

Abstract
The polyomavirus (PyV), JC virus (JCV), is a small nonenveloped DNA virus that asymptomatically infects about 80% of healthy adults and establishes latency in the kidney tissue. In case of immunodeficient hosts, JCV can lytically infect the oligodendrocytes, causing a fatal demyelinating disease, known as progressive multifocal leukoencephalopathy (PML). Although the reactivation of another human PyV, BK virus (BKV), is relatively common and its association with the polyomavirus associated nephropathy (PyVAN) following renal transplantation is proven, JCV replication and its impact on graft function and survival are less well studied. Here we describe the biology of JCV and its pathological features and we review the literature regarding the JCV infection analyzed in the setting of transplantations.
1. An Introduction to the Human Polyomavirus JC (JCV)
JC virus (JCV) is a member of the Polyomaviridae family, including naked DNA viruses with icosahedral capsids and small, circular, and double-stranded DNA genomes. The natural hosts for polyomaviruses (PyVs) include humans, other primates, rodents, rabbits, and birds [1].
It was first isolated by Padgett et al. in 1971 from the brain of a patient with the initial JC, affected by Hodgkin's lymphoma who died of progressive multifocal leukoencephalopathy (PML), a demyelinating disease of the central nervous system (CNS) [2].
The 40–45 nm capsid is composed of three structural viral proteins, VP1, VP2, and VP3. The icosahedron consists of 72 pentamers, with no apparent hexamers, each composed by five VP1 molecules and one molecule of VP2 or VP3. The virion is formed of 88% protein and 12% DNA, represented by a single copy of supercoiled, circular, and double-stranded molecule of approximately 5.2 kb, associated with cellular histone proteins H2A, H2B, H3, and H4 and packaged into chromatin resembling cellular genomes (minichromosomes) [1, 3, 4].
The viral genome has a bipartite organization and contains two regions of about the same size, known as early and late transcription units, transcribed in opposite directions starting from a common hypervariable noncoding control region (NCCR), containing the origin of DNA replication (ori), the TATA box, cellular transcription factors binding sites, and bidirectional promoters and enhancers for the transcription of early and late genes. Starting from the NCCR, early transcription proceeds in a counterclockwise direction, while late transcription proceeds clockwise on the opposite strand of the DNA [5].
The early region spans 2.4 kb and encodes the alternatively spliced transforming proteins, large tumor antigen (T-Ag) and small tumor antigen (t-Ag), which are involved in the viral replication and in promoting transformation of cells in culture and oncogenesis in vivo [5].
The late coding region spans 2.3 kb and encodes the capsid proteins VP1, VP2, and VP3 by alternative splicing of a common mRNA derived from the same primary late transcript and a small regulatory protein, known as agnoprotein, whose function in the virus life cycle is not completely clear [5] (Figure 1).
Figure 1.
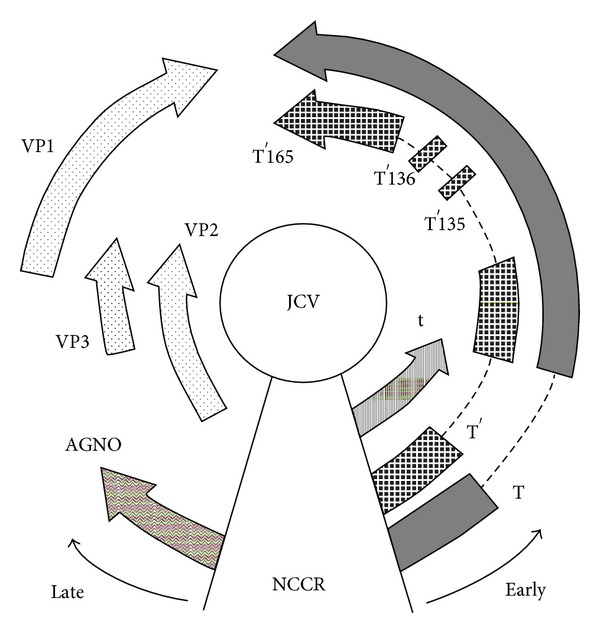
Schematic representation of the JCV genome organization. The circular, double-stranded DNA genome is ~5.2 kb in size and is divided into the early coding region and the late coding region, transcribed in opposite directions from a common noncoding control region (NCCR). Early genes include large T antigen (T-Ag), small t antigen (t-Ag), T′135, T′136, and T′165. Late genes include VP1, VP2, VP3, and agnoprotein.
JCV does not infect any species other than humans and its ability to infect human cells may be restricted at the level of viral early gene transcription and DNA replication, with the T-Ag interacting specifically with the human DNA polymerase [6].
JCV has a tropism for replication in human glial cells, kidney epithelial cells, and, with a less efficiency, in B lymphocytes, and the restricted CNS tropism is confirmed by both experimental animals and in vitro analysis [6, 7].
The transmission of JCV is not fully understood. JCV-specific antibodies are detected in approximately 70% of adults [8] and the primary infection occurs in early childhood, usually in an asymptomatic way and results in a primary viremia. Afterwards, the virus produces a persistent latent infection in the kidney and is shed into the urine. In the context of an immunosuppressive condition, such as AIDS and transplantation, JCV disseminates to the CNS and lytically infects oligodendrocytes, causing the demyelinating disease, known as PML [9–11].
