

Abstract
PURPOSE
To test effects of parent/child training designed to increase calcium intake, bone-loading physical activity (PA), and bone density.
DESIGN
Two-group randomized controlled trial.
SETTING
Family-based intervention delivered at research center.
SUBJECTS
117 healthy children aged 10-13 years (58.1% female, 42.7% Hispanic, 40.2% White). Ninety-seven percent of participants had at least one parent graduate from high school and 37.2% had at least one parent graduate from a 4-year university.
INTERVENTION
Children and parents were randomly assigned to diet and exercise (experimental) or injury prevention (control) interventions. Children were taught in eight weekly classes how to engage in bone-loading PA and eat calcium-rich foods or avoid injuries. Parents were taught behavior management techniques to modify children’s behaviors.
MEASURES
Measures at baseline, three, nine and twelve months included 24-hour diet and PA recalls, and bone mineral density (BMD) by DXA.
ANALYSIS
ANOVA and Generalized Estimating Equations assessed group by time differences. Comparisons were conducted separately for boys and girls.
RESULTS
For boys, cross-sectional differences between experimental versus control group were achieved for 3 and 9-month calcium intake (1352 vs. 1052mg/day, 1298 vs. 970mg/day, p<0.05). For girls, marginal cross-sectional differences were achieved for high-impact PA at 12 months (p<0.10). For calcium intake, a significant group by time interaction was observed from pre to post test for the full sample (p=.008) and for girls (p=.006) but not for boys. No significant group by time differences in calcium were observed across the follow-up period. No group by time differences were observed for high impact physical activity. Among boys, longitudinal group by time differences reached significance for total hip BMD (p=.045) and femoral neck BMD (p=.033), even after adjusting for skeletal growth. Similar differential increases were observed among boys for BMC at the hip (p=.068) and total body (p=.054) regions. No significant group by time interaction effects were observed for girls at any bone site for BMD. For BMC, control girls showed a significant increase (p=.03) in spine BMC compared to intervention girls
CONCLUSION
This study demonstrated that parent/preteen training can increase calcium intake and attenuate the decline in high-impact PA. Results suggest that more powerful interventions are needed to increase activity levels and maximize bone mineral accrual during pre-adolescent years.
Keywords: Calcium, diet, parent education, physical activity, preteens, Osteoporosis prevention
INDEXING KEY WORDS: Manuscript format: research; Research purpose: intervention testing/ program evaluation; Study design: randomized trial; Outcome measure: behavioral, biometric; Setting: family; Health focus: fitness/physical activity, nutrition; Strategy: education, skill building/behavior change; Target population age: youth; Target population circumstances: geographic location
INTRODUCTION
Osteoporosis is a public health problem in the U.S. More than half of all women and as many as one-third of all men will experience an osteoporotic fracture at some point in their lives1. While it is commonly believed that osteoporosis is primarily a female disease, the incidence of hip fractures in men and women increases similarly with advancing age, although delayed by 5-10 years in men2. In absence of intervention, the number of individuals afflicted by this condition is projected to double or triple in the next 30 years owing to increased longevity and unhealthy lifestyles3.
Genetic factors are estimated to determine 60-80% of peak adult bone mass, leaving environmental and lifestyle factors as important contributors of 20-40% of bone mass4. Physical activity and diet, in addition to body weight and hormonal factors, are determinants of fracture susceptibility throughout life5. Studies involving increased intake of calcium-rich foods have consistently shown increased bone mass in children and adolescents6-11. However, an important issue is whether the gain in bone mass that can be achieved is retained post-intervention. Results from intervention studies of long-term effects of calcium intake are inconsistent12-15. It is likely that physical activity and adequate calcium intake need to be sustained to maintain gains in bone mass and strength.
Preventing osteoporosis may be accomplished by optimizing gains in bone mass and bone strength during adolescence, especially during the years of rapid linear growth5,16. In a cohort of Canadian youth aged 8-18 years, measured annually over seven years, the rate of bone mineral accrual was at its highest between approximately age 11-14 years, with girls showing an earlier peak rate by approximately 1.5 years17. By the age of 18 years, adolescents will have acquired 90% of their peak bone mass4. Osteoporosis may be considered a pediatric disorder that is manifested later in life18. It has been reported that each 5% increase in peak bone mass reduced the life-time risk of fracture by 40%4. Evidence from a cross-sectional study of pre-pubertal and retired female gymnasts suggests that vigorous impact exercise during childhood (mean age 10.4 years) may increase BMD and reduce fracture risk during adulthood by 25-50%19. Although longitudinal studies are needed to confirm these observations, the findings support early intervention to reduce future fracture risk.
The timing of exercise in terms of puberty may also be a determinant of the amount of bone mineral a child can accrue. Several exercise interventions in girls and boys during the pre- or early pubescent years showed significant net gains in bone mineral content (BMC) following 8-9 months of intervention20-22, whereas there is some evidence in girls that exercise after menarche may be less effective in promoting rapid bone mineralization23,24. Given the evidence mentioned above that children accrue bone mineral at an accelerated rate during the pre-teen years (and early teen years in boys), we targeted preteens for our intervention.
PURPOSE
Although there have been many studies of exercise and nutrition effects on BMD in adults, particularly in women, relatively few randomized, prospective studies have been conducted among children and adolescents, including both boys and girls16, 21, 22. Also, it is generally agreed that vigorous and high volume exercise associated with competitive sports can increase bone density, but less is known regarding the effects of more moderate exercise typical of non-athletic children. The purpose of this study was to determine whether parent and child training could increase calcium intake and bone-loading physical activity enough to increase bone density in pre-adolescent girls and boys.
METHODS
Design
A random assignment, two-group repeated measures experimental design was employed. Qualified, consenting families were sequentially recruited, completed baseline measures and assigned at random to the physical activity and nutrition intervention or the injury prevention control group. An odd digit from a table of random numbers assigned the participant to the control condition; an even digit assigned them to the experimental condition without stratification for gender. Power was calculated based on the total sample, combining both genders. Assuming four-repeated measures by two groups design α=.05, a two-sided test, a moderate effect size of > .25, N’s as small as 32 in each group provided 85% statistical power to detect significant group by time interactions25. Preliminary analyses revealed gender differences in baseline levels of calcium intake, physical activity and bone density. Thus, analyses were run separately by gender.
Sample
Nine cohorts were sequentially recruited over a 3 year period with a class session starting approximately every 3 - 5 months. Baseline measures were conducted between April 2000 and February 2003. Cohorts ranged in size from 9 (our first cohort) to 21 families.
