

Abstract
Cyst of the canal of Nuck is a rare cause of inguinal swelling in woman. We report a case of a cyst of the canal of Nuck in which sonography showed a tubular cystic structure with internal septae localized within the inguinal canal. Magnetic resonance examination demonstrated that the mass was hypointense on T1-weighted and hyperintense on T2-weighted series and that there were fine hypointense septae inside the mass on the T2-weighted sequence. Diagnosis of cyst of the canal of Nuck was confirmed by surgery and subsequent histopathologic evaluation.
Keywords: Canal of Nuck, Hydrocele, Cyst, Groin, Sonography, Magnetic resonance imaging
Sommario
La cisti del canale di Nuck è una rara causa di tumefazione inguinale nelle donne. Riportiamo un caso di cisti del canale di Nuck in cui l'ecografia aveva evidenziato una struttura tubulare cistica caratterizzata da setti interni, localizzata nel contesto del canale inguinale. L'esame di RM aveva confermato la natura cistica della lesione, che appariva pertanto ipointensa in T1 e iperintensa con fini sepimentazioni ipointense nelle sequenze T2 pesate. La diagnosi di cisti del canale di Nuck è stata successivamente confermata all'intervento chirurgico e dall'esame isto-patologico.
Introduction
Hydrocele of the canal Nuck is a rare cause of inguinal swelling in women, and it occurs due to a patent processus vaginalis. Radiological findings are described only in a few case reports [1]. Here, we present the ultrasonographic and magnetic resonance imaging findings in this little-known developmental disorder.
Case report
A 38-year-old woman was referred to the department of radiology as her physician suspected inguinal hernia. She complained of a right inguinal mass that had appeared 3 months before. She had no vomiting, and defecation as well as urination were normal. On physical examination an irreducible, fluctuant sausage shaped mass was found. There was no sign of inflammation.
High resolution ultrasonography of the groin (Toshiba Aplio SSA-770 Tokyo, Japan) using a linear transducer (PLT-704 AT 5–11 MHz broadband) revealed a tubular cystic structure of 6.0 × 4.0 × 1.5 cm in diameter with thin internal septae (Fig. 1). The mass did not change its shape when compressed by the transducer. Color Doppler sonography showed no abnormal vascularity, neither peripherally nor in the septae of the cyst. No omentum or intestinal segment was observed in the inguinal canal or within the cyst.
Fig. 1.
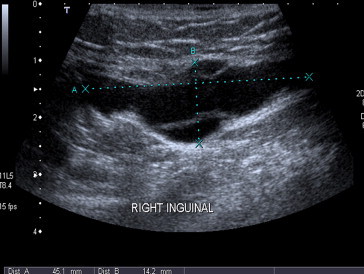
Ultrasonography of the right inguinal canal demonstrates a tubular cystic mass with hypoechoic internal septae.
Magnetic resonance imaging (Signa Excite 2.0, GE Healthcare) demonstrated a well defined lobulated tubular mass which was hypointense on T1-weighted images (Fig. 2) and hyperintense on T2-weighted images (Fig. 3). The mass contained fine hypointense septations on T2-weighted series (Fig. 4). Based on the radiological findings, hydrocele of the canal of Nuck was suspected. Surgery was performed during which the lesion was dissected. Pathologic findings were consistent with a hydrocele of the canal of Nuck.
Fig. 2.
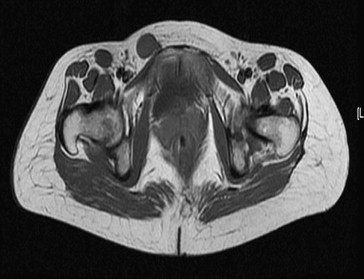
Axial fast spin echo T1-weighted image shows a round hypointense subcutanous lesion within the right inguinal canal.
Fig. 3.
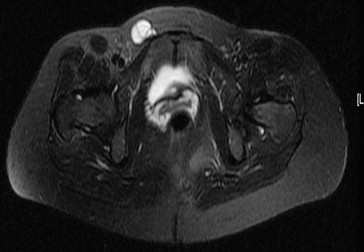
Axial T2-weighted image clearly depicts that the lesion is hyperintense and contains fine hypointense septae.
Fig. 4.
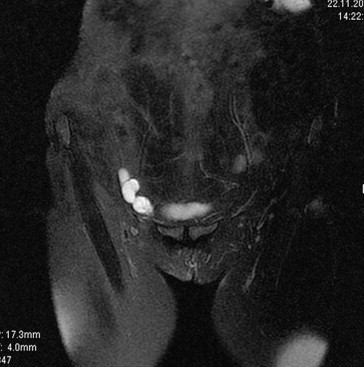
Coronal T2-weighted image clearly depicts that the lesion is hyperintense and contains fine hypointense septae.
