

Abstract
Menopause is a physiological process typically occurring in the fifth decade of life. One of the most annoying oral symptoms in this age group is the burning mouth syndrome (BMS), which may be defined as an intraoral burning sensation occurring in the absence of identifiable oral lesion or laboratory findings. Pain in burning mouth syndrome may be described as burning, tender, tingling, hot, scalding, and numb sensation in the oral mucosa. Multiple oral sites may be involved, but the anterior two-third part and the tip of tongue are most commonly affected site. There is no definite etiology for BMS other than the precipitating causative factors, and it is still considered idiopathic. Various treatment options like use of benzodiazepine, anti-depressants, analgesics, capsaicin, alpha lipoic acids, and cognitive behavioral therapy are found to be effective, but definite treatment is still unknown. The present article discusses some of the recent concepts of etiopathogenesis of BMS as well as the role of pharmacotherapeutic management in this disorder.
Keywords: Burning mouth syndrome, menopause, stomatodynia, oral mucosa
INTRODUCTION
India is the second most populated country after China. It has been estimated that by the year 2026 the population of India will become 1.4 billion, 173 million people will have age over 60 years, and 103 million individuals will account for the menopausal population.[1] This increasing rate of menopausal population and its association with other systemic diseases like osteoporosis, cardiovascular disease, breast cancer, cervix cancer etc., has forced us to think about other problems of this particular group.
The signs and symptoms of menopause largely depend upon the life style, rural-urban division, and economical status. Uro-genital symptoms, fatigue, and body pains are some common complaints in both rural and urban menopausal women, whereas hot flushes, psychological symptoms, mood swings, and sexual dysfunction are predominantly seen in urban women. Among oro-dental problems, gingival bleeding, receding gums, loose teeth, and burning sensation in oral mucosa are some common problems in menopausal women.[2]
The burning sensation in normal oral mucosa is known as “burning mouth syndrome” (BMS) and occurs particularly in postmenopausal women.[3] Various diseases/clinical entities like lichen planus, candidiasis, viral infections, xerostomia etc., also have a characteristic symptom of burning sensation, but in burning mouth syndrome, pain is accompanied without any alteration in oral mucosa. International Association for the Study of Pain defined burning mouth syndrome (BMS) as a burning pain in the tongue and/or other oral mucous membrane in an absence of clinical signs or laboratory findings.[4] The term burning mouth syndrome should only be used when a definite cause has not been found.[5]
Scala A et al. suggested two clinical forms of BMS. Primary BMS/essential/idiopathic BMS, for which organic local/systemic causes cannot be identified and secondary BMS resulting from local/systemic pathological conditions and thus this form responds well to the etiology-directed therapy.[6]
The aim of this review article is to search for various possible etiological factors and treatment modalities of this enigmatic condition, especially in relation to menopausal women. This review is based on the evidences from electronic and manual search. The following keywords were used for the search: Burning mouth syndrome, glossodynia, sore mouth, menopause, and only relevant articles in English language were selected for the study.
