pancreatic cancer. Int J Cancer. 2007;120 (5:1046–1054. doi: 10.1002/ijc.22394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee RC, Feinbaum RL, Ambros V. The C. elegans heterochronic gene lin-4 encodes small RNAs with antisense complementarity to lin-14. Cell. 1993;75 (5:843–854. doi: 10.1016/0092-8674(93)90529-y. [DOI] [PubMed] [Google Scholar]
- Liu J, Gao J, Du Y, Li Z, Ren Y, Gu J, Wang X, Gong Y, Wang W, Kong X. Combination of plasma microRNAs with serum CA19-9 for early detection of pancreatic cancer. Int J Cancer. 2012;131 (3:683–691. doi: 10.1002/ijc.26422. [DOI] [PubMed] [Google Scholar]
- Livak KJ, Schmittgen TD. Analysis of relative gene expression data using real-time quantitative PCR and the 2(−Delta Delta C(T)) method. Methods. 2001;25 (4:402–408. doi: 10.1006/meth.2001.1262. [DOI] [PubMed] [Google Scholar]
- Lu J, Getz G, Miska EA, Alvarez-Saavedra E, Lamb J, Peck D, Sweet-Cordero A, Ebert BL, Mak RH, Ferrando AA, Downing JR, Jacks T, Horvitz HR, Golub TR. MicroRNA expression profiles classify human cancers. Nature. 2005;435 (7043:834–838. doi: 10.1038/nature03702. [DOI] [PubMed] [Google Scholar]
- Mitchell PS, Parkin RK, Kroh EM, Fritz BR, Wyman SK, Pogosova-Agadjanyan EL, Peterson A, Noteboom J, O'Briant KC, Allen A, Lin DW, Urban N, Drescher CW, Knudsen BS, Stirewalt DL, Gentleman R, Vessella RL, Nelson PS, Martin DB, Tewari M. Circulating microRNAs as stable blood-based markers for cancer detection. Proc Natl Acad Sci USA. 2008;105 (30:10513–10518. doi: 10.1073/pnas.0804549105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morimura R, Komatsu S, Ichikawa D, Takeshita H, Tsujiura M, Nagata H, Konishi H, Shiozaki A, Ikoma H, Okamoto K, Ochiai T, Taniguchi H, Otsuji E. Novel diagnostic value of circulating miR-18a in plasma of patients with pancreatic cancer. Br J Cancer. 2011;105 (11:1733–1740. doi: 10.1038/bjc.2011.453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ng EK, Chong WW, Jin H, Lam EK, Shin VY, Yu J, Poon TC, Ng SS, Sung JJ. Differential expression of microRNAs in plasma of patients with colorectal cancer: a potential marker for colorectal cancer screening. Gut. 2009;58 (10:1375–1381. doi: 10.1136/gut.2008.167817. [DOI] [PubMed] [Google Scholar]
- Pfaffl MW. A new mathematical model for relative quantification in real-time RT-PCR. Nucleic Acids Res. 2001;29 (9:e45. doi: 10.1093/nar/29.9.e45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pritchard CC, Kroh E, Wood B, Arroyo JD, Dougherty KJ, Miyaji MM, Tait JF, Tewari M. Blood cell origin of circulating microRNAs: a cautionary note for cancer biomarker studies. Cancer Prev Res (Phila) 2012;5 (3:492–497. doi: 10.1158/1940-6207.CAPR-11-0370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Resnick KE, Alder H, Hagan JP, Richardson DL, Croce CM, Cohn DE. The detection of differentially expressed microRNAs from the serum of ovarian cancer patients using a novel real-time PCR platform. Gynecol Oncol. 2009;112 (1:55–59. doi: 10.1016/j.ygyno.2008.08.036. [DOI] [PubMed] [Google Scholar]
- Satake K, Kanazawa G, Kho I, Chung YS, Umeyama K. A clinical evaluation of carbohydrate antigen 19-9 and carcinoembryonic antigen in patients with pancreatic carcinoma. J Surg Oncol. 1985;29 (1:15–21. doi: 10.1002/jso.2930290106. [DOI] [PubMed] [Google Scholar]
- Shrikhande SV, Kleeff J, Reiser C, Weitz J, Hinz U, Esposito I, Schmidt J, Friess H, Buchler MW. Pancreatic resection for M1 pancreatic ductal adenocarcinoma. Ann Surg Oncol. 2007;14 (1:118–127. doi: 10.1245/s10434-006-9131-8. [DOI] [PubMed] [Google Scholar]
- Sidransky D. Nucleic acid-based methods for the detection of cancer. Science. 1997;278 (5340:1054–1059. doi: 10.1126/science.278.5340.1054. [DOI] [PubMed] [Google Scholar]
