

Abstract
Background
Extensively-drug resistant tuberculosis (XDR-TB) has been reported in 58 countries around the world and has emerged as a major public health challenge. This is the first report to describe pulmonary resection for XDR-TB management in Africa.
Methods
We conducted a retrospective case review of XDR-TB patients who underwent pulmonary resection between January 2007 and December 2009.
Results
Two pneumonectomies and two right upper lobectomies were performed. No operative mortality or major morbidity was noted. All patients achieved sputum conversion and were ultimately regarded as either a “cure” or “probable cure”.
Conclusions
Although the initial cohort of XDR-TB patients from Tugela Ferry demonstrated near complete mortality, our results demonstrate the potential of adjuvant surgical methods in XDR-TB treatment. With appropriate neoadjuvant chemotherapy and timeous surgery, patients with disease localized to lobe or lung XDR-TB may achieve a “cure” with low morbidity and mortality. Consequently, this approach may be the most cost effective treatment for patients suitable for lung resection.
Keywords: XDR-TB, lung resection, South Africa
INTRODUCTION
Extensively-drug resistant tuberculosis (XDR-TB) has been reported in 58 countries around the world and has emerged as a major public health challenge.1 Defined as multidrug resistant (MDR) TB, or strains of Mycobacterium tuberculosis (Mtb) resistant to isoniazid and rifampicin, with additional resistance to any fluoroquinolone, and at least one injectable second line drug2, XDR-TB reports have revealed mortality rates similar to those preceding the discovery of antibiotics3. Strategies to treat XDR-TB have been difficult to optimize due to a restricted number of effective drugs, poor patient compliance, limited resources, and HIV coinfection.4 Although treatment success rates have ranged from 34%5 to 67%6, the relative risk of death due to XDR-TB is 5.5.5 In comparison with MDR-TB, XDR-TB is associated with greater rates of treatment failure, extended hospitalization, and prolonged microbiological conversion.7
Improved treatment outcomes have been reported in XDR-TB patients who underwent pulmonary resection.6,8–13 However, few reports have come from resource-limited settings and no study has described the surgical experience involving patients from the African continent where the TB and HIV epidemics have converged exponentially.14–5 We report our experience in using adjunctive pulmonary resection with individualized chemotherapy regimens for the management of XDR-TB.
PATIENTS AND METHODS
The Department of Cardiothoracic Surgery at King George V Hospital (KGV) is a tertiary care referral center in Durban, South Africa that specializes in the surgical management of drug-resistant TB. A retrospective review of XDR-TB patients referred to KGV between January 2007 and December 2009 was conducted. Criteria for the study included patients with confirmed XDR-TB that underwent pulmonary resection. Data was collected on patient demographics, drug susceptibility profiles, and treatment regimens. Laboratory assessments included complete blood count, blood urea and electrolytes, albumin, and erythrocyte sedimentation rate. Preoperative diagnostic tests involved spirometry, plain chest radiography, high resolution computerized axial tomography (HRCT) scans and, if indicated, ventilation-perfusion isotope scans.
The indications for surgery comprised of failure of a treatment regimen appropriate for XDR-TB, complications of TB sequelae such as hemoptysis or recurrent chest infections, localized disease, and adequate pulmonary reserve to tolerate resection. Open pulmonary resection was performed using established techniques as previously described.16 Excised specimens were submitted for histological examination and microbiological culture. Following surgery, the drug treatment regimen was continued for approximately 18 months and patients were reviewed on a monthly outpatient basis at the TB clinic at King George V Hospital, a referral center that specializes in medical management of drug-resistant tuberculosis.
Treatment outcomes of cure, default, failure, and death, were designated according to the standard MDR-TB definitions.17 Patients who completed treatment and demonstrated consistent culture negativity during the final 12 months of treatment were considered ‘cured’. Patients who were completing chemotherapy at the conclusion of the study that demonstrated consistently negative sputum smear and culture results were classified as ‘probable cure’.12 Treatment interruptions lasting at least two months determined default status. Treatment failure included patients demonstrating culture positivity in at least two of the five cultures in the final 12 months, culture positivity in any of the final three cultures, or based on clinical or radiographic features. Deaths were classified as resulting from any cause while on treatment. Treatment cure and probable cure were considered favorable outcomes, while treatment failure, default, and death were considered unfavorable.
