

Medications are the second largest and fastest growing health care cost in Canada.1 In 2010, there were 499.6 million prescriptions dispensed across Canada, representing a total of $23.3 billion. 2 While medications often produce extensive improvements in patient health and well-being, they have also been associated with many preventable adverse events.3,4 In practice, medications are often used at different dosages, with other medications or for patients or conditions that were not included in clinical trials. These factors reflect the complexity of real-world practice and can result in suboptimal medication use that contributes to drug-related morbidity and mortality.5 In 2000, the cost of drug-related morbidity and mortality resulting from drug-related problems exceeded $177.4 billion US in the United States.6 According to a Canadian study completed in 2000, adverse drug reactions occur frequently (7.5 per 100 hospital admissions),7 are preventable (36.9%)7 and prolong hospital stay by an average of 3.6 days.8
Key points.
Academic detailing has been shown to improve patient health outcomes.
Academic detailing is currently available province-wide in British Columbia, Saskatchewan and Nova Scotia.
The role of the pharmacist can include academic detailer, evidence reviewer for topics, developer of key messages and content/supporting tools, developer of the evaluation framework and trainer of other academic detailers.
Points clés.
Il a été démontré que la visite académique améliore les résultats pour la santé des patients.
La visite académique est actuellement offerte dans l'ensemble de la Colombie-Britannique, de la Saskatchewan et de la Nouvelle-Écosse.
Le rôle du pharmacien peut varier de celui de formateur en pharmacothérapie à celui d'examinateur des données probantes ou de développeur de messages clés, de contenu ou d'outils de soutien ou encore de cadres d'évaluation des agents de formation des formateurs en pharmacothérapie.
There have been a number of strategies evaluated to improve medication prescribing and use. An overview of 41 systematic reviews of interventions to change provider behaviour9 found that passive approaches were unlikely to affect changes in provider behaviour, while academic detailing (AD or educational outreach) was considered to be a promising approach, even when delivered as a single intervention.9 AD is a method of continuing education in which a trained health care professional meets with a prescriber (e.g., family physician or nurse practitioner) in their practice setting to provide one-on-one evidence-based information.10 The information given may include feedback about their performance or may be based on overcoming obstacles to change practice. Academic detailing is frequently provided in multifaceted interventions with written materials, continuing education and feedback. One of the main components of academic detailing is that detailers (mostly pharmacists, sometimes nurses or other physicians) provide well-balanced, objective information; this can be accomplished because they are not employed by the pharmaceutical industry and the academic detailing programs do not have any financial links to the pharmaceutical industry.
AD has been employed to effect changes in prescribing practices based on the best available evidence to improve patient health outcomes. Some improvements in the appropriate prescribing by physicians for antibiotics,11–13 benzodiazepines,14–16 NSAIDs,17,18 acid-peptic disease management19 and diuretics for hypertension20 have been observed. AD has also been employed to target behaviours related to the provision of preventive services or the general management of conditions commonly seen in general practice, such as the management of patients with diabetes,21 patients with osteoporosis,22 the provision of smoking cessation advice23 or cancer screening.24,25 A Health Council of Canada report26 corroborated these findings as part of a review of interventions to target suboptimal prescribing. AD was among one of the more highly effective interventions discussed, with some studies showing improvements ranging from 1% to 2%, to improvements as large as 24% to 45%.26 The reason for the large variance is unknown, but factors such as physicians' baseline knowledge of the evidence, number of physicians per AD visit, clinic location, complexity of behaviour change and the make-up of the academic detailing visit have all been considered.27,28 In a Cochrane review, 69 studies showed that academic detailing consistently provided small changes in prescribing that could lead to significant changes, with hundreds of patients being affected.27
Soumerai and Avorn recommend that the following principles of educational outreach be incorporated into academic detailing to improve clinical decision-making:29
Conduct interviews with target audience to investigate baseline knowledge and motivations for current prescribing and practice patterns.
Focus programs on specific groups of prescribers and opinion leaders.
Define clear educational and behavioural objectives.
