

Abstract
Takotsubo cardiomyopathy is characterized by the development of transient focal wall-motion abnormalities that involve the apical and midventricular segments, in the absence of obstructive coronary artery disease. A variant, inverted takotsubo cardiomyopathy, was described in 2010. We report 3 cases in which each patient's transthoracic echocardiogram revealed the characteristic basal and midventricular segmental akinesis of this variant. This pattern is not associated with coronary artery distribution, and it therefore can be differentiated from coronary artery disease with the use of echocardiography, by evaluating the distribution and temporal changes of akinetic areas.
Key words: Cardiomyopathies/diagnosis/physiopathology; echocardiography; takotsubo cardiomyopathy/diagnosis; ventricular dysfunction, left/diagnosis
WEBSITE FEATURE
Takotsubo cardiomyopathy is a syndrome characterized by transient apical and midventricular akinesis that is typically precipitated by acute stress. A variant, with akinesis of the mid and basal left ventricular (LV) segments and sparing of the apex, has been called inverted (or atypical) takotsubo cardiomyopathy. We describe 3 cases of this variant in which the transthoracic echocardiograms (TTEs) and temporal evolution of the condition were diagnostic. Each patient was emergently admitted to Barnes-Jewish Hospital in St. Louis and examined there; the TTEs were reviewed by a visiting cardiologist (AM).
Case Reports
Patient 1
A 51-year-old woman with a history of depression and no cardiac disease was admitted after having been found unresponsive and surrounded by benzodiazepines and opiate bottles. An electrocardiogram (ECG) showed minimal, nonspecific T-wave changes. The patient's cardiac troponin I level was 6.5 ng/mL. A TTE revealed a moderately reduced overall LV ejection fraction (LVEF) of 0.35, with basal and midventricular segmental hypokinesis and preserved apical segmental function (Fig. 1). Cardiac catheterization revealed no angiographically significant coronary artery disease. Two weeks later, a TTE showed overall normalization of the LVEF and segmental wall-motion abnormalities.
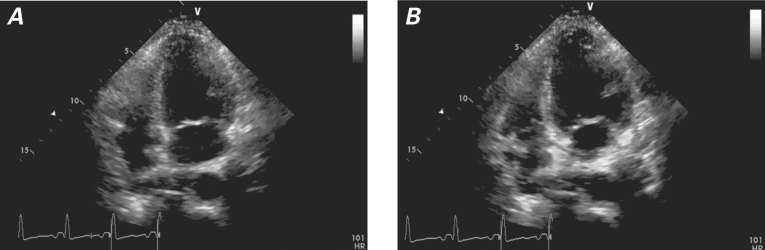
Fig. 1 Patient 1. Transthoracic echocardiogram (4-chamber view) during A) systole and B) diastole shows basal and midventricular segmental hypokinesis but preserved apical segmental function during systole.
Real-time motion image is available at www.texasheart.org/journal.
Patient 2
A 45-year-old woman with a history of hypothyroidism, depression, and chronic abdominal pain was admitted after anaphylactic shock that was caused by gadolinium contrast medium used during abdominal magnetic resonance. She was treated with antihistamines, epinephrine, and intravenous fluids. She subsequently reported chest pain. An ECG showed no significant abnormalities. Blood tests revealed an elevated cardiac troponin I level (2.43 ng/mL). A TTE showed moderate LV dysfunction (LVEF, 0.35) with midventricular and basal akinesis and apical hyperkinesis (Fig. 2). This was interpreted as inverted takotsubo cardiomyopathy, in consideration of the epinephrine that the patient had been given for anaphylaxis-induced hypotension. Four days after the initial episode, TTE showed complete normalization of the akinetic segments.
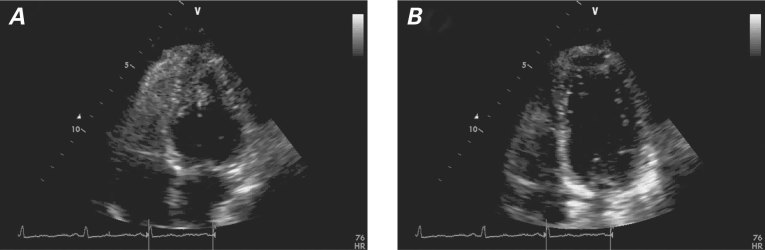
Fig. 2 Patient 2. Transthoracic echocardiogram in A) systole and B) diastole shows severe midventricular and basal akinesis and apical hyperkinesis.