This study was approved by the biomedical ethics review committee at the University of KwaZulu Natal.
RESULTS
Of the 10 XDR-TB patients referred for pulmonary resection, 6 demonstrated bilateral, extensive, cavitatory disease and therefore did not meet the criteria for surgical intervention. Demographic features of the 4 surgical patients are presented in Table 1.
Table 1.
Baseline patient characteristics
| Patient | Sex | Age (years) | Race | Preoperative Sputum Smear | HIV Status |
|---|---|---|---|---|---|
| 1 | M | 37 | Black | Positive | Positive |
| 2 | F | 26 | Indian | Positive | Negative |
| 3 | F | 24 | Black | Positive | Negative |
| 4 | F | 38 | Black | Positive | Negative |
M, male; F, female.
The baseline drug susceptibility profiles of the patients are presented in Table 2. All patients demonstrated resistance to at least 6 drugs. The radiographic features are presented in Table 3, together with the extent of lung resection undertaken. Preoperative chemotherapy regimens, radiographic features, the extent of pulmonary resection undertaken, and treatment outcomes are presented in Table 3. All patients were on an individualized chemotherapy regimen consisting of at least 5 drugs (median: 6 drugs) determined by their respective drug susceptibility results. Drugs to which isolate resistance was noted were used in regimens when no other drugs were available. Postoperative chemotherapy was continued for at least 14.5 months. All patients undergoing surgery demonstrated unilateral disease. There was no operative mortality and all patients achieved sputum culture conversion by the conclusion of the study period.
Table 2.
Baseline drug susceptibility testing
| Patient | Susceptibility
|
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| H | R | E | Z | S | Km | Cip | Ofl | Trd | Eto | |
| 1 | r | r | r | s | r | r | r | s | s | s |
| 2 | r | r | r | s | r | r | r | s | s | s |
| 3 | r | r | r | s | r | r | r | r | s | s |
| 4 | r | r | r | s | r | r | r | s | s | s |
H, isoniazid; R, rifampicin; E, ethambutol; Z, pyrazinamide; S, streptomycin; Km, kanamycin; Cip, ciprofloxacin; Ofl, ofloxacin; Trd, terizidone; Eto, ethionamide; r, resistant; s, sensitive.
Table 3.
Preoperative chemotherapy, operative procedures, and treatment outcomes
| Patient | Preoperative Chemotherapy
|
Chest Radiograph | High Resolution Computerized Axial Tomography Scan | Type of Pulmonary Resection | TB Outcome | |
|---|---|---|---|---|---|---|
| Regimen | Duration | |||||
| 1 | E, Z, Eto, Trd, Ofl | 4.7 | Shrunken RUL with cavitation | Shrunken RUL with cavitation | Right upper lobectomy | Cure |
| 2 | E, Z, Eto, Cs, Cm, PAS | 10.8 | Shrunken, bronchiectatic RLL with scattered bronchiectasis of upper and middle lobes. | Parenchymal disease with “tree- in-bud” pattern* in RUL; Bronchiectatic RML with cavitation and “tree-in-bud” pattern* | Right pneumonectomy | Cure |
| 3 | E, Z, Eto, Mfx, Trd, Cm, PAS | 2.3 | Shrunken, bronchiectatic RUL | Shrunken, bronchiectatic RUL | Right upper lobectomy | Probable cure |
| 4 | E, Z, Eto, Cs, Cm, PAS | 8.1 | Shrunken LUL with cavitation | Shrunken LUL with cavitation; Cavity in left apical segment | Left pneumonectomy | Probable cure |
E, ethambutol; Z, pyrazinamide; Eto, ethionamide; Trd, terizidone; Ofl, ofloxacin; Cs, cycloserine; Cm, capreomycin; PAS, para-aminosalicylic acid; Mfx, moxyfloxacin; RUL, right upper lobe; RLL, right lower lobe, LUL, left lower lobe; RML, right middle lobe;
“tree in bud” pattern – characteristic description of numerous, small, centrilobular nodules of soft-tissue attached to linear branching structures.