Establish credibility through a respected organizational identity, referencing authoritative and unbiased sources of information and presenting both sides of controversial issues.
Stimulate active physician participation in educational interactions.
Use concise graphic educational materials.
Highlight and repeat the essential messages.
Provide positive reinforcement of improved prescribing practices during follow-up visits.
The objectives of this article are to provide a brief overview of academic detailing activity in Canada and describe the role of pharmacists as academic detailers.
Academic detailing across Canada
The academic detailing programs in Canada have followed some (if not all) of the principles of academic detailing to foster improved clinical decision-making. In 2003, the Canadian Academic Detailing Collaboration (CADC) was developed by 6 provinces (NS, ON, MB, SK, AB and BC) to represent the academic detailers of Canada.30,31 With the support of the Canadian Agency for Drugs and Technologies in Health (CADTH), representatives from each academic detailing program meet monthly (online) to share experiences in academic detailing. CADC and CADTH have worked together to develop and disseminate key messages of CADTH's evidence reviews to prescribers. The mission of CADC is to 1) promote the development and visibility of academic detailing in Canada, 2) collaborate in developing and disseminating evidence-informed interventions to optimize practice and 3) facilitate research and evaluation of academic detailing initiatives on health outcomes in Canada. Since rigorous evidence of the real-world impacts of academic detailing in Canadian settings is lacking, the CADC provinces formed the Academic Detailing Evaluation Partnership Team (ADEPT) in 2008 to evaluate the impact of detailing on physician prescribing. The research, co-funded by the Canadian Institutes of Health Research and provincial health research agencies, is ongoing until March 31, 2013, with all provinces having completed 1 or more topics and currently proceeding to the data analysis phase. The project is facilitating valuable relationships between provincial research teams, through materials development for common topics, defining measurable indicators and establishing analytic protocols. The research is also a testing ground for the development of common and practical impact evaluation methods for the ongoing assessment of health improvement strategies (e.g., use of the randomized designed delay trial method for comparing physician prescribing).32 Changes in prescribing will be reviewed and the magnitude of impact on health outcomes will be analyzed with a meta-analysis of aggregate level results performed across the provinces. The study also includes a qualitative review of physician and pharmacist/detailer feedback to better understand the factors that contribute to the effective delivery of academic detailing programs.
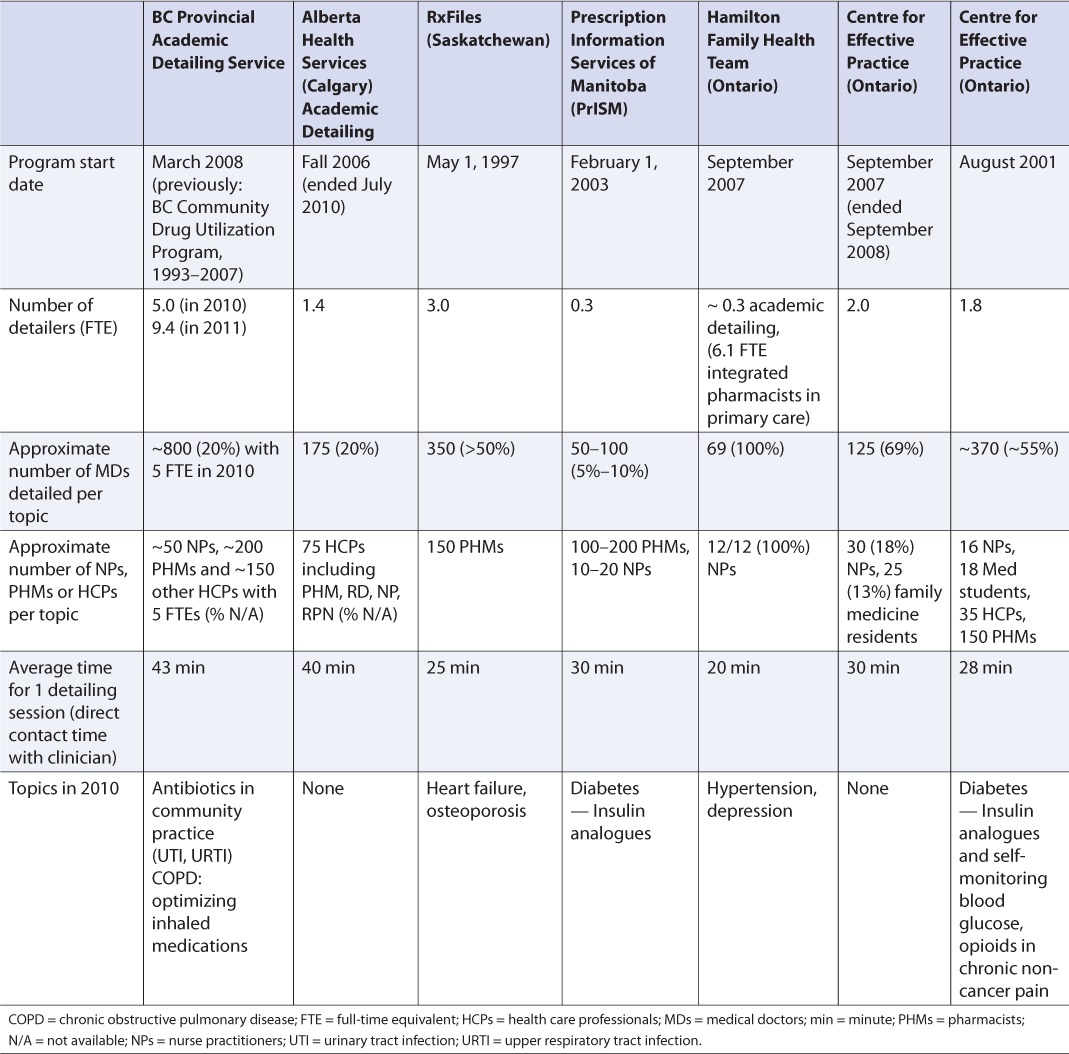