Participants were 10-13 year old children with at least one English or Spanish-speaking parent, living in San Diego County, California. Children were excluded for the following conditions: participation in high-impact or high muscular resistance competitive sports 3 or more times a week for 9 or more months a year, health conditions barring them from physical activity or limiting diet, bone disorders or taking medications known to affect bone metabolism, spending less than four days a week with the guardian willing to attend classes, and children with a body mass index (BMI) greater than 32. Children were not screened for calcium intake. Families were recruited from community events (i.e. neighborhood street fairs, holiday parades), advertisements in local newspapers, fliers posted within the community (i.e. local stores) and from cooperating pediatric agencies. All procedures were approved by the San Diego State University and University of California San Diego Institutional Review Boards.
Intervention
Parent training procedures
Parents received 90 minutes of instruction for each of 8 weeks, independent of their children. A portion of each class focused on osteoporosis, physical activity and diet beneficial for bone health. This component included a mixture of discussion, hands-on activities such as taste tests and exercises that could be done at home without sport’s equipment, and time for questions. Remaining class time (about 60 minutes) was spent training parents in behavior management techniques to be directed toward modifying children’s physical activity and diet, with emphasis on high-impact, high muscular resistance activity, and high calcium food consumption. Parents were taught to use reinforcement (e.g. praise, privileges), shaping, modeling, monitoring, goal setting, and behavior contracting to increase target behavior. These techniques have been successful in previous studies aimed to increase energy intake and activity in children with cystic fibrosis and in trials aimed to decrease children’s exposure to tobacco smoke26-29. Parents were asked to help their children meet a goal of a minimum of 30 minutes of moderate to vigorous physical activity, including high-impact activity, five or more days a week, and a goal of 1300 milligrams of calcium each day. All families received brief coaching calls throughout the eight-week period offering individualized assistance and extra support as needed. Telephone coaching procedures were based on procedures that have been effective in our previous tobacco exposure reduction efficacy trials29,30.
Child training procedures
Children received 90 minutes of instruction once each week for eight weeks with at least 60 minutes spent in supervised physical activity. The training sessions began with a brief discussion of bone health, exercise and exercise safety followed by a warm-up, activity instruction, and participation in individual and cooperative exercises that emphasized bone-loading, including jumping, hopping, skipping, and rebounding from a 4”-8” platform. Fitness games emphasized a variety of motor patterns, quick starts/stops and changes in direction. Exercises were designed to teach children fun activities that could be performed with minimal equipment at home and in the neighborhood, as an individual or in small groups. Some exercises incorporated stability and medicine balls, jump ropes, small hand weights, items found in the home or community such as chairs or curbs. During the last few weeks of the intervention, children were taught exercises on weight machines, modifying the machine and/or exercise as appropriate to accommodate the child’s body size. Resistance exercises included leg presses, seated rows, shoulder presses, and bicep curls and tricep extensions. Participants also learned stretching exercises. The final portion of each session was spent setting individual activity goals with the children, reviewing their goals from the previous week, and discussing the importance of calcium intake, calcium food sources and calcium foods consumed during the previous week. Raffle tickets, praise, encouragement, and differential attention were used to shape and reinforce child behavior.
Evaluation of Intervention Implementation
Attendance was measured at the start of each session. If a family missed a session, both parent and child had the opportunity to make-up the session with a one-to-one session with an instructor. Bilingual, individual sessions were offered in Spanish to parents. A participant was considered to have attended the session if the parent was present during class or made up the session with an instructor. Participants considered to have completed the intervention participated in a minimum of 3 sessions and a maximum of 8 sessions. The mean number of sessions attended was 7 with a standard deviation of 1.15. Almost three-quarters (74.5%) of participants attended 7 or more sessions. The number of sessions attended did not differ by condition, with control group families attending on average 6.8 sessions (+/- 1.08) and experimental group families attending on average 7.1 sessions (+/- 1.19).
Implementation of the intervention was measured by the number of assignments participants completed. Assignments included child and parent monitoring sheets, behavior contracts, and goal sheets that were distributed to families in both the experimental and control conditions. On average, families completed 11 assignments (with a standard deviation of 5.5). Only 4 families did not complete any assignments. Number of assignments significantly correlated with number of sessions attended (r=.473, p<.001). Number of assignments completed was slightly, but not significantly (p=.07) higher among experimental group families (11.8 +/- 5.3) compared to control group families (9.9 +/- 5.6). It is important to note that control families were completing these tasks for injury control outcomes and should have adhered about equally with the experimental families.
Reimbursement and incentives
Parents were provided reimbursement for travel to training and measurement facilities; they and their children were provided meals during the training sessions that illustrated calcium rich foods; parents and children received raffle tickets for class attendance and participation that were entered into a raffle during each session for small prizes; parents and children were provided with cash compensation ($200) for all measures. Attendance and progress toward shaping their children to engage in target behavior resulted in recognition and praise.
Control Group Procedures
Procedures for the injury prevention control group were identical to that of the experimental group with the topical information relating to child safety rather than diet and exercise. For example, parent training included the same behavior management techniques with target behaviors such as bicycle and water safety. Similarly, child sessions focused on injury prevention topics rather than physical activity. Training session frequency and duration, telephone coaching procedures, and reimbursement and incentives were identical, thereby controlling for attention.
Measures
Most measures were completed at baseline, post-test, and at two follow-up assessments. Post-test measures were collected at approximately 3 months after the start of the sessions. The average number of days post test for the physical activity measure was 94.6 days +/- 37 and for the calcium measure was 103.9 +/- 32 days. The first follow-up was approximately 9 months post baseline measure. The average number of days from the baseline measure to the first follow-up measure for physical activity was 271.5 days +/- 28 and for calcium was 283.3 +/- 34. The second follow-up measure was approximately 12 months after the baseline measure. The average number of days from the baseline to the second follow-up measure for physical activity was 367.8 days +/- 39 and for calcium was 380.5 +/- 29. Measures were collected at all points of assessment with the exception of the DXA scan and Tanner staging. The DXA measure occurred at the 9 month measure, on average 247.7 days +/- 43 days after the baseline measure. Tanner staging was only assessed at post-test.
Demographics
Age was reported by the preteen and ethnicity and parent education by the parent. The highest education level reported for either parent was used as an estimate for social class.
Diet
Calcium intake, total energy intake, and other dietary data were measured using three 24-hour dietary recalls, conducted within a two-week period by telephone with trained interviewers using a computer-based prompting system (Minnesota Nutritional Data System (NDS), Nutrition Coordinating Center, University of Minnesota, Minneapolis, MN, Version 4.03, released November 2000). Two of the recalls assessed diet intake for a weekday and the third recall assessed dietary intake for a weekend day. Average daily consumption was averaged across the three recalls. Nutrient calculations were performed using NDS software (Food and Nutrient Database 31, version 4.03). Interviewers queried about dietary supplement use in addition to foods eaten. Both parent and child participated in the dietary recalls, with the parent assisting the child to recall complete diet information and to verify quantities. Participants were given measuring cups, spoons, and food pictures to aid in accurate reporting of quantities of foods consumed. Calcium intake was recorded in milligrams per day to correspond to average daily recommendations. Energy-adjusted calcium intake was calculated by the nutrient density approach (dividing calcium intake by energy consumption). Calcium intake was also dichotomized as 1=met or exceeded the daily recommendation of 1300mg or 0=less.