Patient 1
A 36-year-old male prisoner was diagnosed with pulmonary tuberculosis in 2002. After a relapse in 2004, drug susceptibility testing confirmed MDR-TB in August 2006, followed by XDR-TB in February 2007. The patient was co-infected with HIV with an initial CD4 count of 75, managed with antiretroviral therapy and had an undetectable viral load at the time of surgery. He was treated with a preoperative chemotherapy regimen consisting of five drugs for 4.7 months preceding surgery. Symptoms included cough and chest pain when he presented for a right upper lobectomy in April 2008. Surgery and his postoperative course were uneventful. He received 15.8 months of postoperative chemotherapy, including 6.3 months of amikacin, until he was classified as “cured”.
Patient 2
A 26-year-old woman was diagnosed with TB in 2005 and relapsed in 2006. She began a six-drug XDR-TB chemotherapy regimen for 10.8 months preceding surgery. In May 2009, a right pneumonectomy was undertaken after she presented with bronchiectasis in addition to TB symptoms of cough, chest pain, and dyspnea. Surgery and her postoperative course were uneventful. Thereafter she received 14.5 months of postoperative chemotherapy, including 13 months of capreomycin, until she was cured.
Patient 3
A 24-year-old nurse failed treatment after original TB diagnosis in October 2008. Drug susceptibility testing confirmed MDR-TB in February 2009, and XDR-TB in April 2009. She was maintained on a seven-drug chemotherapy regimen preceding surgery for 2.3 months before presenting with bronchiectasis, cough, and dyspnea. A right upper lobectomy was undertaken in July 2009. Her postoperative course was complicated by a right pneumothorax following the removal of a pleural drain. The pneumothorax was treated conservatively and the patient progressively improved, with complete resolution noted on chest x-ray in 1.6 months later. She received 15.4 months of postoperative chemotherapy at KGV including 6.6 months of capreomycin and is a probable cure.
Patient 4
A 38-year-old hospital clerk was diagnosed with pulmonary TB in February 2008 and then MDR-TB in July 2008. In August 2008, drug susceptibility testing confirmed XDR-TB. She was maintained on a six-drug chemotherapy regimen for 8.1 months preceding surgery. She presented with hemoptysis, bronchiectasis, dyspnea, chest pain, and cough before undergoing a left pneumonectomy in May 2009. Her postoperative course was uneventful. She has been on a postoperative regimen for 15.3 months including 3.5 months of capreomycin and is still being reviewed at KGV. She is a probable cure.
COMMENT
In this study, we describe excellent clinical and microbiological outcomes using adjuvant pulmonary resection for XDR-TB management. All of the patients successfully achieved sputum conversion and obtained favorable treatment outcomes. This cohort did not experience any complications other than a pneumothorax which was not directly related to the surgery. The use of pulmonary resection for XDR-TB has been previously described, but has been reported to be complicated by bronchopulmonary fistulas, empyema, postpneumonectomy syndrome, and less favorable treatment outcomes.12
The selection of suitable surgical candidates warrants further discussion. Ideally, the patient should be nutritionally sound (as assessed by standard anthropometric tests, BMI and serum albumin) and in satisfactory general condition, essentially able to withstand major thoracic surgery. A range of investigations, including biochemical measurement of acute phase reactants (CRP, ESR) and spirometry, were used to estimate disease activity (an ESR of greater than 70 may indicate active disease) and pulmonary reserve (postoperative predicted FEV1 of >0.8) respectively. Radiographically, the distribution of lung disease was established by use of plain chest radiography and HRCT scan. The surgical approach to drug-resistant tuberculosis is analogous to that of malignancy, i.e. the resection of all macroscopically involved lobes or lung segments and a sensitive drug regimen to treat microscopic residual disease conservatively. Radiographic and surgical pathology confirm that the microbiological disease burden within cavitatory and bronchiectatic lung far exceeds that within nodules (107–109 organisms vs. 102 – 104 organisms) 18, thereby providing an opportunity for the use of pulmonary resection in tuberculosis management. Figure 1 and 2 illustrate the radiographic manifestations of the XDR-TB patients involved in this study. Although these features are not pathognomonic of drug-resistant TB, they demonstrate evidence of sequelar TB (bronchiectasis and cavitation) and active parenchymal TB (‘tree-in-bud’, nodules). The aggressive surgical attitude should thus be tempered by an individualized, pragmatic approach incorporating nutritional status, pulmonary reserve, HRCT features and anticipated pleural space problems in association with insufficient residual lung volume.