2. Progressive Multifocal Leukoencephalopathy
PML is a rare demyelinating disease characterized by the lytic infection of glial cells and is often fatal. The disease occurs almost exclusively in patients with severe immunodeficiency; consequently, the incidence of PML has increased dramatically, following the spread of HIV/AIDS. Nowadays, HIV infection is still the most frequent setting for PML, ~80% of the cases, followed by hematologic malignancies (~8%), solid cancers (~3%), organ transplantation, and autoimmune diseases treated with immunomodulators [12].
The classic form of PML is progressive and multifocal and involves the white matter. The main symptoms of the disease are motor deficits, altered consciousness, gait ataxia, and visual disturbances [13, 14]. Atypical presentations of PML are increasingly recognized and include cerebellar syndrome, reflecting productive infection of granule cell neurons [15], meningitis [16], meningoencephalitis [17, 18], progressive myoclonic ataxia [19] and muscle wasting associated to extrapyramidal signs [20]. The median survival of PML patients without HIV infection is of few months, while in HIV positive patients subjected to highly active antiretroviral therapy (HAART) is longer but characterized by severe impairment of CNS. Indeed, successful treatments for PML are not currently available.
3. JCV and Transplantation: Epidemiology
Reports of JCV infection in renal transplant recipients have been published immediately after the first isolation of the virus [32, 33]. Since those times, subsequent works have investigated both the silent and the symptomatic infection and/or reactivation of JCV in the setting of kidney transplantation, finding contradictory results. In 1980, Hogan et al. reported active infection after transplantation with JCV in about half of the 61 patients investigated [33]. Gardner and colleagues performed a wide prospective, serological study for the evidence of JCV infection in forty-eight renal transplant recipients, finding that 54% of the patients were seropositive already before the operation and that in 23% of the seronegative patients JCV infection occurred within the first three months after transplantation [34]. Molecular analyses were also conducted, by means of specific hybridization in situ, PCR, and quantitative PCR assays by different international groups: JCV has been identified in kidney biopsy tissue and/or urine within a range of 3.4% and 46% of kidney transplanted patients (Table 1) [21–31, 35]. The most recent surveys, that had the possibility to measure the amount of replicating JCV in the clinical specimens, reported also a very wide range of viral loads, from 2.0 × 103 copies/mL to 1 × 107 copies/mL [21, 22, 25, 31, 35, 36]. The association between the JCV viruria and transplantation has not been proved yet. In fact, Yin and colleagues showed that JCV load was markedly increased in transplant patients compared to the healthy group, confirming the association between immune function and viral levels [25]. On the contrary, Husseiny and colleagues observed a very low level JCV shedding in the urine of both normal subjects (15%) and renal transplant recipients, with no differences among the viral loads [21]. Regarding JCV viremia in the renal transplant recipients, it seems to be very rare, transient, and low. In a cohort of 103 patients, it has been observed only in 14.2% of subjects with a mean viral load of 2 × 103 copies/mL; in another study conducted on 20 patients, 25% showed JCV viremia from the lower limit of detection (of 25 copies/mL) up to 103 copies/mL [21]. A long-term prospective follow-up study was conducted in France and JCV was detected in only 31 blood samples out of the 1487 collected [29].
Table 1.
Studies on JCV and kidney transplantation.
| Subjects (n) | Sample | JCV (+)/subjects (%) | Pathological correlation | Reference |
|---|---|---|---|---|
| KTx: 103 | Urine Blood |
23/103 (22.3%) 0/103 (0%) |
None | [21] |
| Controls: 23 | Urine Blood |
8/23 (34.7%) 0/23 (0%) |
||
|
| ||||
| KTx: 103 | Urine Blood |
28/103 (27.2%) 15/103 (14.2%) |
None | [22] |
| Controls: 0 | / | / | ||
|
| ||||
| KTx: 76 | Urine Blood |
12/76 (15.8%) 0/76 (0%) |
None | [23] |
| Controls: 0 | / | / | ||
|
| ||||
| KTx: 68 | Urine | 14/68 (21%) | None | [24] |
| Controls: 0 | / | / | ||
|
| ||||
| KTx: 60 | Urine | 24/60 (40%) | None | [25] |
| Controls: 60 | Urine | 11/60 (18.3%) | ||
|
| ||||
| KTx: 186 | Urine | 33/186 (17.8%) | None | [26] |
| Controls: 0 | / | / | ||
|
| ||||
| KTx: 25 | Urine Serum |
6/25 (24%) 6/25 (24%) |
None | [21] |
| Controls: 20 | Urine | 3/20 (15%) | ||
|
| ||||
| KTx: 52 | Urine | 8/52 (15.4%) | None | [27] |
| Controls: 30 | Urine | 0/30 (0%) | ||
|
| ||||
| KTx: 59 | Urine | 2/59 (3.4%) | ||
| CRD: 102 | Urine | 4/102 (3.9%) | None | [28] |
| Controls: 134 | Urine | 27/134 (20.1%) | ||
|
| ||||
| KTx: 103 | Blood | 7/103 (6.8%) | None | [29] |
| Controls: 0 | / | / | ||
|
| ||||
| KTx: 30 | Urine | 7/30 (23.3%) | None | [30] |
| Controls: 30 | Urine | 7/30 (23.3%) | ||
|
| ||||
| KTx: 30 | Urine | 5/30 (16.7%) | None | [31] |
| Controls: 0 | / | / | ||
KTx: kidney transplant recipients; CRD: chronic renal diseases.