Physical Activity
Physical activity levels were assessed using one 24-hour physical activity recall of weekday activity conducted with the children by telephone. The recall measure was similar to measures previously validated for children31,32. The recall prompted for participation, frequency, and duration of 28 physical activities plus an open-ended category for other activities occurring before, during and after school. A high-impact physical activity score was computed for total time (frequency X duration) engaged in activities meeting the high-impact criteria. Muscle strengthening/weight lifting exercise was included in the high-impact activity score, as well as gymnastics, basketball, soccer, volleyball, jumping, jogging/running, and karate. High-impact physical activity was calculated in minutes/day. For example, a child who ran for 15 minutes before and after school, played basketball once for 30 minutes after school, and then swam for 20 minutes after school would have had a total of 60 minutes of high impact physical activity (15 × 2 for running, 30 × 1 for playing basketball, and 0 minutes for swimming). Extreme values were recoded to two standard deviations from the mean. The reported relationship between weekday total time of high-impact physical activity correlated with total body BMD (r=.207, p=.03) and lumbar spine BMD (r=.201, p=.03) from the participant’s DXA scan, suggesting predictive validity. Physical activity was also dichotomized as 1=met the daily recommendation of at least 10 minutes of high-impact physical activity and 0=less21,22,33.
DXA-based BMD and Body Composition
Bone mineral density (BMD), bone mineral content (BMC) and body composition were measured using DXA (DPX-NT, GE/Lunar Corporation, Madison, WI, Software version 6.80) at our research facility. High-resolution regional scans of the total body, lumbar spine (frontal projection) and proximal femur were conducted. Pediatric software algorithms provided by the manufacturer were used for all DXA scans. Precision (% coefficient of variation) for our laboratory was 1.23% for spine (L1-L4), 0.6% for total hip, and 0.99% for total body BMD. This paper analyzed BMD (g/cm2) and BMC (g). Only BMD is reported in the tables. Bone measures were conducted at baseline and 9 months for the lumbar spine (L1-L4), femoral neck, trochanter, total hip and total body and their percent change BMD (((9 month value – baseline value)/baseline value)*100). Lean tissue mass was measured by DXA. A DXA scan was not conducted at 9 months for our first cohort. Therefore, seven participants do not have 9 month bone density values. This subset was retained in our sample because they did complete 9 month calcium and physical activity measures.
Other Measures
Height and weight (with shoes removed) were measured by technicians during fitness testing. Pubertal status of participants was assessed using self-reported Tanner Stages34,35, with boys rating their development of pubic hair and girls rating their development of pubic hair and breasts. As reported in a prior publication, pre-adolescents accurately reported their pubertal stage35. Puberty status was assessed during the post-test measures.
Covariates theoretically expected to determine bone development – age, height, lean tissue mass, and pubertal development– needed to be included in the GEE models in order to differentiate between normal bone development due to maturation and bone development due to the intervention. However, the sample size limited the number of variables that could be included in the model. To conserve power sufficient to test group by time intervention effects, a single growth composite scale was formed. Baseline age, height, lean tissue and pubertal development were converted to a common metric stratified by gender using SPSS. The growth composite score was formed by computing the mean of standardized items allowing up to 1 score to be missing (Cronbach’s α=.85 for boys and α=.84 for girls).
Analysis
Statistical analyses were performed using SPSS versions 6.1.3, 10.1 and SAS v.9.1. Graphics were generated from Stata v. 10. Double entry and logic checks were implemented to ensure data accuracy. Transformations were computed for calcium intake, high-impact physical activity minutes, and BMD to constrain skewness. Geometric means and anti-log interquartile ranges are reported in tables36.
Group by time effects for the intervention were analyzed longitudinally using GEE; with linear components of time as “within subjects” factors and a group by time interaction as a “between subjects” factor34. The number of days post-baseline served as the time variable for GEE equations. The time interaction term was formed by multiplying the group variable (control =0, experimental =1) by the time variable (number of days post the baseline measure). BMD and BMC were regressed on predictors using a Gaussian link function and an exchangeable correlation structure. Modeling procedures based on GEE are superior to models based on analysis of variance since they do not require repeated measures to be equally spaced and they retain cases with missing data30. ANOVAs compared group means cross-sectionally at each point of assessment for calcium intake, high-impact physical activity, BMD and BMC, and BMD and BMC percent change. Pearson Chi-square analyses tested group differences. Gender comparisons were conducted across all analyses.
RESULTS
Sample Demographics
Sequential recruitment from 2000 to 2003 resulted in 138 families volunteering and 117 completing baseline and follow up measures for inclusion in outcome analyses. Figure 1 displays the number of participants who were eligible, randomized, completed the study, and reasons for exclusion and non-completion.
Figure 1. Flow diagram of participants through trial.

The sample was comprised of 58.1% girls with a mean age of 11.48 years (SD=0.96). The ethnic distribution was 42.7% Hispanic, 40.2% White not Hispanic, 9.4% African American and 7.7% other. Ninety-seven percent of participants had at least one parent graduate from high school and 37.2% had at least one parent graduate from a 4-year university.
Demographic and outcome variables at baseline were tested for significant differences between control and experimental conditions, using t-tests or chi square, depending on the variable metric. Only gender reached significance, suggesting that random assignment resulted in balanced groups for all other factors. Boys and girls differed on Tanner stage with girls reporting significantly higher pubertal stage than boys (2.9 and 2.2, respectively, p>.001). Boys and girls were significantly different at baseline for BMD, calcium intake and fitness level; therefore all analyses were conducted separately by gender.
Participants who dropped out of the study were compared to those who completed the study. Only age was significantly different, with participants who dropped out being younger than those who completed the study (10.73 years (SD=0.84) versus 11.42 years (SD=0.97)) and this effect was controlled for in multivariate bone analyses.
For each outcome variable we have presented tests of the significance of cross-sectional differences between groups. These analyses are followed by a summary of the test of significance of the difference in change over time for the same variables. Following these analyses we present the statistically significant differences between groups for those who met a recommended criterion for health.
Calcium Intake
Cross sectional differences
Table 1 reports geometric means and inter-quartile ranges for calcium intake at each point of assessment. Boys in the experimental group had significantly higher calcium intake than the control group at 3 months and 9 months. The difference was no longer significant at the 12 month assessment but the experimental group’s mean calcium intake remained higher than the controls. Similar patterns were observed for energy-adjusted calcium intake with significant differences again at 3 months but not at 9 or 12 months. Among girls, the experimental group had higher calcium intake but not statistically different than controls at 3, 9 and 12 months. For energy adjusted calcium, girls in the experimental condition were higher than controls at 3, 9, and 12 months but not significantly. Both boys and girls in the experimental group experienced an approximate 25% increase in calcium consumption from baseline to post-test, although the girls did not attain the same mean level of intake as boys.