Figure 1.
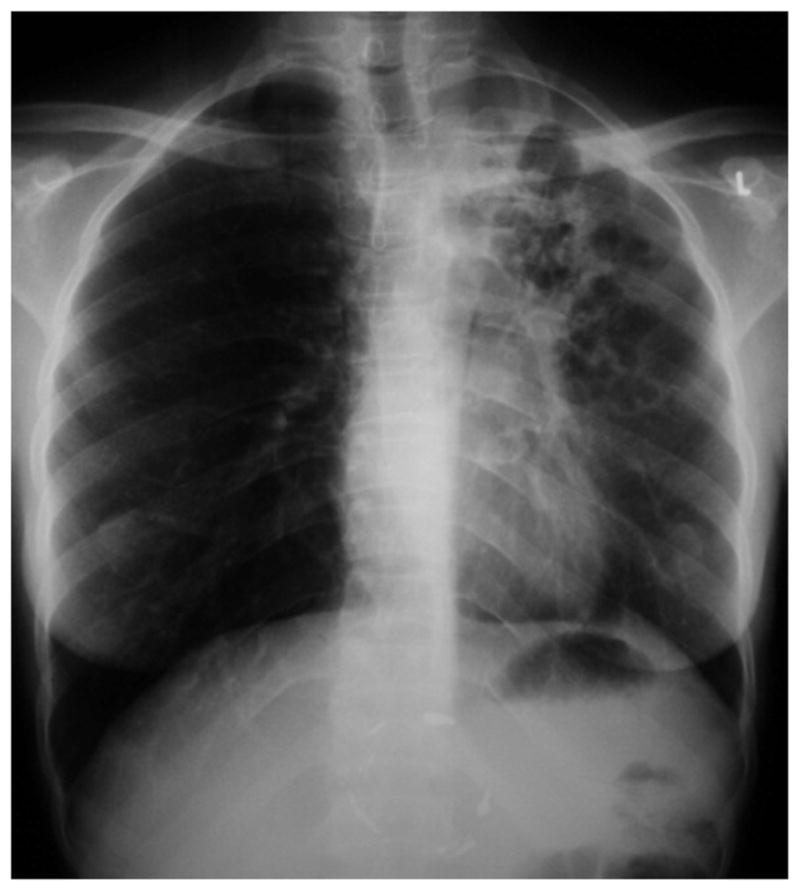
Chest radiograph of patient 4, demonstrating shrinkage and cavitation of the left upper and lower lobe.
Figure 2.
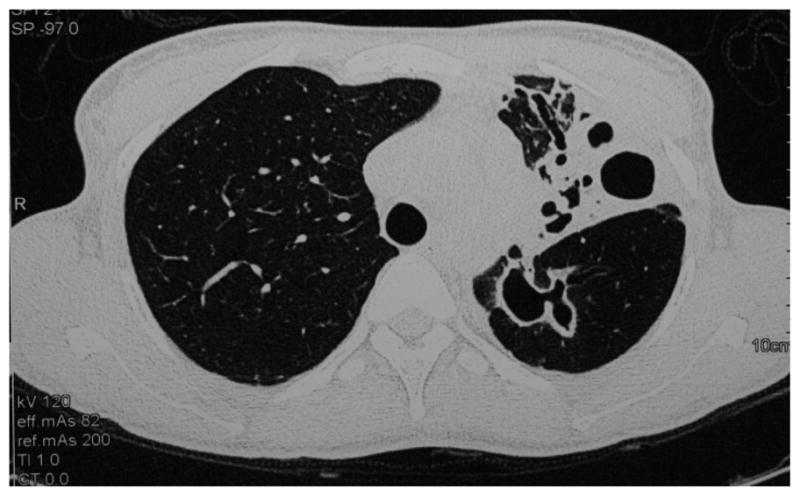
High resolution computed axial tomography scan of Patient 4 confirming bronchiectasis and cavitation of the left upper lobe, with a cavity in the apical segment of the left lower lobe is further illustrated.