At this time, British Columbia, Saskatchewan and Nova Scotia have province-wide government-funded academic detailing programs (personal communication with the CADC, March 15, 2011). Other existing academic detailing programs include Prescription Information Services of Manitoba (PrISM) and the Hamilton Family Health Team. Prior academic detailing programs included the Alberta Health Services (Calgary) Academic Detailing program and the Centre for Effective Practice (CEP) Best Practice Support Service (academic detailing program) in Ontario. The latter 2 programs have not continued due to insufficient financial support from the provincial governments, however, 2 topics detailed in Alberta are currently being analyzed as part of the ADEPT study and options are similarly being explored for Ontario's involvement. It is hoped that the growing body of evidence on the positive impact of academic detailing will continue to foster provincial and national support of government-funded academic detailing programs. For the current programs, each organizational structure varies with the funding model and needs of the individual jurisdictions. Table 1 provides a summary of each province's academic detailing program (including the existing and past programs identified above). The table was originally developed by the Centre for Effective Practice and subsequently updated and revised by each representative of the CADC program in March 2011. Following is a brief description of each existing academic detailing program (west to east).
TABLE 1.
Overview of Canadian academic detailing programs
British Columbia Provincial Academic Detailing (PAD) Service
British Columbia (BC) began providing academic detailing to family physicians in North and West Vancouver in 1993. In March 2008, the BC PAD service was launched to provide academic detailing to physicians and other health care professionals throughout BC. In 2010, 5.0 full-time equivalent (FTE) detailers provided academic detailing sessions to approximately 800 family physicians (~20% of the eligible practising family physicians in BC) on 2 topics: 1) antibiotics in community practice (focus on adult respiratory tract infections and uncomplicated urinary tract infections) and 2) chronic obstructive pulmonary disease (COPD) — optimizing inhaled medications. With annual funding of $2.25 million per year, the BC PAD service has expanded to 9.4 FTE academic detailers in 2011. In 2011, their goal is to reach approximately 2000 family physicians, which is equivalent to approximately 50% of the eligible practising family physicians in BC. Drug therapy topics are recommended by a broad-based advisory committee with representatives from medical, pharmacy and university groups. A clinical expert is involved in creating the printed educational materials, which are peer reviewed by at least 2 physicians. The academic detailing pharmacists attend an accredited upskilling workshop and do extensive self-study to ensure they are prepared for each topic. A rigorous qualitative and quantitative evaluation is planned for each topic. Technology-enabled academic detailing (TEAD) has also been introduced. TEAD uses real-time web conferencing sessions and an electronic community of practice to connect academic detailers and physicians. It has been shown to extend the efficiency of academic detailers to deliver evidence-informed prescribing information to physicians despite geographic separation.33 Details can be found at www.medmatters.bc.ca/info-hprof/pad.html.