Table 1.
Cross-sectional Analyses of Calcium Intake & Minutes of High-Impact Physical Activity (Geometric Means & Inter-Quartile Range at Baseline, 3, 9 and 12 Months
| All Participants | ||||||||
|---|---|---|---|---|---|---|---|---|
| Baseline | 3 Months | 9 Months | 12 Months | |||||
| Control | Exp | Control | Exp | Control | Exp | Control | Exp | |
| Calcium (mg/day) | 1066 (522) | 934 (502)* | 988 (693) | 1182 (691)** | 949 (500) | 1139 (773)** | 962 (609) | 1067 (577) |
| Calcium (mg/1000 kcal) | 539 (217) | 489 (289) | 542 (286) | 623 (289)** | 516 (231) | 563 (336) | 523 (270) | 545 (282) |
| Weekday High Impact PA (mins/day) | 29.2 (70) | 30.3 (39) | 15.8 (44) | 27.2 (50)* | 11.1 (30) | 18.2 (45)* | 12.0 (32) | 17.4 (50) |
| Calcium sample sizes range from 44-49 for Control Group and 62-67 for Experimental Group | ||||||||
| Physical Activity sizes ranges from 43-48 for Control Group and 62-66 for Experimental Group | ||||||||
| BOYS | ||||||||
| Baseline | 3 Months | 9 Months | 12 Months | |||||
| Control | Exp | Control | Exp | Control | Exp | Control | Exp | |
| Calcium (mg/day) | 1092 (513) | 1058 (449) | 1052 (592) | 1352 (541)** | 970 (533) | 1298 (708)** | 1045 (681) | 1172 (627) |
| Calcium (mg/1000 kcal) | 537 (255) | 505 (259) | 531 (285) | 641 (282)** | 514 (254) | 611 (279)* | 539 (328) | 569 (256) |
| Weekday High Impact PA (mins/day) | 35.8 (65) | 32.5 (39) | 13.2 (55) | 26.3 (38) | 14.8 (34) | 22.8 (66) | 19.1 (32) | 19.6 (55) |
| Calcium sample sizes range from 23-24 for Control Group and 22-24 for Experimental Group | ||||||||
| Physical Activity sizes ranges from 20-24 for Control Group and 22-25 for Experimental Group | ||||||||
| GIRLS | ||||||||
| Baseline | 3 Months | 9 Months | 12 Months | |||||
| Control | Exp | Control | Exp | Control | Exp | Control | Exp | |
| Calcium (mg/day) | 1039 (565) | 869 (489)* | 933 (618) | 1097 (600) | 928 (536) | 1061 (829) | 871 (550) | 1013 (585) |
| Calcium (mg/1000 kcal) | 542 (214) | 479 (213) | 553 (267) | 614 (284) | 518 (205) | 538 (348) | 504 (177) | 533 (304) |
| Weekday High Impact PA (mins/day) | 23.0 (61) | 29.1 (35) | 18.6 (39) | 27.6 (52) | 7.9 (29) | 15.9 (42) | 5.9 (32) | 16.1 (44)* |
| Calcium sample sizes range from 20-25 for Control Group and 40-43 for Experimental Group | ||||||||
| Physical Activity sizes ranges from 22-24 for Control Group and 39-41 for Experimental Group | ||||||||
Statistical tests used one-way ANOVA using log or square root transformed means.
p≤.10;
p≤.05 reflect difference in experimental group from control.
Differential change over time
Figure 2 plots the best fit line for each condition by gender. Each individual’s log transformed calcium value was plotted across all points of assessment. We present the best fit line of the individual points as determined by the Stata graphics (lfit) procedure. Longitudinal GEE results are explained below. For calcium intake, a significant group by time interaction was observed from pre to post test (0 to 3 months) for the full sample (p=.008) and for girls (p=.006), but not for boys. For energy-adjusted calcium, significant group by time effects were observed pre to post test for the full sample (p=.006) and for girls (p=.008), but not for boys. From post-test to follow-up (3 to 12 months), a group by time interaction for calcium and energy-adjusted calcium intake was no longer significant for the full sample or for boys and girls separately. However, the change in calcium intake across the length of study (0 to 12 months) produced a significant group by time effect for the full sample (p=.023) and a significant effect for girls (p=.019), but not for boys. Change in energy-adjusted calcium was not significant across the length of the study for the full sample, for girls or boys.
Figure 2. Log of Calcium Intake by Group and Gender.

For graphical purposes, extreme values for the number of days between baseline and the final follow-up were recoded to two standard deviations from the mean number of days for the group. The original number of days was retained in the longitudinal GEE analyses.
Meeting Calcium Recommendation
Further cross-sectional analyses were conducted with the percentages of boys and girls within each condition who met the recommended 1300 mg/day calcium intake (Refer to Table 2). The proportion of boys in the experimental group who met the daily calcium recommendation was significantly higher than controls at 9 months (p<.001). The pattern observed among boys in the experimental group reflected a higher percentage meeting the calcium recommendation at 3 and 9 months with a slightly lower level at 12 months, but still above the baseline level. In comparison, the pattern observed among control boys reflected a lower percentage meeting the calcium recommendation at 9 months and then a return to baseline levels at 12 months. The percentage of experimental girls achieving the recommended levels of intake was higher than controls at 3, 9 and 12 months, but there were no significant cross-sectional differences. For control girls, a decline in percentages who met the calcium recommendation across the entire length of the study was observed. Both genders in the experimental group had a higher proportion meeting the recommendation at every point of assessment post-test than their control counterparts. The patterns observed with the percent meeting the recommendation parallel the trends observed in the reported group means in Table 1.
Table 2.
Percentages Meeting Daily Calcium & Physical Activity Recommendations
| Baseline | 3 Mos | 9 Mos | 12 Mos | |||
|---|---|---|---|---|---|---|
| 1300 mg/day Calcium | BOYS | Control (n = 23-24) | 33% | 35% | 13% | 33% |
| Experimental (n = 22-24) | 25% | 58% | 65%** | 41% | ||
|
|
||||||
| GIRLS | Control (n = 20-25) | 33% | 24% | 24% | 15% | |
| Experimental (n = 40-43) | 15% | 37% | 43% | 30% | ||
|
| ||||||
| 10 min/day high-impact physical activity | BOYS | Control (n = 23-24) | 83% | 52% | 63% | 75% |
| Experimental (n = 21-24) | 92% | 81%** | 68% | 63% | ||
|
|
||||||
| GIRLS | Control (n = 21-24) | 61% | 61% | 70% | 43% | |
| Experimental (n = 40-43) | 79% | 79% | 76% | 53% | ||
Significant group differences p<.05.