The principles for lung resection outlined by Naidoo and Reddi for MDR-TB and inflammatory lung disease were applied to the resection in the 4 patients with XDR-TB in this study.16 In our view, the role of Video Assisted Thorascopic Surgery (VATS) is extremely limited for a variety of reasons in this cohort and thoracotomy is our preference. An adherence to the simple principles of anastomotic technique, i.e. a tension-free suture line, maintenance of adequate tissue blood supply, and membranous flap closure for pneumonectomy, made bronchial stump closure with absorbable interrupted sutures without a muscle pedicle feasible in all our cases.
Although the timing of surgery in XDR-TB management has not been established, Iseman et al recommended at least 3 months of preoperative chemotherapy.19 In our study, the duration on preoperative chemotherapy ranged from 2.3 to 10.8 months. The findings from our study support early surgical intervention in appropriately selected patients followed by postoperative chemotherapy to promote healing of the bronchial stump and remove residual parynchymal disease, which may be present preoperatively or as a result of contralateral contamination or “spill”. A conservative approach to surgical intervention in patients with active tuberculosis is unnecessary and, paradoxically, persistent sputum positivity remains a strong indication for surgery to appropriately selected candidates with drug resistant TB.20
This is the first report of its kind from Africa, which has the highest incidence of TB in the world. According to WHO data, approximately 69000 cases of drug resistant TB emerged in Africa 2008, with rates in some southern African countries at least 5 times higher than those of India and China.1 South Africa is one of the high TB burden countries and nearly 72% of TB patients are coinfected with HIV. Indeed, the original cohort of XDR-TB patients from Tugela Ferry were coinfected with HIV and demonstrated mortality approaching 100%.3 Subsequent reports have confirmed the high early mortality, increased adverse events, and poor treatment outcomes experienced by HIV/XDR-TB patients.21–22
Patient 1 was coinfected with HIV was successfully managed with antiretroviral therapy, achieved sputum conversion, and eventually a TB cure. In South Africa, all patients coinfected with drug-resistant strains of TB and HIV have been able to qualify for antiretroviral therapy, regardless of CD4 count, since April 2010. In addition, there is increasing coordination of TB and HIV services within correctional services. Our findings support the notion that with effective integration of HIV and TB services, disease coinfection does not necessarily imply a short, lethal, inexorable course.
According to WHO data, female TB patients in South Africa are 1.2 times more likely to exhibit drug resistant strains of MTb. In addition, two of the female patients in this study were healthcare workers (HCWs), both of which had a previous history of pulmonary TB before being diagnosed with XDR-TB. Similar to recent reports of drug-resistant tuberculosis in South African HCWs,24–25 XDR-TB in the HCWs of this study did not appear to be associated with HIV infection. Considering their gender and occupation (nurses are more likely to be female), nosocomial acquisition of XDR-TB is likely.26 However, without molecular epidemiologic methods, it was not possible to determine the transmission dynamics of the infections. As HCWs are continuously exposed to patients, in addition to their families and communities, it is imperative that hospitals improve infection control measures through policies that reduce the spread of tuberculosis, especially drug-resistant strains of Mtb.
Future studies should focus on long-term assessment of the South African cohort that has undergone surgery. In addition, prospective studies comparing chemotherapy with combined pulmonary resection and chemotherapy would provide more conclusive evidence of the efficacy of surgery in managing XDR-TB.
Several limitations of our study warrant further discussion. First, as a retrospective chart review, the results are dependent upon previously recorded information, which may be influenced by incomplete data and recorder bias. Second, patients were required to meet stringent criteria before surgery could be performed, resulting in the small number of patients in this single arm study. Furthermore, as XDR-TB was defined in 2006, prior resections may have been undertaken in patients with XDR-TB that were simply labeled MDR TB.