Real-time motion image is available at www.texasheart.org/journal.
Patient 3
A 21-year-old man was admitted after a motor vehicle accident. He had sustained a severe, traumatic brain injury and was unresponsive (Glasgow coma scale, 2). A computed tomographic scan of the patient's head revealed a large left subdural hematoma with a large amount of subarachnoid hemorrhage. An ECG showed minimal ST-segment elevation in leads V1 through V3. The patient's cardiac troponin I level was elevated (15 ng/mL). A TTE showed severe LV dysfunction (LVEF, 0.25). The LV was akinetic except for the apex, which appeared to be hyperkinetic (Fig. 3). An analysis of global longitudinal peak systolic strain showed normal apical strain with reduced strain in the mid and basal segments (Fig. 4). Several hours after the patient's admission, the hemorrhage was evacuated; however, his neurologic status continued to deteriorate, and he died.
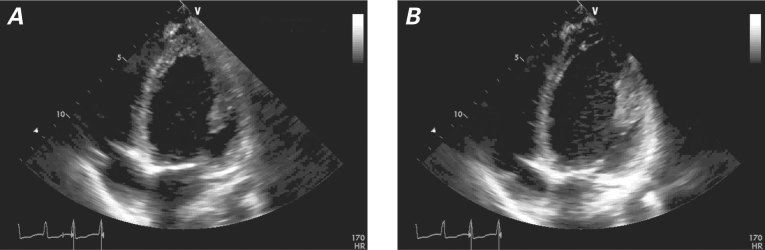
Fig. 3 Patient 3. Transthoracic echocardiogram in A) systole and B) diastole shows severe left ventricular dysfunction and wall-motion abnormalities typical of inverted takotsubo cardiomyopathy.
Real-time motion image is available at www.texasheart.org/journal.
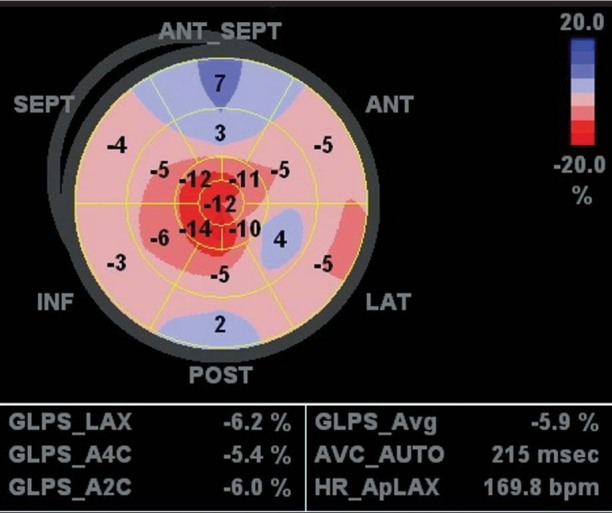
Fig. 4 Patient 3. Global longitudinal peak systolic strain (GLPS) shows normal apical strain and reduced strain in the mid and basal segments.