Weekday High-Impact Physical Activity
Cross sectional differences
Table 1 reports geometric means and inter-quartile ranges for total minutes per weekday of high-impact physical activity at each point of assessment. Average minutes of high-impact physical activity were lower at post-test for both genders in experimental and control groups. Among boys, high-impact physical activity minutes were not significantly different between group conditions at any assessment point, although experimental boys were higher at each post-baseline assessment. Experimental girls’ average minutes of high-impact physical activity was approximately double the average of the control group at 9 and 12 months, but only marginally significant cross-sectional differences were observed at 12 months.
Differential change over time
There were no group by time effects for high-impact physical activity across the length of the study, pre-test to post-test or post-test to follow-up for the full sample or either gender separately. Figure 3 presents the best fit line for the log transformed amount of high impact weekday physical activity across all points of assessment. Both genders in both conditions declined across time.
Figure 3. High-Impact Physical Activity by Group and Gender.
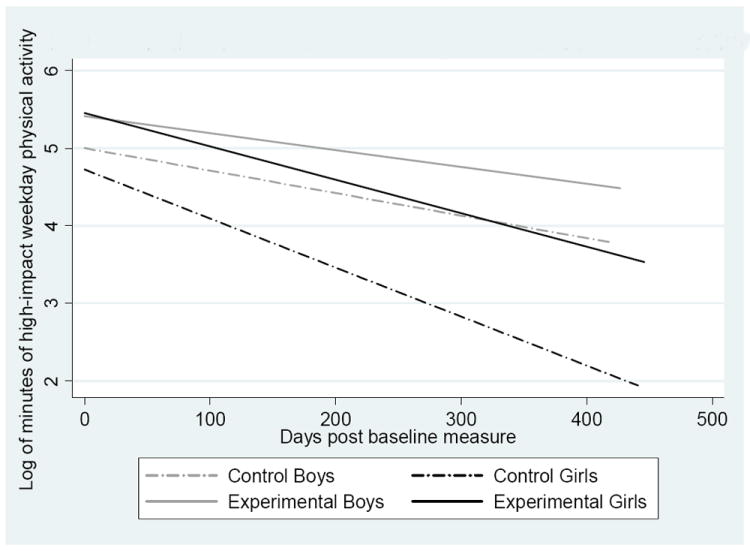
For graphical purposes, extreme values for the number of days between baseline and the final follow-up were recoded to two standard deviations from the mean number of days for the group. The original number of days was retained in the longitudinal GEE analyses.
Meeting High-Impact Physical Activity Recommendation
The percentages of boys and girls in each condition meeting at least 10 minutes per day of high-impact physical activity was examined (Refer to Table 2). This level, when averaged over a week, has been found beneficial as measured by bone mass21,22,33. A significantly higher percentage of experimental boys met the recommendation at 3 months compared to control boys. Among experimental boys, fewer met the recommendation at 9 and 12 months compared to 3 months. A lower percentage of control boys met the recommendation than experimental boys at all points of assessment except at 12 months where a higher percentage of control boys met the recommendation compared to experimental boys. Among girls, the experimental group reported higher percentages of meeting the high-impact physical activity recommendation at each post-baseline assessment, although not significantly.
Bone Measurements
Cross sectional differences
BMD at baseline and 9 months are presented in Table 3 without applying controls for skeletal growth. BMC results are not shown in tabular form but results from their analyses are discussed below. There were no group differences on mean values of BMD or BMC at 9 months.
Table 3.
Cross-sectional Analyses of Bone mineral density (BMD) at baseline and 9 months. Geometric Means (Inter-quartile Ranges), Mean Percent Changes (Standard Deviations), and Proportional Differential Change
| ALL PARTICIPANTS | |||||||
|---|---|---|---|---|---|---|---|
| Baseline | 9 Months | Mean % Change by Group | Proportion of Differential Change | ||||
| BMD (g/cm2) | Control | Exp | Control | Exp | Control | Exp | ((Exp – Control)/Control)*100 |
| L1-L4 | 0.816 (0.193) | 0.818 (0.156) | 0.858 (0.215) | 0.874 (0.232) | 6.3 (5.0) | 6.6 (5.2) | 4.7% |
| Total hip | 0.904 (0.186) | 0.916 (0.162) | 0.930 (0.153) | 0.952 (0.182) | 3.8 (4.7) | 4.6 (4.2) | 21.1% |
| Femoral neck | 0.897 (0.155) | 0.908 (0.190) | 0.931 (0.158) | 0.950 (0.222) | 4.5 (4.8) | 5.1 (4.9) | 13.3% |
| Trochanter | 0.769 (0.153) | 0.767 (0.135) | 0.785 (0.157) | 0.799 (0.205) | 3.2 (5.7) | 4.5 (5.2) | 40.6% |
| Total Body | 0.975 (0.109) | 0.989 (0.111) | 0.998 (0.123) | 1.017 (0.119) | 2.9 (2.9) | 3.0 (2.6) | 3.4% |
| Sample sizes ranged from 46-49 for the Control Group and 63-68 for the Experimental Group | |||||||
| BOYS | |||||||
| Control | Exp | Control | Exp | Control | Exp | ((Exp – Control)/Control)*100 | |
| L1-L4 | 0.763 (0.128) | 0.767 (0.100) | 0.797 (0.160) | 0.803 (0.103) | 4.5 (4.7) | 5.0 (3.8) | 11.1% |
| Total hip | 0.906 (0.187) | 0.894 (0.101) | 0.926 (0.155) | 0.932 (0.111) | 2.2 (3.5) | 4.1 (2.7)* | 86.4% |
| Femoral neck | 0.899 (0.154) | 0.883 (0.100) | 0.921 (0.163) | 0.928 (0.115) | 2.4 (4.0) | 5.0 (4.4)** | 108.3% |
| Trochanter | 0.771 (0.158) | 0.753 (0.081) | 0.786 (0.158) | 0.781 (0.120) | 2.0 (4.6) | 3.6 (3.6) | 80.0% |
| Total Body | 0.960 (0.090) | 0.974 (0.072) | 0.976 (0.105) | 0.994 (0.089) | 1.7 (2.7) | 2.3 (1.9) | 35.3% |
| Sample sizes ranged from 24 for the Control Group and 23-25 for the Experimental Group | |||||||
| GIRLS | |||||||
| Control | Exp | Control | Exp | Control | Exp | ((Exp – Control)/Control)*100 | |
| L1-L4 | 0.871 (0.180) | 0.851 (0.213) | 0.930 (0.191) | 0.919 (0.257) | 8.3 (4.6) | 7.6 (5.7) | -8.4% |
| Total hip | 0.903 (0.187) | 0.929 (0.214) | 0.934 (0.153) | 0.964 (0.262) | 5.5 (5.2) | 5.0 (4.9) | -9.1% |
| Femoral neck | 0.894 (0.157) | 0.924 (0.265) | 0.942 (0.185) | 0.964 (0.282) | 6.7 (4.7) | 5.1 (5.2) | -23.9% |
| Trochanter | 0.768 (0.155) | 0.775 (0.196) | 0.784 (0.157) | 0.809 (0.221) | 4.6 (6.5) | 5.0 (5.9) | 8.7% |
| Total Body | 0.990 (0.156) | 0.997 (0.144) | 1.022 (0.134) | 1.031 (0.166) | 4.3 (2.6) | 3.5 (2.8) | -18.6% |
| Sample sizes ranged from 22-25 for the Control Group and 39-43 for the Experimental Group | |||||||
p≤.10;
p≤.05 reflect difference in experimental group from control.