Although the initial cohort of XDR-TB patients from Tugela Ferry demonstrated almost uniform mortality, our results show the potential for effective adjuvant surgical methods in XDR-TB treatment. Despite the aforementioned limitations, we are confident that appropriate pharmacologic and surgical intervention, coupled with early diagnostics and proper infection control measures, can increase the capacity to reduce the burden of the XDR-TB.
In the final analysis, it must be made incandescently clear and emphatically stated that the cohort of patients with active TB (with or without drug resistance), suitable for lung resection is extremely small and probably represents less than a fraction of a percent of all patients with pulmonary tuberculosis, because of a surgical attitude to rigid adherence to stringent criteria and austere indications for surgery.
References
- 1.The WHO/IUATLD Global Project on Anti-Tuberculosis Drug Resistance Surveillance. Multidrug and extensively drug-resistant TB (M/XDR-TB): 2010 global report on surveillance and response. Geneva: World Health Organization; 2010. (Report no. WHO/HTM/TB/2010.3) [Google Scholar]
- 2.Revised definition of extensively drug resistant tuberculosis. MMWR Morb Mortal Wkly Rep. 2006;55:301–5. [Google Scholar]
- 3.Gandhi NR, Moll A, Sturm AW, et al. Extensively drug-resistant tuberculosis as a cause of death in patients co-infected with tuberculosis and HIV in a rural area of South Africa. Lancet. 2006 Nov 4;368(9547):1575–80. doi: 10.1016/S0140-6736(06)69573-1. [DOI] [PubMed] [Google Scholar]
- 4.Madariaga MG, Lalloo UG, Swindells S. Extensively drug-resistant tuberculosis. Am J Med. 2008 Oct;121(10):835–44. doi: 10.1016/j.amjmed.2008.04.015. [DOI] [PubMed] [Google Scholar]
- 5.Migliori GB, Besozzi G, Girardi E, et al. Clinical operational value of the extensively drug-resistant tuberculosis definition. Euro Respir J. 2007;30:623–626. doi: 10.1183/09031936.00077307. [DOI] [PubMed] [Google Scholar]
- 6.Kwon YS, Kim YH, Suh GY, et al. Treatment outcomes for HIV-uninfected patients with multidrug-resistant and extensively drug-resistant tuberculosis. Clin Infect Dis. 2008 Aug 15;47(4):496–502. doi: 10.1086/590005. [DOI] [PubMed] [Google Scholar]
- 7.Sotgiu G, Ferrara A, Matteelli A, et al. Epidemiology and clinical management of XDR-TB: a systematic review by TBNET. Eur Respir J. 2009;33:871–881. doi: 10.1183/09031936.00168008. [DOI] [PubMed] [Google Scholar]
- 8.Dravniece G, Cain KP, Holtz TH, Riekstina V, Leimane V, Zaleskis R. Adjunctive resectional lung surgery for extensively drug-resistant tuberculosis. Eur Respir J. 2009 Jul;34(1):180–3. doi: 10.1183/09031936.00047208. [DOI] [PubMed] [Google Scholar]
- 9.Jeon DS, Kim DH, Kang HS, et al. Survival and predictors of outcomes in non-HIV-infected patients with extensively drug-resistant tuberculosis. Int J Tuberc Lung Dis. 2009 May;13(5):594–600. [PubMed] [Google Scholar]
- 10.Shiraishi Y, Katsuragi N, Kita H, Toishi M, Onda T. Experience with pulmonary resection for extensively drug-resistant tuberculosis. Interact Cardiovasc Thorac Surg. 2008 Dec;7(6):1075–8. doi: 10.1510/icvts.2008.185124. [DOI] [PubMed] [Google Scholar]
- 11.Park SK, Kim JH, Kang H, Cho JS, Smego RA., Jr Pulmonary resection combined with isoniazid- and rifampin-based drug therapy for patients with multidrug-resistant and extensively drug-resistant tuberculosis. Int J Infect Dis. 2009 Mar;13(2):170–5. doi: 10.1016/j.ijid.2008.06.001. [DOI] [PubMed] [Google Scholar]