Only few studies analyzed also the molecular features of the isolated virus, mainly observing that the JCV strains infecting the kidney transplantation recipients did not differ significantly from those infecting the immunocompetent subjects [36, 37]. On the contrary, Yin and colleagues observed a dramatic increase in the proportion of transplant patients carrying two or more genotype strains of JCV compared with control subjects assuming an association between uncommon JCV genotypes and immunosuppression [25].
Regarding the nonkidney solid organ transplants (SOT), the incidence and clinical manifestation of JCV infection have been even more poorly investigated. In 2005, two independent groups published very different results about JCV infection in liver transplant patients, reporting 1.7% and 22.7% of patients excreting the virus, respectively [35, 38]. More recently, Kusne and colleagues [39] examined the frequency of JCV urinary shedding in a longitudinal study on 41 kidney and 33 liver transplant recipients. The proportion of patients shedding JCV was found higher in the liver than in the kidney transplant group (71% versus 38%), with a viral load of 1.2 × 107 copies/mL and 3.9 × 106 copies/mL, respectively. In addition, none of the patients with JCV viruria had also JCV viremia.
A prospective prevalence study on 100 liver transplant children reported a JCV viruria in 19%, without clinical signs of viral infection. The viruria was not influenced by the extent of immunosuppressive therapy but it was found higher in pediatric liver transplant recipients [40] than reported in adult patients [41, 42].
Studies on the association between JCV infection and lung, pancreas and heart transplantations are very rare. Antonsson and colleagues [43] analyzed the seroprevalence and antibody stability of JCV in 441 organ transplant recipients, including 386 kidney, 9 heart, 1 kidney and heart, and 35 kidney and pancreas, over a time period of up to 18 months. The JCV seroprevalence was shown as 76% at baseline, higher than reported previously (reviewed in [43]), and it increased continuously over time reaching 80.4%.
A previous study [38] on 263 heart, kidney, liver, and pancreas transplant patients reported JCV DNA in the blood for 2.7% of kidney, 0.04% of kidney pancreas, 1.1% of heart, and 0.8% of liver grafts, which was transient in 69% of the episodes. The majority of JCV DNAemic episodes were subclinical (61.5%). Only 5 patients (38.5%) had clinical symptoms at the time of JCV DNAemia, one out of which had biopsy-proven acute heart rejection, whereas the other four patients had fatigue, lethargy, dyspnea, or tremors. No patients developed manifestations of PML. Since the overall JCV DNAemia rate was 5%, the authors remarked that JCV infection is a rare complication after SOT. JCV DNAemia was more common in kidney and/or pancreas transplant patients, possibly reflecting the reactivation of donor-derived JCV, which also persists in the kidneys [38]. These data were confirmed by Kamar and colleagues [44] that showed a higher JCV viremia in kidney (5.5%) than in liver and heart rituximab-treated transplant patients.
Regarding JCV infections in lung transplant recipients, Thomas and colleagues [45] tested urine samples for the presence of JCV with conventional PCR, demonstrating a positivity rate of 24% in at least one urine specimens. Mean viral load analyzed with q-PCR was 5 × 105 copies/mL. However, there was no significant association between the immunosuppressive regiment and PyV infection. In fact, the prevalence of chronic graft dysfunction was 42% and 53% in patients who shed JCV or not, respectively. In addition, there was no significant correlation between urinary viral load and the patient's age and sex, the patient's immunosuppressive regimen, and the number of month after transplantation.
Although the different experimental approaches and the various results reported by the analyzed studies, they all agree that a strict attention should be paid to monitoring JCV infection, especially during the first 24 months following transplantation. In fact, even if JCV replication was mostly silent, it was not ruled out the hypothesis that it could be associated with certain clinical syndromes, as reported in Section 4.
4. JCV and Kidney Transplantation: The Virus-Associated Diseases
Infection by JCV has been observed in renal allograft recipients as both nephropathy and/or PML. PML occurs rarely in renal transplant patients and it is typically caused by JCV with high levels of viral genome found in the CSF (reviewed in [46]). However, recent reports suggest that another PyV, BKV, can also cause a PML-like disease [47, 48].