- Skog J, Wurdinger T, van Rijn S, Meijer DH, Gainche L, Sena-Esteves M, Curry WT, Carter BS, Krichevsky AM, Breakefield XO. Glioblastoma microvesicles transport RNA and proteins that promote tumour growth and provide diagnostic biomarkers. Nat Cell Biol. 2008;10 (12:1470–1476. doi: 10.1038/ncb1800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sobin LHGM, Wittekind C.2009TNM Classification of Malignant Tumours7th edn.Wiley-Blackwell: New York [Google Scholar]
- Sultana A, Tudur Smith C, Cunningham D, Starling N, Neoptolemos JP, Ghaneh P. Meta-analyses of chemotherapy for locally advanced and metastatic pancreatic cancer: results of secondary end points analyses. Br J Cancer. 2008;99 (1:6–13. doi: 10.1038/sj.bjc.6604436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Szafranska AE, Davison TS, John J, Cannon T, Sipos B, Maghnouj A, Labourier E, Hahn SA. MicroRNA expression alterations are linked to tumorigenesis and non-neoplastic processes in pancreatic ductal adenocarcinoma. Oncogene. 2007;26 (30:4442–4452. doi: 10.1038/sj.onc.1210228. [DOI] [PubMed] [Google Scholar]
- Thayer SP, di Magliano MP, Heiser PW, Nielsen CM, Roberts DJ, Lauwers GY, Qi YP, Gysin S, Fernandez-del Castillo C, Yajnik V, Antoniu B, McMahon M, Warshaw AL, Hebrok M. Hedgehog is an early and late mediator of pancreatic cancer tumorigenesis. Nature. 2003;425 (6960:851–856. doi: 10.1038/nature02009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tsujiura M, Ichikawa D, Komatsu S, Shiozaki A, Takeshita H, Kosuga T, Konishi H, Morimura R, Deguchi K, Fujiwara H, Okamoto K, Otsuji E. Circulating microRNAs in plasma of patients with gastric cancers. Br J Cancer. 2010;102 (7:1174–1179. doi: 10.1038/sj.bjc.6605608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Valadi H, Ekstrom K, Bossios A, Sjostrand M, Lee JJ, Lotvall JO. Exosome-mediated transfer of mRNAs and microRNAs is a novel mechanism of genetic exchange between cells. Nat Cell Biol. 2007;9 (6:654–659. doi: 10.1038/ncb1596. [DOI] [PubMed] [Google Scholar]
- Vickers KC, Palmisano BT, Shoucri BM, Shamburek RD, Remaley AT. MicroRNAs are transported in plasma and delivered to recipient cells by high-density lipoproteins. Nat Cell Biol. 2011;13 (4:423–433. doi: 10.1038/ncb2210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Volinia S, Calin GA, Liu CG, Ambs S, Cimmino A, Petrocca F, Visone R, Iorio M, Roldo C, Ferracin M, Prueitt RL, Yanaihara N, Lanza G, Scarpa A, Vecchione A, Negrini M, Harris CC, Croce CM. A microRNA expression signature of human solid tumors defines cancer gene targets. Proc Natl Acad Sci USA. 2006;103 (7:2257–2261. doi: 10.1073/pnas.0510565103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang J, Chen J, Chang P, LeBlanc A, Li D, Abbruzzesse JL, Frazier ML, Killary AM, Sen S. MicroRNAs in plasma of pancreatic ductal adenocarcinoma patients as novel blood-based biomarkers of disease. Cancer Prev Res (Phila) 2009;2 (9:807–813. doi: 10.1158/1940-6207.CAPR-09-0094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wong TS, Liu XB, Wong BY, Ng RW, Yuen AP, Wei WI. Mature miR-184 as potential oncogenic microRNA of squamous cell carcinoma of tongue. Clin Cancer Res. 2008;14 (9:2588–2592. doi: 10.1158/1078-0432.CCR-07-0666. [DOI] [PubMed] [Google Scholar]
- Zhang Y, Li M, Wang H, Fisher WE, Lin PH, Yao Q, Chen C. Profiling of 95 microRNAs in pancreatic cancer cell lines and surgical specimens by real-time PCR analysis. World J Surg. 2009;33 (4:698–709. doi: 10.1007/s00268-008-9833-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhu H, Fan GC. Extracellular/circulating microRNAs and their potential role in cardiovascular disease. Am J Cardiovasc Dis. 2011;1 (2:138–149. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.