RxFiles (Saskatchewan)
RxFiles began in 1997 as a service to Saskatoon family physicians. In 2000, the program was expanded to provide service to physicians throughout Saskatchewan.34 With a budget of $400,000, RxFiles had 3.0 FTE detailers, who educated approximately 350 family physicians (~50% of the eligible practising family physicians in Saskatchewan) on heart failure and osteoporosis and other emerging topics in 2010. Topics are chosen based on physician surveys, practice gaps, current topics in the news and suggestions from groups who identify practice gaps or current issues (e.g., Health Quality Council, CADTH, CADC). RxFiles also keeps drug comparison charts up to date, publishes online questions and answers on trials and regularly publishes in the Canadian Family Physician journal. More information can be found at www.rxfiles.ca.
Prescription Information Services of Manitoba (PrISM)
PrISM began in 2003 as an academic detailing service to family physicians in Winnipeg and rural Manitoba. This pilot project began with a one-time start-up grant and has used project-specific funding to maintain its function. This limited program has provided written materials to all pharmacists and physicians in the province, participates in group education sessions and uses 0.3 FTE to provide academic detailing services to 50–100 family physicians (~5%–10% of eligible practising family physicians in Manitoba). Topics are selected based on pragmatic assessment of need, available educational and financial resources.
Hamilton Family Health Team (Ontario)
In 2008, the Hamilton Family Health Team (HFHT) took an innovative personalized/patient-specific approach to academic detailing and merged the role of the integrated primary care pharmacists practising within the Family Health Team with the role of the academic detailer to try to minimize some of the challenges of academic detailing. The pharmacy program initiated the idea with no formal budget. One FTE pharmacist spends approximately 1–2 days per week developing the academic detailing program. Topics are selected by physicians' needs and available resources. Since 2008, the 6.1 FTE clinical pharmacists have detailed the HFHT family physicians and nurse practitioners on smoking cessation, hypertension and depression. The key messages are related to the evidence, guidelines and recommendations plus the suggestion to the clinician to refer patients to see the pharmacist for smoking cessation education, blood pressure follow-up or medication review. At this time, academic detailing plays a small role in the pharmacists' time — the majority of their time is spent caring for patients (medication reviews, diabetes education, smoking cessation education, etc.). It is estimated that for each 1.0 FTE pharmacist, 0.05 FTE time is spent on academic detailing. In 2010, 6.1 FTE clinical pharmacists trained in academic detailing educated 69/69 (100%) HFHT family physicians and 12/12 (100%) HFHT nurse practitioners on hypertension using updated guidelines and recent evidence. With their unique role as health care members of the team, the electronic medical record was used to identify specific patients with hypertension. The team of pharmacist and prescriber applied the evidence to each individual patient to optimize prescribing practices. Some clinicians referred their patients with hypertension to the pharmacist for a full medication review and identification of any drug-related issues. A descriptive retrospective cohort pilot project study on academic detailing in the primary care setting on smoking cessation was completed in 2011. Eight pharmacists (5.8 FTE) detailed 48 physicians and 9 nurse practitioners on the evidence for smoking cessation. Within 6 months, 200 new patients were referred to the pharmacists for smoking cessation counselling (data not yet published). To learn more about the Hamilton Family Health Team, go to www.hamiltonfht.ca.