Epidemiology and site specificity
Most of studies suggested that majority of patients with burning mouth syndrome are middle-aged women in post-menopausal phase. The female/male ratio of occurrence of BMS is 7:1.[7,8] The prevalence of burning mouth symptoms as reported from international studies ranges from 0.6% to 15%.[9] The prevalence in the general population is 3.7% (1.6% men and 5.5% women).[3] Most of the investigators agreed to the point that the prevalence of BMS increases with age in both males and females, with this syndrome mainly affecting females in the fifth to seventh decade.[3,10] BMS usually presents 3 years before to 12 years following menopause[8] and rarely before the age of 30.[3,11]
BMS can involve multiple sites, but the tip of the tongue is the most common location (71%), followed by lips (50%), lateral border of tongue, (46%) and palate (46%).[12]
Pain characteristics in burning mouth syndrome
The onset of pain can be either gradual and spontaneous or sudden and related to a precipitating event. Patients usually report that the burning sensation presents its lowest intensity upon waking up, but reappears after the first meal of the day. Once begun, it is continuous, reaching the maximum intensity by late evening.[8,13] Patients do not normally wake up during the night, but do find it difficult to get to sleep. These patients often present mood changes, including irritability, anxiety, and depression.[14] Grushka M et al. reported that some patients complain of sleep onset and may wake up during the sleep because of pain.[15] The pain of BMS is found to be associated with consumption of hot/spicy food, too much speaking, stressful life and subsides with cold food, work, and distraction. BMS generally presents as a triad: Mouth pain, alteration in taste, and altered salivation, in the absence of visible mucosal lesions in the mouth.[16]
In 1994, Lamey, et al. classified the syndrome into 3 types: Type 1 (35%), defined by daily pain where symptoms are absent upon awakening but gradually increase in severity as the day progresses, unrelated to psychiatric conditions. Type 2 (55%) is defined by constant pain present during day and night; these patients are very anxious. Type 3 (10%) is defined by intermittent pain, with pain-free intervals, occurring in non-usual sites such as the floor of mouth and the posterior oropharynx; in this type, there is a relation between pain and the type of food taken as well as allergens.[17]
Etiology and diagnosis of burning mouth syndrome
Burning sensations in oral tissues might be associated with a large number of local and systemic factors like candida infections, lichen planus, xerostomia, oral galvanism, parafunctional habits such as tongue thrust, diabetes, side effects of drug therapy etc., [Figure 1]. But, the term “burning mouth syndrome” or a true “BMS” should be applied only if burning sensation occurs on a clinically healthy oral mucosa in the absence of all aforementioned known local and systemic factors.
Figure 1.
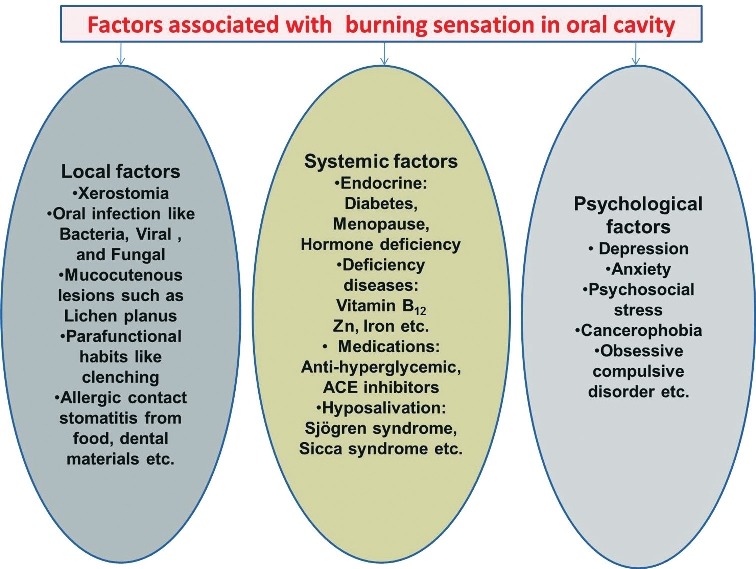
Factors associated with burning sensation in the oral cavity
Mínguez-Sanz MP, et al. proposed 3 hypotheses for the etiology of burning mouth syndrome. A first hypothesis suggests that neuronal inflammation may be mediated by a classical axonal reflex that would activate a group of nociceptors, causing them to release neuropeptides at trigeminal terminal branch level. A second hypothesis points suggests the existence of an indirect reflex that would develop in the afferent nerves of the oral cavity, followed by processing at central level in the trigeminal nerve, and the induction of a response at autonomic nervous system level. The third hypothesis is related to the capsaicin receptors, which have dual efferent and sensory activities. These receptors, which are found in the C-polymodal nociceptors, would be implicated in the regulation of the events associated to neurogenic inflammation and would be activated upon receiving afferent signals and the simultaneous release of neuropeptides from the same nerve endings.[18]
The pain of BMS is found to be associated with consumption of hot/spicy food, too much speaking, stressful life etc., but the exact etiology of burning mouth syndrome is not known. Some investigators believe it to be associated with some neuropathic pain. One of the most widely accepted theories is that the partial or total loss of chorda tympani (facial) nerve function disinhibits the trigeminal nerve, resulting in pain along trigeminal pathways, as both taste and pain systems are regulated by interneurons of the central nervous system (CNS).[3,19]
More recently, an enticing hypothesis has been proposed that burning mouth syndrome is associated with an alteration of gonadal, adrenal, and neuroactive steroid levels. Woda et al. suggested that chronic anxiety or stress results in a dysregulation of adrenal steroids, a reduction in adrenal steroids will, in turn, lead to an altered production of neuroactive steroids in skin, mucosa, and the nervous system.[20] The relationship with menopause is proven by the suggestion that the dramatic fall in gonadal steroids that occurs at that time further alters the production of neuroactive steroids. But, the exact etiopathogenesis still remains largely obscure.