- 12.Kang M, Kim HK, Hong KK, et al. Surgical treatment for multidrug-resistant and extensive drug-resistant tuberculosis. Ann Thorac Surg. 2010;89:1597–602. doi: 10.1016/j.athoracsur.2010.02.020. [DOI] [PubMed] [Google Scholar]
- 13.Mitnick CD, Shin SS, Seung KJ, et al. Comprehensive treatment of extensively drug-resistant tuberculosis. N Engl J Med. 2008 Aug 7;359(6):563–74. doi: 10.1056/NEJMoa0800106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Naidoo K, Naidoo K, Padayatchi N, Abdool Karim Q. HIV-Associated Tuberculosis. Clin Dev Immunol. 2011;2011:585919. doi: 10.1155/2011/585919. pii. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Abdool Karim SS, Churchyard GJ, Abdool Karim Q, Lawn SD. HIV infection and tuberculosis in South Africa: an urgent need to escalate the public health response. Lancet. 2009 Sep 12;374(9693):921–33. doi: 10.1016/S0140-6736(09)60916-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Naidoo R, Reddi A. Lung resection for multidrug-resistant tuberculosis. Asian Cardiovasc Thorac Ann. 2005 Jun;13(2):172–4. doi: 10.1177/021849230501300216. [DOI] [PubMed] [Google Scholar]
- 17.Laserson KF, Thorpe LE, Leimane V, et al. Speaking the same language: treatment outcome definitions for multidrug-resistant tuberculosis. Int J Tuberc Lung Dis. 2005 Jun;9(6):640–5. [PubMed] [Google Scholar]
- 18.Pomerantz M. General Thoracic Surgery. 6. Lippincott Williams and Wilkins; 2005. Surgery for the Management of Mycobacterium Tuberculosis and Nontuberculous Mycobacterial Infections of the Lung. [Google Scholar]
- 19.Iseman MD, Madsen L, Goble M, Pomerantz M. Surgical intervention in the treatment of pulmonary disease caused by drug-resistant Mycobacterium tuberculosis. Am Rev Respir Dis. 1990 Mar;141(3):623–5. doi: 10.1164/ajrccm/141.3.623. [DOI] [PubMed] [Google Scholar]
- 20.Naidoo R. Active Pulmonary Tuberculosis: Experience with resection in 106 cases. Asian Cardiovasc Thorac Ann. 2007;15:134–138. doi: 10.1177/021849230701500211. [DOI] [PubMed] [Google Scholar]
- 21.Gandhi NR, Shah NS, Andrews JR, et al. HIV coinfection in multidrug- and extensively drug-resistant tuberculosis results in high early mortality. Am J Respir Crit Care Med. 2010 Jan 1;181(1):80–6. doi: 10.1164/rccm.200907-0989OC. [DOI] [PubMed] [Google Scholar]
- 22.O’Donnell MR, Padayatchi N, Master I, Osburn G, Horsburgh CR. Improved early results for patients with extensively drug-resistant tuberculosis and HIV in South Africa. Int J Tuberc Lung Dis. 2009 Jul;13(7):855–61. [PMC free article] [PubMed] [Google Scholar]
- 23.World Health Organization. Global tuberculosis control: A short update to the 2009 report. Geneva: World Health; 2009. (Report no. WHO/HTM/TB/2009.426) [Google Scholar]
- 24.Jarand J, Shean K, O’Donnell M, et al. Extensively drug-resistant tuberculosis (XDR-TB) among health care workers in South Africa. Trop Med Int Health. 2010 Oct;15(10):1179–84. doi: 10.1111/j.1365-3156.2010.02590.x. [DOI] [PubMed] [Google Scholar]
- 25.O’Donnell MR, Jarand J, Loveday M, et al. High incidence of hospital admissions with multidrug-resistant and extensively drug-resistant tuberculosis among South African health care workers. Ann Intern Med. 2010 Oct 19;153(8):516–22. doi: 10.1059/0003-4819-153-8-201010190-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Joshi R, Reingold AL, Menzies D, Pai M. Tuberculosis among health-care workers in low- and middle-income countries: a systematic review. PLoS Med. 2006 Dec;3(12):e494. doi: 10.1371/journal.pmed.0030494. [DOI] [PMC free article] [PubMed] [Google Scholar]