Dalhousie Academic Detailing Service (ADS) in Nova Scotia
In 2001, Nova Scotia became the first province in Canada to undertake a province-wide academic detailing program.35 Each academic detailing topic is developed with the assistance of a drug evaluation pharmacist, at least 1 specialist physician and an advisory board consisting of 4 urban and rural family physicians. With an annual budget of $300,000, 1.8 FTE academic detailers educated approximately 370 family physicians (~55% of family physicians in the province) on opioids in chronic non-cancer pain and on insulin analogues and self-monitoring of blood glucose in 2010. In addition to providing clinicians with evidence-based information, the service encourages a culture of critical thinking by informing them of uncertainties and controversies in the interpretation of evidence. More information can be found at http://cme.medicine.dal.ca/ADS.htm.
Role of the pharmacist
The role of the pharmacist ranges from academic detailer, evidence reviewer for topics and topic selection, developer of key messages and content/supporting tools, developer of the evaluation framework to trainer of other academic detailers. Training can be completed through workshops involving practising prescribers and hands-on experience with another trained or experienced academic detailer. Pharmacists with or without doctoral-level training have been effective in academic detailing.36,37 Training of an academic detailer involves the history of academic detailing, evidence supporting the impact of academic detailing, principles of social marketing, the development of key messages, advanced literature evaluation, an understanding of family physicians' practice environment, role play in which learners practise an academic detailing visit and concepts of persuasive communication with application to academic detailing. The CADC has been instrumental in coordinating this training for academic detailers across the country.
The content of material or topic selection varies based on the program model and needs of the local physician population of the individual jurisdiction. The materials are evidence-based with appropriate referencing and are peer reviewed by specialists, family physicians and pharmacists. The academic detailing sessions are generally one-on-one in the clinician's office setting. The average time spent with each clinician is approximately 20 minutes to review 3–5 key messages per topic (can range from 5 to 60 minutes per session). Ideally, after each academic detailing session, the health care professional should have the opportunity to evaluate the visit and receive continuing education credits.
Academic detailing does have some inherent challenges. Many family physicians (up to 50% in Nova Scotia) have not taken the opportunity to use academic detailing because they prefer to access continuing medication education (CME) in other ways, do not want to schedule office time for CME, do not want to have CME provided by a nonphysician and feel AD is time consuming, meant to cut expenses, politically coloured and/or patronizing. 38,39 Some ways in which members of CADC have tried to minimize some of these challenges include technology-enabled academic detailing, booking academic detailing sessions during nonpatient scheduled appointments (e.g., lunch, early morning, non-clinic days), offering CME credits and providing topics that are up to date and/or relevant to the physicians' practice. The pharmacists at the HFHT also see the clinicians at least once every 2 weeks and can detail key messages between patient visits at scheduled times, during team meetings and in response to physicians' patient-specific drug-related issues.
In summary, pharmacists are often considered to play a role in academic detailing because of their training in pharmacology and drug information. The considerable investment in medications for our society justifies a parallel investment in academic detailing as an effective way of enhancing clinical decision-making and optimizing medication use.40,41 Evidence indicates that academic detailing may provide benefits that exceed the costs for some but not all interventions.42–48 Academic detailing has become a cornerstone of interventions to optimize prescribing in 3 provinces that have fully funded programs providing services to all practising family physicians. Although smaller academic detailing programs exist, more support is required to maintain the key principles of academic detailing throughout Canada. This can potentially optimize prescribing practices, prevent adverse effects and help to ensure value for our investment in medication while improving health outcomes for all Canadians.