Renal transplant recipients have the highest risk of developing polyomavirus associated nephropathy (PyVAN) in comparison to other organ recipients because of the presence of ongoing graft injury due to drug toxicity, rejection episodes, cold ischemia, and donor/recipients HLA mismatch [49–52]. PyVAN with graft dysfunction and premature graft loss has been markedly increased since the 1990s [53, 54]; therefore, a pathogenic potential of JCV should be taken into account. In contrast to the closely related BKV, to date, only few cases of nephropathy have been attributed to JCV [55–59]. Low level of JCV replication and shedding are common in immunocompetent individuals [60, 61] but surprisingly the incidence of asymptomatic viruria is not increased in renal allograft recipients [62, 63]. This suggests that immunosuppressive state is not as strictly related to the development of PyVAN as it is for BKV [64, 65]. In addition, the immunosuppressive regimen does not play any important role and, once JCV PyVAN has been established, the reduction of immunosuppression has a controversial impact on the clinical course [66]. However, a profound immunosuppressive state is required for a pathological and potentially threatening JCV replication. In fact, patients with PML have significant JCV viruria and PML and JCV PyVAN have been reported to occur concurrently [58, 67–70]. This raises the question whether anti-CD20 biological therapy with rituximab in kidney transplant recipients is potentially cumbersome, because of a rapid depletion of pre-B and mature B cells that lasts for at least six months upon its administration. Our recent report in a small cohort of pediatric kidney transplant recipients showed that rituximab treatment had no effect on susceptibility to JCV replication [36]. These findings confirm some reports on adult population treated with either rituximab [71] or different immunomodulator drugs such as natalizumab [72, 73], where the risk of JCV new infection or reactivation was found inconsistent.
In a recent paper by Drachenberg and colleagues based on urine cytology and prospective protocol kidney biopsy in a cohort of hundred kidney transplant recipients, the incidence of JCV PyVAN was reported as low as 0.9% despite the fact that a significant proportion of the patients displayed JCV viruria or decoy cell shedding [22]. Interestingly, the majority of JCV PyVAN was diagnosed in patients with a normal renal function suggesting an apparently less aggressive or more protracted clinical course when compared with BKV PyVAN. This was recently confirmed by Cheng et al. in a larger cohort of kidney transplant recipients where the clinical outcome of JCV viruric patients was reported to be favorable up to five years following transplant [74]. Compared to non-JCV viruric patients, rejection rate, graft survival, and death-censored graft survival were lower and the patient survival was similar. Based on their results, they also suggested that JCV reactivation occurs in the native kidney on immunosuppression rather than in the donor-derived graft in contrast to BKV [52]. Another important difference between BKV PyVAN and JCV PyVAN is the strong association with viremia and the severity of histological pattern in the former [75]. On the contrary, low level of JCV viremia has been reported either in patients shedding large amounts of JCV in urine or in patients with parenchymal involvement and this may be related to fundamental differences between BKV and JCV biology, which remain presently unexplained [26, 38].
5. Conclusion
In conclusion, very few studies have been published regarding the replication of JCV in transplant patients. However, it is clear that JCV PyVAN is a unique clinical entity that needs to be differentiated from BKV PyVAN. This requires viral typing methods that are not widely available and this should account for an underestimation of its incidence in kidney transplant recipients. However, the protracted and nonaggressive clinical course of the disease and the favorable outcome should be considered once this form of PyVAN is diagnosed. Thus, monitoring of JCV infection, especially during the first 24 months after transplantation, is recommended.
References
- 1.Imperiale MJ. The human polyomaviruses: an overview. In: Khalili K, Stoner GL, editors. Human Polyomaviruses: Molecular and Clinical Perspective. chapter 5. New York, NY, USA: John Wiley & Sons; 2001. pp. 53–71. [Google Scholar]
- 2.Padgett BL, Walker DL, ZuRhein GM, Eckroade RJ, Dessel BH. Cultivation of papova-like virus from human brain with progressive multifocal leucoencephalopathy. Lancet. 1971;1(7712):1257–1260. doi: 10.1016/s0140-6736(71)91777-6. [DOI] [PubMed] [Google Scholar]