A2C = apical 2-chamber; A4C = apical 4-chamber; ANT = anterior; ANT_SEPT = anteroseptal; AVC_AUTO = automatic video-level control; Avg = average; HR_ApLAX = heart rate–apical long-axis; INF = inferior; LAT = lateral; POST = posterior; SEPT = septal
Discussion
Takotsubo (stress-induced) cardiomyopathy is characterized by the development of transient wall-motion abnormalities in the absence of obstructive coronary artery disease. This cardiomyopathy was initially described in the Japanese population in 1991 as a syndrome of reversible LV dysfunction with wall-motion abnormalities that involve the apical and midventricular segments.1 Its presentation can resemble that of myocardial infarction, with similar ECG changes and biomarker elevation. The syndrome is typically triggered by severe emotional or physical stress. Its exact cause is unknown. Several pathophysiologic mechanisms have been proposed, such as multivessel coronary vasospasm, abnormalities in coronary microvascular function, and catecholamine-mediated cardiotoxicity.2
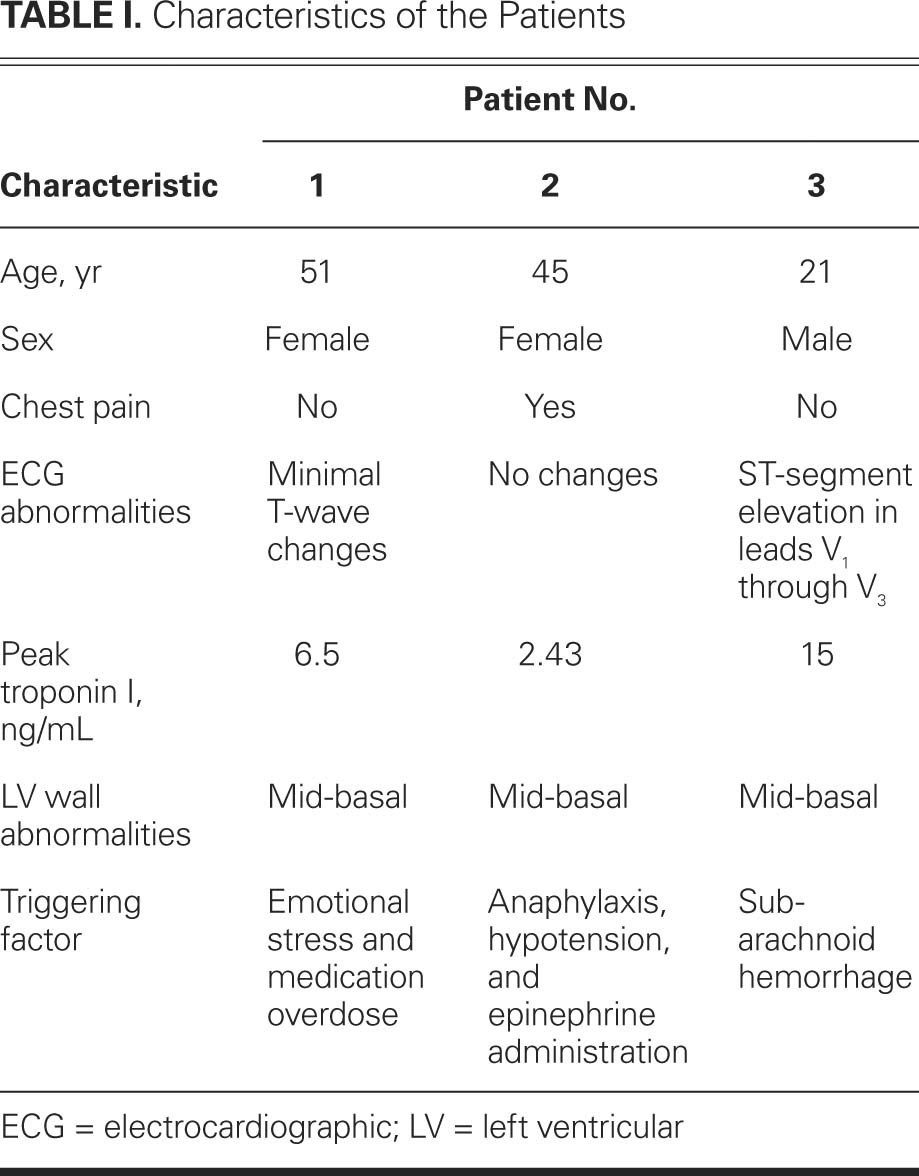
In our patients, the triggers differed from one another (Table I); however, each could expectedly be associated with elevated catecholamine levels. In patient 1, the syndrome was related to mental stress and multiple substance abuse. Patient 2 had hypotension caused by anaphylaxis and exogenous epinephrine. Patient 3 had posttraumatic subarachnoid hemorrhage.
TABLE I. Characteristics of the Patients
Takotsubo syndrome varies in nature, depending upon the affected segments of the LV. The midventricular and inverted variants are 2 examples. The inverted variant presents as hypokinesis or akinesis of the basal and midventricular segments with preserved contractility of the apical segments.3
The prevalence of takotsubo cardiomyopathy in the general population is estimated to be 1.2% to 2.2%.3–6 Inverted takotsubo cardiomyopathy could be more common than was initially believed. In one series,4 it constituted 40% of the cases of stress-induced cardiomyopathy. Accordingly, awareness of this variant aids in its prompt recognition in the appropriate clinical setting.