References
- 1.Canadian Institute for Health Information. Drug expenditure in Canada, 1985 to 2010. Ottawa (ON): Canadian Institute for Health Information; 2011. Available: http://secure.cihi.ca/cihiweb/products/drug_expenditure_2010_en.pdf (accessed July 14, 2011) [Google Scholar]
- 2.Campeau L. Top RxDrugs of 2010. Pharmacy Practice. 2011;February/March:32–6. [Google Scholar]
- 3.Hanlon JT, Artz MB, Pieper CF, et al. Inappropriate medication use among frail elderly inpatients. Ann Pharmacother. 2004;38:9–14. doi: 10.1345/aph.1D313. [DOI] [PubMed] [Google Scholar]
- 4.Piecoro LT, Browning SR, Prince TS, et al. A database analysis of potentially inappropriate drug use in an elderly medicaid population. Pharmacother. 2000;20:221–8. doi: 10.1592/phco.20.3.221.34779. [DOI] [PubMed] [Google Scholar]
- 5.Lau E, Dolovich L. Drug-related problems in elderly general practice patients receiving pharmaceutical care. Int J Pharm Pract. 2005;13:165–77. [Google Scholar]
- 6.Ernst FR, Grizzle AJ. Drug-related morbidity and mortality: updating the cost-of-illness model. J Am Pharm Assoc. 2001;41:192–9. doi: 10.1016/s1086-5802(16)31229-3. [DOI] [PubMed] [Google Scholar]
- 7.Baker GR, Norton PG, Flintoft V, et al. The Canadian adverse events study: the incidence of adverse events among hospital patients in Canada. CMAJ. 2004;170:1678–86. doi: 10.1503/cmaj.1040498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Canadian Institute for Health Information. Hospital morbidity database 2000/01 Tabular reports. Ottawa (ON): Canadian Institute for Health Information; 2002. Available: http://secure.cihi.ca/cihiweb/products/HospitalMorbidityTabularReports2000-2001.pdf (accessed July 14, 2011) [Google Scholar]
- 9.Grimshaw JM, Shirran L, Thomas R, et al. Changing provider behavior: an overview of systematic reviews of interventions. Med Care. 2001;39:I12–I45. [PubMed] [Google Scholar]
- 10.Knowledge Translation Program. 2006. Glossary of terms in knowledge translation and continuing education. KTClearinghouse. Available: http://ktclearinghouse.ca/knowledgebase/knowledgetoaction/action/interventions/strategies/academicdetailing (accessed April 5, 2012) [Google Scholar]
- 11.Coenen S, Van Royen P, Michiels B, Denekens J. Optimizing antibiotic prescribing for acute cough in general practice: a cluster-randomized controlled trial. J Antimicrob Chemother. 2004;54:661–72. doi: 10.1093/jac/dkh374. [DOI] [PubMed] [Google Scholar]
- 12.Seager JM, Howell-Jones RS, Dunstan FD, et al. A randomised controlled trial of clinical outreach education to rationalise antibiotic prescribing for acute dental pain in the primary care setting. Br Dent J. 2006;201:217–22. doi: 10.1038/sj.bdj.4813879. [DOI] [PubMed] [Google Scholar]
- 13.Solomon DH, Van Houten L, Glynn RJ, et al. Academic detailing to improve use of broad-spectrum antibiotics at an academic medical center. Arch Intern Med. 2001;161:1897–902. doi: 10.1001/archinte.161.15.1897. [DOI] [PubMed] [Google Scholar]
- 14.Berings D, Blondeel L, Habraken H. The effect of industry-independent drug information on the prescribing of benzodiazepines in general practice. Eur J Clin Pharmacol. 1994;46:501–5. doi: 10.1007/BF00196105. [DOI] [PubMed] [Google Scholar]
- 15.de Burgh S, Mant A, Mattick RP, et al. A controlled trial of educational visiting to improve benzodiazepine prescribing in general practice. Aust J Public Health. 1995;19:142–8. doi: 10.1111/j.1753-6405.1995.tb00364.x. [DOI] [PubMed] [Google Scholar]
- 16.Schmidt I, Claesson CB, Westerholm B, et al. The impact of regular multidisciplinary team interventions on psychotropic prescribing in Swedish nursing homes. J Am Geriatr Soc. 1998;46:77–82. doi: 10.1111/j.1532-5415.1998.tb01017.x. [DOI] [PubMed] [Google Scholar]