- 3.Ahsan N, Shah KV. Polyomaviruses: an overview. Graft. 2002;5:9–18. [Google Scholar]
- 4.Ahsan N, Shah KV. Polyomaviruses and human diseases. Advances in Experimental Medicine and Biology. 2006;577:1–18. doi: 10.1007/0-387-32957-9_1. [DOI] [PubMed] [Google Scholar]
- 5.Khalili K, White MK. Human demyelinating disease and the polyomavirus JCV. Multiple Sclerosis. 2006;12(2):133–142. doi: 10.1191/135248506ms1264oa. [DOI] [PubMed] [Google Scholar]
- 6.Khalili K, Del Valle L, Otte J, Weaver M, Gordon J. Human neurotropic polyomavirus, JCV, and its role in carcinogenesis. Oncogene. 2003;22(33):5181–5191. doi: 10.1038/sj.onc.1206559. [DOI] [PubMed] [Google Scholar]
- 7.Raj GV, Khalili K. Transcriptional regulation: lessons from the human neurotropic polyomavirus, JCV. Virology. 1995;213(2):283–291. doi: 10.1006/viro.1995.0001. [DOI] [PubMed] [Google Scholar]
- 8.Egli A, Infanti L, Dumoulin A, et al. Prevalence of polyomavirus BK and JC infection and replication in 400 healthy blood donors. Journal of Infectious Diseases. 2009;199(6):837–846. doi: 10.1086/597126. [DOI] [PubMed] [Google Scholar]
- 9.Clayson ET, Brando LVJ, Compans RW. Release of simian virus 40 virions from epithelial cells is polarized and occurs without cell lysis. Journal of Virology. 1989;63(5):2278–2288. doi: 10.1128/jvi.63.5.2278-2288.1989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Perez-Liz G, Del Valle L, Gentilella A, Croul S, Khalili K. Detection of JC virus DNA fragments but not proteins in normal brain tissue. Annals of Neurology. 2008;64(4):379–387. doi: 10.1002/ana.21443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Caldarelli-Stefano R, Vago L, Omodeo-Zorini E, et al. Detection and typing of JC virus in autopsy brains and extraneural organs of AIDS patients and non-immunocompromised individuals. Journal of NeuroVirology. 1999;5(2):125–133. doi: 10.3109/13550289909021994. [DOI] [PubMed] [Google Scholar]
- 12.Molloy ES, Calabrese LH. Progressive multifocal leukoencephalopathy: a national estimate of frequency in systemic lupus erythematosus and other rheumatic diseases. Arthritis and Rheumatism. 2009;60(12):3761–3765. doi: 10.1002/art.24966. [DOI] [PubMed] [Google Scholar]
- 13.Berger JR. Progressive multifocal leukoencephalopathy and newer biological agents. Drug Safety. 2010;33(11):969–983. doi: 10.2165/11537510-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 14.Berger JR, Kaszovitz B, Post MJD, Dickinson G. Progressive multifocal leukoencephalopathy associated with human immunodeficiency virus infection: a review of the literature with a report of sixteen cases. Annals of Internal Medicine. 1987;107(1):78–87. doi: 10.7326/0003-4819-107-1-78. [DOI] [PubMed] [Google Scholar]
- 15.Koralnik IJ, Wüthrich C, Dang X, et al. JC virus granule cell neuronopathy: a novel clinical syndrome distinct from progressive multifocal leukoencephalopathy. Annals of Neurology. 2005;57(4):576–580. doi: 10.1002/ana.20431. [DOI] [PubMed] [Google Scholar]
- 16.Viallard JF, Ellie E, Lazaro E, Lafon ME, Pellegrin JL. JC virus meningitis in a patient with systemic lupus erythematosus. Lupus. 2005;14(12):964–966. doi: 10.1191/0961203305lu2229cr. [DOI] [PubMed] [Google Scholar]
- 17.Blake K, Pillay D, Knowles W, Brown DWG, Griffiths PD, Taylor B. JC virus associated meningoencephalitis in an immunocompetent girl. Archives of Disease in Childhood. 1992;67(7):956–957. doi: 10.1136/adc.67.7.956. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Behzad-Behbahani A, Klapper PE, Vallely PJ, Cleator GM, Bonington A. BKV-DNA and JCV-DNA in CSF of patients with suspected meningitis or encephalitis. Infection. 2003;31(6):374–378. doi: 10.1007/s15010-003-3078-5. [DOI] [PubMed] [Google Scholar]
- 19.Fontoura P, Vale J, Lima C, Scaravilli F, Guimarães J. Progressive myoclonic ataxia and JC virus encephalitis in an AIDS patient. Journal of Neurology Neurosurgery and Psychiatry. 2002;72(5):653–656. doi: 10.1136/jnnp.72.5.653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Tallantyre EC, Paine SML, Sharp CP, Lowe JS, Gran B. Atypical progressive multifocal leukoencephalopathy associated with an unusual JC polyomavirus mutation. Archives of Neurology. 2009;66(8):1021–1024. doi: 10.1001/archneurol.2009.94. [DOI] [PubMed] [Google Scholar]
- 21.Husseiny MI, Anastasi B, Singer J, Lacey SF. A comparative study of Merkel cell, BK and JC polyomavirus infections in renal transplant recipients and healthy subjects. Journal of Clinical Virology. 2010;49(2):137–140. doi: 10.1016/j.jcv.2010.06.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Drachenberg CB, Hirsch HH, Papadimitriou JC, et al. Polyomavirus BK versus JC replication and nephropathy in renal transplant recipients: a prospective evaluation. Transplantation. 2007;84(3):323–330. doi: 10.1097/01.tp.0000269706.59977.a5. [DOI] [PubMed] [Google Scholar]