Chemenos E, et al. correlated the symptoms of BMS with composition and flow of saliva. It is supposed that at local level, qualitative and quantitative salivary changes such as hypo-salivation, altered concentrations of certain salivary proteins, and increased viscosity and increased pH of saliva could possibly contribute to the alteration of salivary lubricant function and oral mucosal perception.[21]
A through and comprehensive history along with clinical examination and laboratory tests is the key to diagnosis of BMS.
History should include:
Duration, intensity, location, aggravating, and relieving factors of pain
Taste alteration and dry mouth
Current and past health status like hypertension, diabetes etc.
Medications (current and past) Clinical examination should include:
Intraoral examination, which includes inspection of oral mucosa and tongue for any lesion, swelling, change in color etc.
Palpation of muscles of mastication
Examination of dental hard and soft tissues
Temporo-mandibular joint examination Lab test should include:
Hematological test: Complete blood count, glucose test, thyroid test etc.
Oro – microbial culture for fungal, viral, and bacterial infections
Allergy testing
Salivary flow rate tests
MRI, CT scans, and nuclear medicine test to rule out systemic diseases/disorders.
Management
Due to multifactorial nature of BMS, it usually requires an organized approach to take the various etiologies into account. The management of BMS requires help from one or a variety of medical specialties like dentists, ENT specialist, dermatologist, endocrinologist etc.
The treatment of burning mouth syndrome is usually directed at its symptoms.
Pain, which is the most important symptoms in BMS, is usually controlled by the use of low dose of centrally acting medications like benzodiazepine, tricyclic anti-depressants, gabapentin etc., Grushka et al. suggested that the best treatment for the syndrome consists of a combination of drugs, such as clonazepam, gabapentinn and baclofen.[22] Gremeau-Richard, in 2004, reported significantly reduction in pain with topical application of clonazepam in patients with BMS.[23] Heckmann SM et al. conducted a double-blind study on clonazepam in patients with BMS. They found that patients on clonazepam (0.5 mg/day) were significantly improved in pain rating as compared to placebo (lactose).[24] Sardella A et al., in their prospective, randomized, double blind, placebo-controlled study, investigated the effect of Hypericum perforatum (popularly known as St. john's wort) extracts in patients with BMS. But, no statistically significant differences were observed in VAS scores between active treatment and placebo.[25]
Local application of desensitizing agents like topical capsaicin: The use of hot pepper sauce (a good source of capsaicin) in water in the ratio of 1:2 is also found to be effective in reducing oral pain in BMS. Epstein and Marcoe recommended 3-4 times/day application for partial or even complete remission of pain. Capsaicin acts by depletion of substance p, so results in decreased peripheral burning.[26]
Hormone replacement therapy (HRT): Volpe et al., in his study on postmenopausal women, found that 12 out of 22 patients experienced improvement in oral symptoms after estradiol-based treatment.[27] It has been found that women with symptoms of burning and estrogen receptors in the oral mucosa respond to hormone replacement, while this does not occur in patients without these receptors; however, it cannot be guaranteed that HRT could be an effective treatment for the oral symptomatology.[14]