- 17.Newton-Syms FA, Dawson PH, Cooke J, et al. The influence of an academic representative on prescribing by general practitioners. Br J Clin Pharmacol. 1992;33:69–73. doi: 10.1111/j.1365-2125.1992.tb04002.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Pit SW, Byles JE, Henry DA, et al. A quality use of medicines program for general practitioners and older people: a cluster-randomised controlled trial. Med J Aust. 2007;187:23–30. doi: 10.5694/j.1326-5377.2007.tb01110.x. [DOI] [PubMed] [Google Scholar]
- 19.Offman JJ, Segal R, Russell WL, et al. A randomized trial of an acid-peptic disease management program in a managed care environment. Am J Manag Care. 2003;9:425–33. [PubMed] [Google Scholar]
- 20.Stafford RS, Bartholomew LK, Cushman WC, et al. Impact of the ALLHAT/JNC7 dissemination project on thiazide-type diuretic use. Arch Intern Med. 2010;170:851–8. doi: 10.1001/archinternmed.2010.130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Feder G, Griffiths C, Highton C, et al. Do clinical guidelines introduced with practice based education improve care of asthmatic and diabetic patients? A randomised controlled trial in general practices in east London. BMJ. 1995;311:1473–8. doi: 10.1136/bmj.311.7018.1473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Solomon DH, Polinski JM, Stedman M, et al. Improving care of patients at-risk for osteoporosis: a randomized controlled trial. J Gen Intern Med. 2007:362–7. doi: 10.1007/s11606-006-0099-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Young JM, D'Este C, Ward JE. Improving family physicians' use of evidence-based smoking cessation strategies: a cluster randomization trial. Prev Med. 2002;35:572–83. doi: 10.1006/pmed.2002.1111. [DOI] [PubMed] [Google Scholar]
- 24.Kim CS, Kristopaitis RJ, Stone E, et al. Physician education and report cards: do they make the grade? Results from a randomized controlled trial. Am J Med. 1999;107:556–60. doi: 10.1016/s0002-9343(99)00293-4. [DOI] [PubMed] [Google Scholar]
- 25.Walsh JM, Salazar R, Terdiman JP, et al. Promoting use of colorectal cancer screening tests. Can we change physician behaviour? J Gen Intern Med. 2005;20:1097–101. doi: 10.1111/j.1525-1497.2005.0245.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Sketris I, Langille E, Lummis H. Optimal prescribing and medication use in Canada: challenges and opportunities. Toronto (ON): Health Council of Canada; 2007. Available: http://publications.gc.ca/collections/collection_2007/hcc-ccs/H174-6-2007E.pdf (accessed July 14, 2011) [Google Scholar]
- 27.O'Brien MA, Rogers S, Jamtvedt G, et al. Educational outreach visits: effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2007;(4):CD000409. doi: 10.1002/14651858.CD000409.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Freemantle N, Nazareth I, Eccles M, et al. A randomized controlled trial of the effect of educational outreach by community pharmacists on prescribing in UK general practice. Br J Gen Pract. 2002;52:290–5. [PMC free article] [PubMed] [Google Scholar]
- 29.Soumerai SB, Avorn J. Principles of educational outreach (“academic detailing”) to improve clinical decision making. JAMA. 1990;263:549–56. [PubMed] [Google Scholar]
- 30.Bacovsky R, Maclure M, Nyguyen A, et al. Canadian Academic Detailing Collaboration: evaluating processes and outcomes of academic detailing. Can Pharm J. 2006;139:54–7. [Google Scholar]
- 31.Maclure M, Allen M, Bacovsky R, et al. Show me the evidence: best practices for using educational visits to promote evidence-based prescribing. Victoria (BC): Drug Policy Futures; 2006. Available: http://web.his.uvic.ca/dpf/index.php?Research_Themes:Academic_detailing (accessed July 14, 2011) [Google Scholar]