Differential change over time
Two different analyses were conducted to assess bone change. The first analyses was to create a percent change in bone between the 9 month and baseline measure (((9 month value – baseline value)/baseline value)*100). The BMD percent change values for each bone site are presented in Table 3 without applying controls for skeletal growth. BMC percent change variables are not presented in the table but are described below. Group differences were tested on percent change using ANOVAS. Experimental boys accrued 4.1% in total hip BMD compared to 2.2% for controls (p=.053) as well as a 5.0% accrual in femoral neck BMD compared to 2.4% for controls (p=.041). Higher spine, trochanter and total body percent changes were observed for experimental boys but these changes did not reach significance. Girls’ BMD accrued at a higher rate than boys. However, there were no significant differences in the percentage increase between experimental girls and controls at any bone site. Percent changes of BMC were analyzed without applying controls for skeletal growth. Experimental boys accrued higher rates of BMC at all bone sites compared to control boys, but only marginally statistically higher at the total hip (12.0% vs. 9.0%, p=.09) and total body (11.3% vs. 9.3%, p=.07) regions. Among girls, there were no significant differences in BMC by experimental condition. However, control girls showed a near significant increase in spine BMC accrual (13.4% vs. 18.2%, p=.08) compared to experimental girls.
The second analyses assessed repeated measures of bone using GEE and adjusting for the growth composite score. There were no significant group by time differences for the full sample. Among boys, group by time differences reached significance for total hip BMD (p=.045), and femoral neck BMD (p=.033). Experimental boys showed a higher rate of bone accrual at the hip and femoral neck regions compared to control boys even after adjusting for skeletal growth. Similar differential increases were observed among boys for BMC at the hip (p=.068) and total body (p=.054) regions. No significant group by time interaction effects were observed for girls at any bone site for BMD. For BMC, control girls showed an increase in spine BMC (p=.030) compared to experimental girls. No other significant group by time interaction effects were observed for girls for BMC.
DISCUSSION
As noted earlier, more than 50% of women and 30% of men will experience an osteoporotic fracture in their lifetime. Since bone growth and integrity are determined during growth periods in childhood and adolescence, it is imperative that efficacious interventions during childhood be identified in order to reduce or delay the incidence of osteoporosis and consequential fractures for women and men. Increasing BMD and BMC during adolescence might achieve these goals.
Our parent and child training was based on learning theory, studies designed to train parents in child management, and studies that demonstrate children’s ability to modify food choices and activity26-29. We hypothesized that family training was sufficient to increase calcium intake to the target of 1300mg/day, and moderate to vigorous physical activity to 30 minutes per day, including at least 10 minutes of high-impact activity, for at least five days per week. Our outcome results, while promising, did not reach these levels.
For change in calcium intake, we achieved increases in both boys and girls, but only experimental boys reached the goal of 1300mg/day. Differential change in calcium intake over time showed that the experimental group increased calcium intake pre to post-test significantly more than did controls. This approached significance for boys and reached significance for girls, even though the average for girls did not reach the 1300mg/day goal. The significance of differences in girls was most likely attributed to the decline in the control group pre to post test with an increase in the experimental group. However, consistent with behavioral theory, group by time interactions were no longer significant for the whole sample or for boys and girls separately over the follow up period. This suggests that the increase in calcium intake was not sustained in absence of the intervention procedures. Since theory asserts that behavior should be reinforced at least intermittently to be sustained, this finding suggests that our training did not sustain parent child management procedures enough to sustain increased calcium intake among their children. An alternative explanation for our findings on calcium intake is that the recognized imprecision of dietary assessment constrained our ability to obtain accurate estimates of calcium intake in the study sample. The interpretation of self-reported data on dietary intakes collected using available methodologies (including dietary records, recalls, and food frequency questionnaires) is constrained by several well-described limitations37,38.
For changes in physical activity, average weekday minutes of high-impact physical activity decreased over time for both genders in both experimental groups, which is typical as children progress through adolescence39-41. Boys maintained a higher level of physical activity compared to girls. Control girls reported the lowest levels of physical activity of any group. These findings suggest that the intervention may have slowed the rate of decline in high-impact physical activity for both boys and girls. While such a “trend” is promising, it falls far short of our goals for increasing high-impact physical activity.
Our primary outcome measure was change in BMD. No significant group by time interactions were observed for the full sample. However, for boys, longitudinal group by time differences remained for BMD total hip and femoral neck as well as total hip and total body BMC after controlling for skeletal growth. The only significant difference among girls was an increase in spine BMC and a marginal significant difference in spine BMD observed for controls compared to experimental girls. Our interpretation of these bone changes is that for girls, failure to reach the goal for calcium intake and/or failure to sustain let alone increase high-impact physical activity precluded differential increase in bone relative to controls, even though both groups were growing and obtained increases in bone density. For boys, however, we achieved a significant differential increase in calcium intake that reached the goal of 1300 mg/day among those in the experimental condition. While boys did not obtain a significant increase in high-impact physical activity, experimental boys decreased more slowly than did male controls or girls. The combination of both sufficient calcium intake and sufficient physical activity, at least during the nine months of follow up, appears to have been sufficient to obtain a differential increase in BMD and BMC among boys, even after control for skeletal growth.
To test a procedure that might enable parents to promote relatively intense physical activity and calcium rich diets in their children, we adopted a brief parent training model. Our results suggest that this did not result in sufficiently intense physical activity for boys and girls or calcium consumption among girls. Relying solely on clinical or public school programs to achieve these goals does not now appear affordable, making family interventions all the more important for prevention of osteoporosis. A program that can equip parents to promote diet and activity in their children remains to be developed and validated.
While most parents in both experimental and control conditions acquired knowledge of child management practices, anecdotal information suggested that many were not motivated to encourage their children to engage in more or more vigorous recreational physical activity. Future studies should direct more attention to increasing motivation of parents to provide incentives to increase the frequency, duration, and intensity of physical activity, even if this compromises other responsibilities (e.g. household chores) assigned to adolescents. This might be achieved by teaching parents to discriminate the intensity, duration and frequency of bone-building physical activity from less intense and casual recreational activity. This might also require linking physical activity, in addition to household chores, to contingent privileges.