- 23.López V, Gutiérrez C, Burgos D, et al. Prospective study of infection and nephropathy due to BK and JC polyomavirus in 76 kidney transplant recipients. Transplantation Proceedings. 2008;40(9):2927–2929. doi: 10.1016/j.transproceed.2008.08.098. [DOI] [PubMed] [Google Scholar]
- 24.Helanterä I, Ortiz F, Auvinen E, et al. Polyomavirus BK and JC infections in well matched Finnish kidney transplant recipients. Transplant International. 2009;22(7):688–693. doi: 10.1111/j.1432-2277.2009.00847.x. [DOI] [PubMed] [Google Scholar]
- 25.Yin WY, Lu MC, Lee MC, Liu SC, Lin TY, Lai NS. A correlation between polyomavirus JC virus quantification and genotypes in renal transplantation. American Journal of Surgery. 2010;200(1):53–58. doi: 10.1016/j.amjsurg.2009.03.017. [DOI] [PubMed] [Google Scholar]
- 26.Lopez V, Gutierrez C, Sola E, et al. Does JC polyomavirus cause nephropathy in renal transplant patients? Transplantation Proceedings. 2010;42(8):2889–2891. doi: 10.1016/j.transproceed.2010.07.061. [DOI] [PubMed] [Google Scholar]
- 27.Hu JH, Zhao H, Huang YP, et al. Opportunistic posttransplantation virus infections in renal transplant recipients. Transplantation Proceedings. 2011;43(10):3715–3719. doi: 10.1016/j.transproceed.2011.07.024. [DOI] [PubMed] [Google Scholar]
- 28.Pires EP, Bernardino-Vallinoto CV, Alves DM, et al. Prevalence of infection by JC and BK polyomaviruses in kidney transplant recipients and patients with chronic renal disease. Transplant Infectious Disease. 2011;13(6):633–637. doi: 10.1111/j.1399-3062.2011.00614.x. [DOI] [PubMed] [Google Scholar]
- 29.Mengelle C, Kamar N, Mansuy JM, et al. JC virus DNA in the peripheral blood of renal transplant patients: a 1-year prospective follow-up in France. Journal of Medical Virology. 2011;83(1):132–136. doi: 10.1002/jmv.21951. [DOI] [PubMed] [Google Scholar]
- 30.Taheri S, Kafilzadeh F, Shafa M, et al. Comparison of polyomavirus (BK virus and JC viruses) viruria in renal transplant recipients with and without kidney dysfunction. Journal of Research in Medical Sciences. 2011;16(7):916–922. [PMC free article] [PubMed] [Google Scholar]
- 31.Saundh BK, Tibble S, Baker R, Sasnauskas K, Harris M, Hale A. Different patterns of BK and JC polyomavirus reactivation following renal transplantation. Journal of Clinical Pathology. 2010;63(8):714–718. doi: 10.1136/jcp.2009.074864. [DOI] [PubMed] [Google Scholar]
- 32.Gardner SD. Implication of papovaviruses in human diseases. In: Kurstak E, Kurstak C, editors. Comparative Diagnosis of Viral Disease, I. Human and Related Viruses. part A, chapter 3. New York, NY, USA: Academic Press; 1977. pp. 41–84. [Google Scholar]
- 33.Hogan TF, Borden EC, McBain JA. Human polyomavirus infections with JC virus and BK virus in renal transplant patients. Annals of Internal Medicine. 1980;92(3):373–378. doi: 10.7326/0003-4819-92-3-373. [DOI] [PubMed] [Google Scholar]
- 34.Gardner SD, Mackenzie EFD, Smith C, Porter AA. Prospective study of the human polyomavirus BK and JC and cytomegalovirus in renal transplant recipients. Journal of Clinical Pathology. 1984;37(5):578–586. doi: 10.1136/jcp.37.5.578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Randhawa P, Uhrmacher J, Pasculle W, et al. A comparative study of BK and JC virus infections in organ transplant recipients. Journal of Medical Virology. 2005;77(2):238–243. doi: 10.1002/jmv.20442. [DOI] [PubMed] [Google Scholar]
- 36.Delbue S, Ferraresso M, Elia F, et al. Investigation of polyomaviruses replication in pediatric patients with nephropathy receiving rituximab. Journal of Medical Virology. 2012;84(9):1464–1470. doi: 10.1002/jmv.23339. [DOI] [PubMed] [Google Scholar]
- 37.Baksh FK, Finkelstein SD, Swalsky PA, Stoner GL, Ryschkewitsch CF, Randhawa P. Molecular genotyping of BK and JC viruses in human polyomavirus-associated interstitial nephritis after renal transplantation. American Journal of Kidney Diseases. 2001;38(2):354–365. doi: 10.1053/ajkd.2001.26101. [DOI] [PubMed] [Google Scholar]
- 38.Razonable RR, Brown RA, Humar A, Covington E, Alecock E, Paya CV. A longitudinal molecular surveillance study of human polyomavirus viremia in heart, kidney, liver, and pancreas transplant patients. Journal of Infectious Diseases. 2005;192(8):1349–1354. doi: 10.1086/466532. [DOI] [PubMed] [Google Scholar]
- 39.Kusne S, Vilchez RA, Zanwar P, et al. Polyomavirus JC urinary shedding in kidney and liver transplant recipients associated with reduced creatinine clearance. Journal of Infectious Diseases. 2012;206(6):875–880. doi: 10.1093/infdis/jis469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Brinkert F, Briem-Richter A, Ilchmann C, Kemper MJ, Ganschow R. Prevalence of polyomavirus viruria (JC virus/BK virus) in children following liver transplantation. Pediatric Transplantation. 2010;14(1):105–108. doi: 10.1111/j.1399-3046.2009.01139.x. [DOI] [PubMed] [Google Scholar]