Discussion
Hydrocele of the canal of Nuck is an unusual diagnosis with only about 400 reported cases [2,3]. In women, a round ligament is attached to the uterus close to the origin of the fallopian tubes, and the extension of the parietal peritoneum follows the round ligament as it passes to the inguinal canal through the internal ring. This evagination of the parietal peritoneum, named the canal of Nuck, is known as the female counterpart of the processus vaginalis in men. Normally this peritoneal evagination undergoes obliteration soon after birth in both sexes. If it remains completely patent, it forms an avenue for an indirect inguinal hernia. Partial proximal obliteration with a patent distal portion causes a cyst of the canal of Nuck [4]. The cystic enlargement is probably due to the imbalance of the secretion and absorption of the secretory membrane that covers the processus vaginalis. This imbalance may be caused by a change in lymphatic drainage as a result of trauma or infection, although most cases are idiopathic [4].
Clinically a cyst of the canal of Nuck appears as a fluctuant irreducible mass causing mild pain or a painless lump in the inguinal region. Inguinal hernias are always considered in the differential diagnosis. In one third of patients an associated inguinal hernia is present, so diagnosis can be difficult. A cyst of the canal of Nuck is different from an inguinal hernia sac as there is no omental and intestinal contents within the cystic mass. The differential diagnosis list includes also enlarged lymph nodes and soft tissue tumors (e.g. lipomas, leiomyomas and endometriosis of the round ligament). Vascular abnormalities are very rare entities, and ganglion cysts protruding from the hip joint and paraspinal abscesses surfacing onto the groin are on the bottom of the differential diagnosis list [4].
Radiologic findings in the cyst of the canal of Nuck are described only in a few cases in the literature. Sonography is an easily applied and highly accurate imaging modality. A tubular or oval anechoic lesion in the inguinal area or labium majus is observed [1,4–6]. Anderson et al [1] found a tubular anechoic mass extending along the course of the round ligament without any internal structures, thus representing a unilocular hydrocele. Park et al [5] described a cystic structure with a comma shaped tail directed towards the inguinal canal. The reported case was a cystic, thin-walled structure in the inguinal area with hypointense T1 signal and hyperintense T2 signal characteristics; it was the first report of MRI findings in this pathology in English literature. Walter and Martin [4] described a case of a cyst of the canal of Nuck as a “cyst within a cyst”, which is similar to their description of a spermatic cord cyst in a man [4]. Miklos et al. [7] described sonographically guided placement of a hook-wire needle to facilitate surgical exposure of a multicystic hydrocele of the canal of Nuck without giving further details related to the sonographic features of the lesion.
Safak et al [8] described a proximal dilatation at the inguinal canal with an ovoid, septated cystic lesion at the distal end. In contrast with their sonographic findings, MRI showed a simple cyst, which was hypointense on T1-weighted images and hyperintense on T2-weighted images. The authors emphasized the role of Valsalva's maneuver during real time sonography for differentiating a cyst of the canal of Nuck from an inguinal hernia.
In the literature, only a few cases of cysts of the canal of Nuck are described as internal incomplete septae within a cyst demonstrated by ultrasonography and MRI.
In conclusion, the cyst of the canal of Nuck is a rare developmental disorder, but it ought to be on the differential diagnosis list of groin tumors in female patients. Ultrasonography and MR are the imaging modalities of choice for evaluating a cyst of the canal of Nuck.
Conflict of interest statement
The authors have no conflict of interest.
References
- 1.Anderson C.C., Broadie T.A., Mackey J.E., Kopecky K.K. Hydrocele of the canal of Nuck: ultrasound appearance. Am Surg. 1995;61:959–961. [PubMed] [Google Scholar]
- 2.Ihekwaba F.N. Hydrocele in the female. J R Coll Surg Edinb. 1981;26:91–93. [PubMed] [Google Scholar]
- 3.Kucera P.R., Glazer J. Hydrocele of the canal of Nuck: a report of 4 cases. J Reprod Med. 1985;30:439–442. [PubMed] [Google Scholar]
- 4.Walter H.S., Martin M. Female hydrocele (cyst of the canal of Nuck) J Ultrasound Med. 2004;23:429–432. doi: 10.7863/jum.2004.23.3.429. [DOI] [PubMed] [Google Scholar]
- 5.Park S.J., Lee H.K., Hong H.S. Hydrocele of the canal of Nuck in a girl: ultrasound and MR appearance. Br J Radiol. 2004;77:243–244. doi: 10.1259/bjr/51474597. [DOI] [PubMed] [Google Scholar]
- 6.Yigit H., Tuncbilek I., Fitoz S., Yigit N., Kosar U., Karabulut B. Cyst of the canal of Nuck with demonstration of the proximal canal: the role of compression technique in the sonographic diagnosis. J Ultrasound Med. 2006;25:123–125. doi: 10.7863/jum.2006.25.1.123. [DOI] [PubMed] [Google Scholar]
- 7.Miklos J.R., Karam M.M., Silver E., Reid R. Ultrasound and hookwire needle placement for localization of a hydrocele of the canal of Nuck. Obstet Gynecol. 1995;85:884–886. doi: 10.1016/0029-7844(94)00439-k. [DOI] [PubMed] [Google Scholar]
- 8.Safak A.A., Erdogmus B., Yazici B., Gokgoz A.T. Hydrocele of the canal of Nuck: sonographic and MRI appearances. J Clin Ultrasound. 2007;35:531–532. doi: 10.1002/jcu.20329. [DOI] [PubMed] [Google Scholar]