Although a specific exercise prescription for maximizing bone mineralization in children is not yet known, recent studies indicated that 15-20 minutes of high-impact activity, e.g., jumping, for 2-3 d/wk induced significant differential changes between control and intervention groups21,22,33. Thus, our overall results suggest that the “dose” of our physical activity intervention needs to be substantially higher in both boys and girls. Our data also suggest, for girls, that a more intensive intervention is needed to increase calcium intake.
Our results are encouraging in the face of recent research that has not demonstrated reliable increases in BMC for preteen girls involved in a lifestyle educational program42. Other research, however, has demonstrated BMD and BMC increases in the context of structured, school-based programs of vigorous exercise for children and for structured trials conducted within HMOs21,22,43. A study conducted among teen girls showed significant increases in calcium and vitamin D intake but no differences in physical activity. This trial produced significant increases in BMD after one year and maintained these differences for an additional year43. Future research should be directed to means of increasing the intensity of interventions for both diet and physical activity changes and maintenance among both girls and boys not involved in competitive athletic programs.
Recent research directions following ecological models suggest that “more intensive interventions” might involve both societal changes in built environments (such as development of walkable neighborhoods44-48) and policies that encourage calcium fortification of a wide variety of foods (e.g. orange juice, cereal, bread). This might set in motion greater physical activity in general, but it may not be sufficiently high-impact to affect change in bone mass or strength. However, even an increase in general activity might combine with more intensive educational or clinical interventions to affect bone health.
To our knowledge, no study has demonstrated that increased calcium fortification of foods results in an overall increase in calcium intake. Such policies, as for the walkable neighborhoods, might serve as motivating variables that increase the efficacy of educational or clinical interventions to increase calcium intake and high-impact physical activity to high enough intensity to effect bone growth during critical periods of development. Policies that increase opportunity for calcium consumption as well as promoting general physical activity (if not vigorous) also might serve as mediating variables for maintenance of lifestyle changes achieved by formal educational or clinical interventions. Thus, research concerning both community-wide and intensive clinical interventions seems warranted to test possible osteoporosis prevention and to reverse alarming trends in preteen and adolescent diet and physical activity patterns.
Future research should be directed to development of more intensive educational or clinical interventions for increasing calcium intake and for increasing high-impact physical activity and to assess their affects on bone health in the context of increased calcium fortification of foods (or other policies affecting diet) and community-wide ecological supports (e.g. city planning) for general activity, if not also for high-impact physical activity. This will require contrasting ecological conditions within which more intensive educational/clinical interventions are tested experimentally.
SO WHAT?
This is the first randomized, controlled trial that has taught parents of preteens to use child management procedures to encourage their preteen children to consume high calcium diets and engage in bone-loading physical activity, that combined promote bone growth. Increases in calcium consumption and increases in bone density among boys suggests that a more intensive intervention might yield sufficient change in diet and physical activity to contribute to the prevention of osteoporosis in later life. If our results hold true, health promotion researchers should provide a more intensive skills training procedures for more than 8 weeks in order to reliably increase calcium consumption and bone-promoting physical activity in both male and female preteens.
Acknowledgments
FUNDING
This study was supported by a grant from DHHS/NIH/NICHHD # RO1 HD37749, awarded to Dr. Mel Hovell and the San Diego State University Research Foundation and by intramural support from CBEACH. This study serves to commemorate Dr. David Sartoris, Radiologist, who died in year 2 of this study. This study could not have been initiated without his incredible energy and expertise.
References
- 1.Center J, Eisman J. The epidemiology of pathogenesis of osteoporosis. Bailliere’s Clin Endocrinol Metab. 1997;11(1):23–62. doi: 10.1016/s0950-351x(97)80489-2. [DOI] [PubMed] [Google Scholar]
- 2.Orwoll ES, Klein RF. Osteoporosis in Men. Epidemiology, pathophysiology and clinical characterization. In: Marcus R, Feldman D, Kelsey J, editors. Osteoporosis. 3. San Diego: Academic Press; 1996. pp. 745–784. [Google Scholar]
- 3.US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. Rockville, MD: US Department of Health and Human Services, Office of the Surgeon General; 2004. [Google Scholar]
- 4.Bachrach LK. Acquisition of optimal bone mass in childhood and adolescence. TRENDS in. Endocrinol Metab. 2001;12(1):22–28. doi: 10.1016/s1043-2760(00)00336-2. [DOI] [PubMed] [Google Scholar]
- 5.Bailey D. The Saskatchewan bone mineral accrual study: Bone mineral acquisition during the growing years. Int J Sports Med. 1997;18(Suppl 3):S191–194. doi: 10.1055/s-2007-972713. [DOI] [PubMed] [Google Scholar]
- 6.Iuliano-Burns S, Saxon L, Naughton G, Gibbons K, Bass SL. Regional specificity of exercise and calcium during skeletal growth in girls: a randomized controlled trial. J Bone Miner Res. 2003;18:156–162. doi: 10.1359/jbmr.2003.18.1.156. [DOI] [PubMed] [Google Scholar]
- 7.Johnston CC, Miller JZ, Slemenda CW, et al. Calcium supplementation and increases in bone mineral density in children. N Engl J Med. 1992;327:82–87. doi: 10.1056/NEJM199207093270204. [DOI] [PubMed] [Google Scholar]
- 8.Lloyd T, Andon MB, Rollings N, et al. Calcium supplementation and bone mineral density in adolescent girls. JAMA. 1993;270:841–844. [PubMed] [Google Scholar]
- 9.Lee WT, Leung SS, Wang SH, et al. Double-blind, controlled calcium supplementation and bone mineral accretion in children accustomed to a low-calcium diet. Am J Clin Nutr. 1994;60:744–750. doi: 10.1093/ajcn/60.5.744. [DOI] [PubMed] [Google Scholar]