High fluid diet
Nutritional supplements and antioxidative therapy: Femiano et al. in 2002 have shown the use of alpha lipoic acid in management of BMS. 96% of patients had shown significant improvement in their symptoms. It is a potent antioxidant and neuroprotective agent.[28] But, Cavalcanti DR et al., in their randomized, double-blind, placebo-controlled trial of 38 patients, didn’t find effectiveness of alpha lipoic acid, in comparison with the control group given placebo, in the management of BMS.[29] Similar non-significant differences were reported by Lopez-Jornet P et al. in alpha lipoic acid group (800 mg/day for 8 weeks) and placebo group.[30]
Last but not the least is the cognitive behavioral therapy (CBT): The patients of burning mouth syndrome should be reassured that this condition is not fatal nor it is cancerous, and it will eventually resolve itself. Bergdahl et al. suggested the use of cognitive behavioral therapy for BMS patients. He found reduction in pain intensity following CBT immediately, following therapy.[31] Mock D et al.[32] and Reamy BV et al.[33] found the combination of cognitive behavioral therapy (CBT), alpha-lipoic acid, and/or clonazepam as the most promising approach for the treatment of burning mouth syndrome.
Mínguez-Serra MP et al. reviewed the pharmacological treatments used in the last 10 years to reduce the symptoms of BMS. They found that capsaicin and clonazepam, administered systemically via the oral route, can be discarded because of their adverse reactions. Gabapentin didn’t show its efficacy in alleviation of pain while alpha-lipoic acid appeared useful, but it loses its efficacy over time. Benzidamine and trazodone were not found to be better than placebo in the treatment of BMS. With amisulpiride, paroxetine, sertraline, and sucralfate, the patients reported improvement-though the study designs were deficient. Topical clonazepam presently seems to be the best option, with healing of almost half of all patients (40%).[34]
Sengupta P in his work “Health Impacts of Yoga and Pranayam: A State-of-the-Art Review” advocated the use of the holistic science of yoga for prevention and management of stress and other stress-induced disorders. He found beneficial health impact of yoga in treatment of depression, mood alterations, neuro-hormonal activity, diabetes, and coronary atherosclerosis.[35] But, further long term clinical trials are needed to document the effects of yoga, especially in management of burning mouth syndrome.
CONCLUSION
Burning mouth syndrome still remains a poorly-understood condition in the field of oral medicine. This could be because of lack of universally accepted definition, which makes it a condition with multifactorial origin and often idiopathic. High incidence rate in middle age females (age group 40-60) clearly indicates its association with female sex hormones.