The different patterns of LV dysfunction in stress-induced cardiomyopathy might occur in the same patient during temporally distinct episodes.6 Alternatively, different patterns might evolve during one episode. If the event starts as apico-midventricular dysfunction and evolves into isolated midventricular dysfunction in the same patient, it could explain the different patterns of myocardial dysfunction that have been observed.6
The proposed Mayo Clinic criteria7 require all 4 of the following for the diagnosis of takotsubo cardiomyopathy: 1) transient hypokinesis, akinesis, or dyskinesis of the LV mid segments, with or without apical involvement, with the regional wall-motion abnormalities extending beyond a single epicardial vascular distribution; 2) the absence of obstructive coronary disease or angiographic evidence of acute plaque rupture; 3) new ECG abnormalities or elevation in cardiac troponin levels; and 4) the absence of pheochromocytoma or myocarditis. These criteria cannot always be fulfilled because of coexistent clinical conditions that contraindicate cardiac catheterization. When catheterization cannot be performed, the echocardiographic distribution of wall-motion abnormalities and their temporal resolution can help to differentiate takotsubo cardiomyopathy from an acute coronary syndrome.
In our series, patient 1 had the typical echocardiographic pattern and temporal evolution, and normal coronary arteries. Patient 2 had the typical echocardiographic pattern and temporal evolution, but it was not possible to perform cardiac catheterization because of her acute presentation and rapid clinical improvement. In patient 3, it was not possible to determine the recovery of LVEF because of the fatal outcome; nevertheless, the echocardiographic results were typical of a variant of stress-induced cardiomyopathy. Furthermore, the observed wall-motion abnormalities did not match an epicardial coronary distribution; the patient was a young man without cardiovascular risk factors; and the syndrome occurred in a clinical setting known to precipitate stress-induced cardiomyopathies (intracranial hemorrhage).8
We found transthoracic echocardiography to be integral to the diagnosis of inverted takotsubo cardiomyopathy in these 3 patients.
Supplementary Material
Footnotes
Address for reprints: Arantza Manzanal, MD, Department of Cardiology, Basurto Hospital, Av. Montevideo 18, 48013 Bilbao, Spain
E-mail: Arantza.manzanal@gmail.com
References
- 1.Dote K, Sato H, Tateishi H, Uchida T, Ishihara M. Myocardial stunning due to simultaneous multivessel coronary spasms: a review of 5 cases [in Japanese]. J Cardiol 1991;21(2):203–14. [PubMed]
- 2.Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or takotsubo cardiomyopathy: a systematic review. Eur Heart J 2006;27(13):1523–9. [DOI] [PubMed]
- 3.Ramaraj R, Movahed MR. Reverse or inverted takotsubo cardiomyopathy (reverse left ventricular apical ballooning syndrome) presents at a younger age compared with the mid or apical variant and is always associated with triggering stress. Congest Heart Fail 2010;16(6):284–6. [DOI] [PubMed]
- 4.Kurowski V, Kaiser A, von Hof K, Killermann DP, Mayer B, Hartmann F, et al. Apical and midventricular transient left ventricular dysfunction syndrome (tako-tsubo cardiomyopathy): frequency, mechanisms, and prognosis. Chest 2007;132 (3):809–16. [DOI] [PubMed]
- 5.Bybee KA, Prasad A, Barsness GW, Lerman A, Jaffe AS, Murphy JG, et al. Clinical characteristics and thrombolysis in myocardial infarction frame counts in women with transient left ventricular apical ballooning syndrome. Am J Cardiol 2004;94(3):343–6. [DOI] [PubMed]
- 6.Chattopadhyay S, John J. Tako-tsubo and reverse tako-tsubo cardiomyopathy: temporal evolution of the same disease? Eur Heart J 2009;30(23):2837. [DOI] [PubMed]
- 7.Bybee KA, Kara T, Prasad A, Lerman A, Barsness GW, Wright RS, Rihal CS. Systematic review: transient left ventricular apical ballooning: a syndrome that mimics ST-segment elevation myocardial infarction. Ann Intern Med 2004; 141(11): 858–65. [DOI] [PubMed]
- 8.Ennezat PV, Pesenti-Rossi D, Aubert JM, Rachenne V, Bauchart JJ, Auffray JL, et al. Transient left ventricular basal dysfunction without coronary stenosis in acute cerebral disorders: a novel heart syndrome (inverted takotsubo). Echocardiography 2005;22(7):599–602. [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.