- 41.Muñoz P, Fogeda M, Bouza E, Verde E, Palomo J, Bañares R. Prevalence of BK virus replication among recipients of solid organ transplants. Clinical Infectious Diseases. 2005;41(12):1720–1725. doi: 10.1086/498118. [DOI] [PubMed] [Google Scholar]
- 42.Doucette KE, Pang XL, Jackson K, et al. Prospective monitoring of bk polyomavirus infection early posttransplantation in nonrenal solid organ transplant recipients. Transplantation. 2008;85(12):1733–1736. doi: 10.1097/TP.0b013e3181722ead. [DOI] [PubMed] [Google Scholar]
- 43.Antonsson A, Pawlita M, Feltkamp MC, et al. Longitudinal study of seroprevalence and serostability of the human polyomaviruses JCV and BKV in organ transplant recipients. Journal of Medical Virology. 2013;85(2):327–335. doi: 10.1002/jmv.23472. [DOI] [PubMed] [Google Scholar]
- 44.Kamar N, Mengelle C, Rostaing L. Incidence of JC-virus replication after rituximab therapy in solid-organ transplant patients. American Journal of Transplantation. 2009;9(1):244–245. doi: 10.1111/j.1600-6143.2008.02499.x. [DOI] [PubMed] [Google Scholar]
- 45.Thomas LD, Vilchez RA, White ZS, et al. A prospective longitudinal study of polyomavirus shedding in lung-transplant recipients. Journal of Infectious Diseases. 2007;195(3):442–449. doi: 10.1086/510625. [DOI] [PubMed] [Google Scholar]
- 46.Crowder CD, Gyure KA, Drachenberg CB, et al. Successful outcome of progressive multifocal leukoencephalopathy in a renal transplant patient. American Journal of Transplantation. 2005;5(5):1151–1158. doi: 10.1111/j.1600-6143.2005.00800.x. [DOI] [PubMed] [Google Scholar]
- 47.Hix JK, Braun WE, Isada CM. Delirium in a renal transplant recipient associated with BK virus in the cerebrospinal fluid. Transplantation. 2004;78(9):1407–1408. doi: 10.1097/01.tp.0000137106.09925.8b. [DOI] [PubMed] [Google Scholar]
- 48.Cabrejo L, Diop M, Blohorn-Sense A, Mihout B. Progressive BK virus associated multifocal leukoencephalopathy in an immunocompromised patient treated with corticosteroids. Revue Neurologique. 2005;161(3):326–330. doi: 10.1016/s0035-3787(05)85040-4. [DOI] [PubMed] [Google Scholar]
- 49.Nickeleit V, Hirsch HH, Zeiler M, et al. BK-virus nephropathy in renal transplants—tubular necrosis, MHC-class II expression and rejection in a puzzling game. Nephrology Dialysis Transplantation. 2000;15(3):324–332. doi: 10.1093/ndt/15.3.324. [DOI] [PubMed] [Google Scholar]
- 50.Nickeleit V, Singh HK, Mihatsch MJ. Polyomavirus nephropathy: morphology, pathophysiology, and clinical management. Current Opinion in Nephrology and Hypertension. 2003;12(6):599–605. doi: 10.1097/00041552-200311000-00005. [DOI] [PubMed] [Google Scholar]
- 51.Mengel M, Marwedel M, Radermacher J, et al. Incidence of polyomavirus-nephropathy in renal allografts: influence of modern immunosuppressive drugs. Nephrology Dialysis Transplantation. 2003;18(6):1190–1196. doi: 10.1093/ndt/gfg072. [DOI] [PubMed] [Google Scholar]
- 52.Bohl DL, Storch GA, Ryschkewitsch C, et al. Donor origin of BK virus in renal transplantation and role of HLA C7 in susceptibility to sustained BK viremia. American Journal of Transplantation. 2005;5(9):2213–2221. doi: 10.1111/j.1600-6143.2005.01000.x. [DOI] [PubMed] [Google Scholar]
- 53.Hirsch HH, Steiger J. Polyomavirus BK. Lancet Infectious Diseases. 2003;3(10):611–623. doi: 10.1016/s1473-3099(03)00770-9. [DOI] [PubMed] [Google Scholar]
- 54.Hirsch HH. Polyomavirus BK nephropathy: a (re-)emerging complication in renal transplantation. American Journal of Transplantation. 2002;2(1):25–30. doi: 10.1034/j.1600-6143.2002.020106.x. [DOI] [PubMed] [Google Scholar]
- 55.Randhawa P, Baksh F, Aoki N, Tschirhart D, Finkelstein S. JC virus infection in allograft kidneys: analysis by polymerase chain reaction and immunohistochemistry. Transplantation. 2001;71(9):1300–1303. doi: 10.1097/00007890-200105150-00020. [DOI] [PubMed] [Google Scholar]
- 56.Kazory A, Ducloux D, Chalopin JM, Angonin R, Fontanière B, Moret H. The first case of JC virus allograft nephropathy. Transplantation. 2003;76(11):1653–1655. doi: 10.1097/01.TP.0000090749.42791.14. [DOI] [PubMed] [Google Scholar]
- 57.Wen MC, Wang CL, Wang M, et al. Association of JC virus with tubulointerstitial nephritis in a renal allograft recipient. Journal of Medical Virology. 2004;72(4):675–678. doi: 10.1002/jmv.20037. [DOI] [PubMed] [Google Scholar]