Pain, the major symptom of BMS, is largely controlled by the use of centrally-acting medications, anti-depressants, antioxidants, desensitizing agents, hormonal therapy, and cognitive behavioral therapy. But, the treatment of BMS is still empirical. More and more research work is required to explore new directions in the field of etiopathogenesis and management of BMS.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Unni J. Third consensus meeting of Menopause society (2008): A summary. Journal of Mid-life health. 2010;1:43–47. doi: 10.4103/0976-7800.66987. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Frutos R, Rodríguez S, Miralles-Jorda L, Machuca G. Oral manifestations and dental treatment in menopause. Med Oral. 2002;7:26–35. [PubMed] [Google Scholar]
- 3.Bergdahl M, Bergdahl J. Burning mouth syndrome: Prevalence and associated factors. J Oral Pathol Med. 1999;28:350–4. doi: 10.1111/j.1600-0714.1999.tb02052.x. [DOI] [PubMed] [Google Scholar]
- 4.Merskey H, Bogduk N. Classification of chronic pain. Seattle (WA): IASP Press; 1994. pp. 59–71. [Google Scholar]
- 5.ADA Division of Communications; Journal of the American Dental Association. Burning mouth syndrome. J Am Dent Assoc. 2005;136:1191. doi: 10.14219/jada.archive.2005.0324. [DOI] [PubMed] [Google Scholar]
- 6.Scala A, Checchi L, Montevecchi M, Marini I. Update on burning mouth syndrome: Overview and Patient management. Crit Rev Oral Biol Med. 2003;14:275–91. doi: 10.1177/154411130301400405. [DOI] [PubMed] [Google Scholar]
- 7.Ship JA, Grushka M, Lipton JA, Mott AE, Sessle BJ, Dionne RA. Burning mouth syndrome: An update. J Am Dent Assoc. 1995;126:842–53. doi: 10.14219/jada.archive.1995.0305. [DOI] [PubMed] [Google Scholar]
- 8.Grushka M. Clinical features of burning mouth syndrome. Oral Surg Oral Med Oral Pathol. 1987;63:30–6. doi: 10.1016/0030-4220(87)90336-7. [DOI] [PubMed] [Google Scholar]
- 9.Zakrzewska JM, Hamlyn PJ. Facial pain. In: Crombie IK, editor. Epidemiology of pain. Seattle (WA): IASP press; 1999. pp. 175–82. [Google Scholar]
- 10.Ferguson MM, Carter J, Boyle P, Hart DM, Lindsay R. Oral complaints related to climacteric symptoms in oophorectomized women. J R Soc Med. 1981;74:492–8. doi: 10.1177/014107688107400707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Van der Waal I. The burning mouth syndrome. Copenhagen: Munksgaard; 1990. pp. 5–90. [Google Scholar]
- 12.Miyamoto SA, Ziccardi VB. Burning Mouth syndrome. Mt Sinai J Med. 1998;65:343–7. [PubMed] [Google Scholar]
- 13.Grinspan D, Fernandez Blanco G, Allevato MA, Stengel FM. Burning mouth syndrome. Int J Dermatol. 1995;34:483–7. doi: 10.1111/j.1365-4362.1995.tb00617.x. [DOI] [PubMed] [Google Scholar]
- 14.López-Jornet P, Camacho-Alonso F, Andujar-Mateos P, Sánchez-Siles M, Gómez-Garcia F. Burning mouth syndrome: An update. Med Oral Patol Oral Cir Bucal. 2010;15:E562–8. doi: 10.4317/medoral.15.e562. [DOI] [PubMed] [Google Scholar]
- 15.Grushka M, Epstein JB, Gorsky M. Burning mouth syndrome. Am Fam Physician. 2002;65:615–20. [PubMed] [Google Scholar]
- 16.Cerchiari DP, Moricz RD, Sanjar FA, Rapoport PB, Moretti G, Guerra MM. Burning mouth syndrome: Etiology. Rev Bras Otorrinolaringol. 2006;72:419–24. doi: 10.1016/S1808-8694(15)30979-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lamey PJ, Lamb AB. Lip component of BMS. Oral Surg Oral Med Oral Pathol. 1994;78:590–3. doi: 10.1016/0030-4220(94)90169-4. [DOI] [PubMed] [Google Scholar]
- 18.Mínguez-Sanz MP, Salort-Llorca C, Silvestre-Donat FJ. Etiology of burning mouth syndrome: A review and update. Med Oral Patol Oral Cir Bucal. 2011;16:E144–8. doi: 10.4317/medoral.16.e144. [DOI] [PubMed] [Google Scholar]