- 32.Maclure M, Nguyen A, et al. Measuring prescribing improvements in pragmatic trials of educational tools for general practitioners. Basic Clin Pharmacol Toxicol. 2006;98:243–52. doi: 10.1111/j.1742-7843.2006.pto_301.x. [DOI] [PubMed] [Google Scholar]
- 33.Cordeiro J, Lauscher H, Olatunbosun T, et al. Physician-pharmacist electronic linkage for evidence informed prescribing: from project to provincial implementation in British Columbia. Poster Presentation. eHealth Conference 2011, Toronto, Ontario. [Google Scholar]
- 34. RxFiles. About us. Available: www.rxfiles.ca/rxfiles/modules/aboutus/AboutUs.aspx (accessed July 14, 2011) [Google Scholar]
- 35.Academic detailing service. Faculty of Medicine: continuing medical education. Dalhousie University. Available: http://cme.medicine.dal.ca/ADS.htm (accessed July 14, 2011) [Google Scholar]
- 36.Avorn J, Soumerai SB. Improving drug-therapy decisions through educational outreach: a randomized controlled trial of academically based “detailing.”. N Engl J Med. 1983;308:1457–63. doi: 10.1056/NEJM198306163082406. [DOI] [PubMed] [Google Scholar]
- 37.Avorn J, Soumerai SB, Everitt DE, et al. A randomized trial of a program to reduce the use of psychoactive drugs in nursing homes. N Engl J Med. 1992;327:168–73. doi: 10.1056/NEJM199207163270306. [DOI] [PubMed] [Google Scholar]
- 38.Allen M, Ferrier S, O'Conner N, et al. Family physicians' perception of academic detailing: a quantitative and qualitative study. BMC Medical Education. 2007;7:36. doi: 10.1186/1472-6920-7-36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Janssens I, De Meyere M, Habraken H, et al. Barriers to academic detailers: a qualitative study in general practice. Eur J Gen Pract. 2005;11:59–63. doi: 10.3109/13814780509178239. [DOI] [PubMed] [Google Scholar]
- 40.Soumerai SB, Avorn J. Principles of educational outreach (“academic detailing”) to improve clinical decision making. JAMA. 1990;263:549–56. [PubMed] [Google Scholar]
- 41.Davis DA, Thomson MA, Oxman AD, et al. Changing physician performance. A systematic review of the effect of continuing medical education strategies. JAMA. 1995;274:700–5. doi: 10.1001/jama.274.9.700. [DOI] [PubMed] [Google Scholar]
- 42.Freemantle N, Eastaugh J. Using effectiveness studies for prescribing research, part I. J Clin Pharm Ther. 2002;27:383–9. doi: 10.1046/j.1365-2710.2002.00423.x. [DOI] [PubMed] [Google Scholar]
- 43.Mason J, Freemantle N, Nazareth I, et al. When is it cost-effective to change the behavior of health professionals? JAMA. 2001;286:2988–92. doi: 10.1001/jama.286.23.2988. [DOI] [PubMed] [Google Scholar]
- 44.Fretheim A, Aaserud M, Oxman AD. Rational prescribing in primary care (RaPP): economic evaluation of an intervention to improve professional practice. PLoS Med. 2006;3(6):e216. doi: 10.1371/journal.pmed.0030216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Soumerai SB, Avorn J. Economic and policy analysis of university-based drug “detailing.”. Medical Care. 1986;24:313–31. doi: 10.1097/00005650-198604000-00003. [DOI] [PubMed] [Google Scholar]
- 46.Lemelin J, Hogg W, Baskerville N. Evidence to action: a tailored multifaceted approach to changing family physician practice patterns and improving preventive care. CMAJ. 2001;164(6):757–63. [PMC free article] [PubMed] [Google Scholar]
- 47.Steele MA, Bess DT, Franse VL, Graber SE. Cost effectiveness of two interventions for reducing outpatient prescribing costs. DICP. 1989;23:497–500. doi: 10.1177/106002808902300612. [DOI] [PubMed] [Google Scholar]
- 48.Coopers & Lybrand Consultants. Drug and therapeutics information service: update of the economic evaluation of the NSAID project. In: May FW, Rowett D, editors. DATIS progress report to the Department of Health and Family Services October to March 1995–96. Canberra: Australian Commonwealth Department of Health and Family Services; 1996. [Google Scholar]