- 58.Dörries K, Ter Meulen V. Progressive multifocal leucoencephalopathy: detection of papovavirus JC in kidney tissue. Journal of Medical Virology. 1983;11(4):307–317. doi: 10.1002/jmv.1890110406. [DOI] [PubMed] [Google Scholar]
- 59.Kantarci G, Eren Z, Demirağ A, Dogan I, Çakalagaoglu F, Yilmaz G. JC virus-associated nephropathy in a renal transplant recipient and comparative analysis of previous cases. Transplant Infectious Disease. 2011;13(1):89–92. doi: 10.1111/j.1399-3062.2010.00567.x. [DOI] [PubMed] [Google Scholar]
- 60.Polo C, Pérez JL, Mielnichuck A, Fedele CG, Niubó J, Tenorio A. Prevalence and patterns of polyomavirus urinary excretion in immunocompetent adults and children. Clinical Microbiology and Infection. 2004;10(7):640–644. doi: 10.1111/j.1469-0691.2004.00882.x. [DOI] [PubMed] [Google Scholar]
- 61.Rossi A, Delbue S, Mazziotti R, et al. Presence, quantitation and characterization of JC virus in the urine of Italian immunocompetent subjects. Journal of Medical Virology. 2007;79(4):408–412. doi: 10.1002/jmv.20829. [DOI] [PubMed] [Google Scholar]
- 62.Kitamura T, Yogo Y, Kunitake T, Suzuki K, Tajima A, Kawabe K. Effect of immunosuppression on the urinary excretion of BK and JC polyomaviruses in renal allograft recipients. International Journal of Urology. 1994;1(1):28–32. doi: 10.1111/j.1442-2042.1994.tb00004.x. [DOI] [PubMed] [Google Scholar]
- 63.Randhawa P, Vats A, Shapiro R. Monitoring for polyomavirus BK and JC in urine: comparison of quantitative polymerase chain reaction with urine cytology. Transplantation. 2005;79(8):984–986. doi: 10.1097/01.tp.0000157573.90090.fd. [DOI] [PubMed] [Google Scholar]
- 64.Binet I, Nickeleit V, Hirsch HH, et al. Polyomavirus disease under new immunosuppressive drugs: a cause of renal graft dysfunction and graft loss. Transplantation. 1999;67(6):918–922. doi: 10.1097/00007890-199903270-00022. [DOI] [PubMed] [Google Scholar]
- 65.Behzad-Behbahani A, Klapper PE, Vallely PJ, Cleator GM, Khoo SH. Detection of BK virus and JC virus DNA in urine samples from immunocompromised (HIV-infected) and immunocompetent (HIV-non-infected) patients using polymerase chain reaction and microplate hybridisation. Journal of Clinical Virology. 2004;29(4):224–229. doi: 10.1016/S1386-6532(03)00155-0. [DOI] [PubMed] [Google Scholar]
- 66.Kazory A, Ducloux D. Renal transplantation and polyomavirus infection: recent clinical facts and controversies. Transplant Infectious Disease. 2003;5(2):65–71. doi: 10.1034/j.1399-3062.2003.00017.x. [DOI] [PubMed] [Google Scholar]
- 67.Doerries K. Human polyomavirus JC and BK persistent infection. Advances in Experimental Medicine and Biology. 2006;577:102–116. doi: 10.1007/0-387-32957-9_8. [DOI] [PubMed] [Google Scholar]
- 68.Knowles WA. Discovery and epidemiology of the human polyomaviruses BK virus (BKV) and JC virus (JCV) Advances in Experimental Medicine and Biology. 2006;577:19–45. doi: 10.1007/0-387-32957-9_2. [DOI] [PubMed] [Google Scholar]
- 69.Phillips T, Jacobs R, Ellis EN. Polyoma nephropathy and progressive multifocal leukoencephalopathy in a renal transplant recipient. Journal of Child Neurology. 2004;19(4):301–304. doi: 10.1177/088307380401900412. [DOI] [PubMed] [Google Scholar]
- 70.Mateen FJ, Muralidharan R, Carone M, et al. Progressive multifocal leukoencephalopathy in transplant recipients. Annals of Neurology. 2011;70(2):305–322. doi: 10.1002/ana.22408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Kamar N, Milioto O, Puissant-Lubrano B, et al. Incidence and predictive factors for infectious disease after rituximab therapy in kidney-transplant patients. American Journal of Transplantation. 2010;10(1):89–98. doi: 10.1111/j.1600-6143.2009.02785.x. [DOI] [PubMed] [Google Scholar]
- 72.Rinaldi L, Rinaldi F, Perini P, et al. No evidence of JC virus reactivation in natalizumab treated multiple sclerosis patients: an 18 month follow-up study. Journal of Neurology, Neurosurgery and Psychiatry. 2010;81(12):1345–1350. doi: 10.1136/jnnp.2009.201079. [DOI] [PubMed] [Google Scholar]
- 73.Warnke C, Menge T, Hartung HP, et al. Natalizumab and progressive multifocal leukoencephalopathy: what are the causal factors and can it be avoided? Archives of Neurology. 2010;67(8):923–930. doi: 10.1001/archneurol.2010.161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Cheng XS, Bohl DL, Storch GA, et al. Inhibitory interactions between BK and JC virus among kidney transplant recipients. Journal of the American Society of Nephrology. 2011;22(5):825–831. doi: 10.1681/ASN.2010080877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Hirsch HH, Knowles W, Dickenmann M, et al. Prospective study of polyomavirus type BK replication and nephropathy in renal-transplant recipients. New England Journal of Medicine. 2002;347(7):488–496. doi: 10.1056/NEJMoa020439. [DOI] [PubMed] [Google Scholar]