- 19.Grushka M, Epstein JB, Gorsky M. Burning mouth syndrome and other oral sensory disorders: A unifying hypothesis. Pain Res Man. 2003;8:133–5. doi: 10.1155/2003/654735. [DOI] [PubMed] [Google Scholar]
- 20.Woda A, Dao T, Grémeau-Richard C. Steroid dys- regulation and stomatodynia (burning mouth syndrome) J Orofacial Pain. 2009;23:202–10. [PubMed] [Google Scholar]
- 21.Chimenos-Kustner E, Marques-Soares MS. Burning mouth and saliva. Med Oral. 2002;7:244–53. [PubMed] [Google Scholar]
- 22.Grushka M, Ching V, Epstein J. Burning Mouth Syndrome. Adv. Otorhinolaryngol. 2006;63:278–87. doi: 10.1159/000093766. [DOI] [PubMed] [Google Scholar]
- 23.Gremeau-Richard C, Woda A, Navez ML, Attal N, Bouhassira D, Gagnieu MC, et al. Topical clonazepam in stomatodynia: A randomized placebo-controlled study. Pain. 2004;108:51–7. doi: 10.1016/j.pain.2003.12.002. [DOI] [PubMed] [Google Scholar]
- 24.Heckmann SM, Kirchner E, Grushka M, Wichmann MG, Hummel T. A double-blind study on clonazepam in patients with burning mouth syndrome. Laryngoscope. 2012;122:813–6. doi: 10.1002/lary.22490. [DOI] [PubMed] [Google Scholar]
- 25.Sardella A, Lodi G, Demarosi F, Tarozzi M, Canegallo L, Carrassi A. Hypericum perforatum extract in burning mouth syndrome: A randomized placebo-controlled study. J Oral Pathol Med. 2008;37:395–401. doi: 10.1111/j.1600-0714.2008.00663.x. [DOI] [PubMed] [Google Scholar]
- 26.Epstein JB, Marcoe JH. Topical application of capsaicin for treatment of oral neuropathic pain and trigeminal neuralgia. Oral Surg Oral Med Oral Pathol. 1994;77:135–40. doi: 10.1016/0030-4220(94)90275-5. [DOI] [PubMed] [Google Scholar]
- 27.Volpe A, Lucenti V, Forabosco A. Oral discomfort and hormonal therapy in post menopause. Maturitus. 1991;13:1–5. doi: 10.1016/0378-5122(91)90279-y. [DOI] [PubMed] [Google Scholar]
- 28.Femiano F, Scully C. Burning mouth syndrome (BMS): Double blind controlled study of alpha-lipoic acid therapy. J Oral Pathol Med. 2002;31:267–9. doi: 10.1034/j.1600-0714.2002.310503.x. [DOI] [PubMed] [Google Scholar]
- 29.Cavalcanti DR, da Silveira FR. Alpha lipoic acid in burning mouth syndrome-a randomized double-blind placebo-controlled trial. J Oral Pathol Med. 2009;38:254–61. doi: 10.1111/j.1600-0714.2008.00735.x. [DOI] [PubMed] [Google Scholar]
- 30.López-Jornet P, Camacho-Alonso F, Leon-Espinosa S. Efficacy of alpha lipoic acid in burning mouth syndrome: A randomized, placebo-treatment study. J Oral Rehabil. 2009;36:52–7. doi: 10.1111/j.1365-2842.2008.01914.x. [DOI] [PubMed] [Google Scholar]
- 31.Bergdahl J, Anneroth G, Perris H. Cognitive therapy in the treatment of patients with resistant burning mouth syndrome: A controlled study. J Oral Pathol Med. 1995;24:213–5. doi: 10.1111/j.1600-0714.1995.tb01169.x. [DOI] [PubMed] [Google Scholar]
- 32.Mock D, Chugh D. Burning mouth syndrome. Int J Oral Sci. 2010;2:1–4. doi: 10.4248/IJOS10008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Reamy BV, Derby R, Bunt CW. Common tongue conditions in primary care. Am Fam Physician. 2010;81:627–34. [PubMed] [Google Scholar]
- 34.Mínguez Serra MP, Salort Llorca C, Silvestre Donat FJ. Pharmacological treatment of burning mouth syndrome: A review and update. Med Oral Patol Oral Cir Bucal. 2007;12:E299–304. [PubMed] [Google Scholar]
- 35.Sengupta P. Health impacts of yoga and pranayama: A state-of-the-art review. Int J Prev Med. 2012;3:444–58. [PMC free article] [PubMed] [Google Scholar]