- 10.Nowson CA, Green RM, Hopper JL, et al. A co-twin study of the effect of calcium supplementation on bone density during adolescence. Osteoporos Int. 1997;7:219–225. doi: 10.1007/BF01622292. [DOI] [PubMed] [Google Scholar]
- 11.Lloyd T, Martel J, Rollings N, et al. The effect of calcium supplementation and Tanner stage on bone density, content and area in teenage women. Osteoporos Int. 1996;6:276–283. doi: 10.1007/BF01623385. [DOI] [PubMed] [Google Scholar]
- 12.Fehily AM, Coles RJ, Evans WD, Elwood PC. Factors affecting bone density in young adults. Am J Clin Nutr. 1992;56:579–586. doi: 10.1093/ajcn/56.3.579. [DOI] [PubMed] [Google Scholar]
- 13.Lee WT, Leung SS, Leung DM, Cheng JC. A follow-up study on the effects of calcium-supplement withdrawal and puberty on bone acquisition of children. Am J Clin Nutr. 1996;64:71–77. doi: 10.1093/ajcn/64.1.71. [DOI] [PubMed] [Google Scholar]
- 14.Slemenda CW, Peacock M, Hui S, Zhou L, Johnston CC. Reduced rates of skeletal remodeling are associated with increased bone mineral density during the development of peak skeletal mass. J Bone Miner Res. 1997;12:676–683. doi: 10.1359/jbmr.1997.12.4.676. [DOI] [PubMed] [Google Scholar]
- 15.Bonjour JP, Chevalley T, Ammann P, Slosman D, Rizzoli R. Gain in bone mineral mass in prepubertal girls 3.5 years after discontinuation of calcium supplementation: a follow-up study. Lancet. 2001;358:1208–1212. doi: 10.1016/S0140-6736(01)06342-5. [DOI] [PubMed] [Google Scholar]
- 16.Janz K, Burns T, Levy S, et al. Everyday activity predicts bone geometry in children: The Iowa bone development study. Med Sci Sports Exerc. 2004;36(7):1124–1131. doi: 10.1249/01.mss.0000132275.65378.9d. [DOI] [PubMed] [Google Scholar]
- 17.Bailey DA, Martin Ad, McKay HA, Minwald RL, Crocker PR, Faulkner RA. Calcium accretion in girls and boys during puberty: A longitudinal analysis. J Bone Mineral Res. 2000;15:2245–2250. doi: 10.1359/jbmr.2000.15.11.2245. [DOI] [PubMed] [Google Scholar]
- 18.Dent CE. Problems in metabolic bone disease. In: Frame B, Parfitt AM, Duncan H, editors. Clinical Aspects of Metabolic Bone Disease. Amsterdam: Excerpta Medica; 1973. pp. 1–7. [Google Scholar]
- 19.Bass S, Pearce G, Bradney M, et al. Exercise before puberty may confer residual benefits in bone density in adulthood: studies in active prepubertal and retired female gymnasts. J Bone Min Res. 1998;13(3):500–507. doi: 10.1359/jbmr.1998.13.3.500. [DOI] [PubMed] [Google Scholar]
- 20.Morris FL, Naughton GA, Gibbs JL. Prospective 10-month exercise intervention in premenarcheal girls: Positive effects on bone and lean mass. J Bone Mineral Res. 1997;12:1453–1462. doi: 10.1359/jbmr.1997.12.9.1453. [DOI] [PubMed] [Google Scholar]
- 21.McKay HA, Petit MA, Schutz RW, Prior JC, Barr SI, Khan KM. Augmented trochanteric bone mineral density after modified physical education classes: a randomized school-based exercise intervention study in prepubescent and early pubescent children. J Pediatr. 2000;136:156–162. doi: 10.1016/s0022-3476(00)70095-3. [DOI] [PubMed] [Google Scholar]
- 22.Fuchs RK, Bauer JJ, Snow CM. Jumping improves hip and lumbar spine bone mass in prepubescent children: a randomized controlled trial. J Bone Miner Res. 2001;16(1):148–156. doi: 10.1359/jbmr.2001.16.1.148. [DOI] [PubMed] [Google Scholar]
- 23.Witzke KA, Snow CM. Effects of plyometric jump training on bone mass in adolescent girls. Med Sci Sports Exerc. 2000;32(6):1051–1057. doi: 10.1097/00005768-200006000-00003. [DOI] [PubMed] [Google Scholar]
- 24.Heinonen A, Sievanen H, Kannus P, et al. High-impact exercise and bones of growing girls: A 9-month controlled trial. Osteoporos Int. 2000;11(12):1010–1017. doi: 10.1007/s001980070021. [DOI] [PubMed] [Google Scholar]
- 25.Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2. Hillsdale, NJ: Lawrence Erlbaum Associates; 1988. [Google Scholar]
- 26.Stark LJ, Knapp LG, Bowen AM, et al. Increasing calorie consumption in children with Cystic Fibrosis: replication with 2-year follow-up. J Applied Behav Analysis. 1993;26:435–450. doi: 10.1901/jaba.1993.26-435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Stark LJ, Bowen AM, Tyc VL, Evans S, Passero MA. A behavioral approach to increasing calorie consumption in children with Cystic Fibrosis. Pediatric Psychology. 1990;15(3):309–326. doi: 10.1093/jpepsy/15.3.309. [DOI] [PubMed] [Google Scholar]
- 28.Stark LJ, Mulvihill MM, Powers SW, et al. Behavioral intervention to improve calorie intake of children with Cystic Fibrosis: treatment versus wait list control. Pediatric Gastroenterology & Nutrition. 1996;22(3):240–253. doi: 10.1097/00005176-199604000-00005. [DOI] [PubMed] [Google Scholar]
- 29.Wahlgren DR, Hovell MF, Meltzer SB, Hofstetter CR, Zakarian JM. Reduction of environment tobacco smoke exposure in asthmatic children: a two-year follow-up. Chest. 1997;111(1):81–88. doi: 10.1378/chest.111.1.81. [DOI] [PubMed] [Google Scholar]
- 30.Hovell MF, Zakarian JM, Matt GE, Hofstetter CR, Bernert JT, Pirkle J. Effect of counseling mothers on their children’s exposure to environmental tobacco smoke: randomised controlled trial. BMJ. 2000;321:337–342. doi: 10.1136/bmj.321.7257.337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Sallis J, Strikmiller P, Harsha D, et al. Validation of interviewer- and self-administered physical activity checklists for fifth grade students. Med Sci Sports Exerc. 1996;28(7):840–851. doi: 10.1097/00005768-199607000-00011. [DOI] [PubMed] [Google Scholar]
- 32.Sallis J, Buono M, Roby J, Micale F, Nelson J. Seven-day recall and other physical activity self-reports in children and adolescents. Med Sci Sports Exerc. 1993;25(1):99–108. doi: 10.1249/00005768-199301000-00014. [DOI] [PubMed] [Google Scholar]
- 33.MacKelvie KJ, Khan KM, Petit MA, Janssen PA, McKay HA. A school-based exercise intervention elicits substantial bone health benefits: A 2-year randomized controlled trial in girls. Pediatrics. 2003;112(6):e447–e452. doi: 10.1542/peds.112.6.e447. [DOI] [PubMed] [Google Scholar]
- 34.Tanner JM. Growth at adolescence. Springfield, IL: Thomas; 1962. [Google Scholar]
- 35.Schmitz KE, Hovell MF, Nichols JF, et al. Validation study of adolescents’ puberty self-assessments. Journal of Early Adolescence. 2004;24(4):357–384. [Google Scholar]
- 36.Bland JM, Altman DG. Transformations, means, and confidence intervals. BMJ. 1999;312:1079. doi: 10.1136/bmj.312.7038.1079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Black AE, Cole TJ. Biased over- or under-reporting is characteristic of individuals whether over time or by different assessment methods. J Am Diet Assoc. 2001;101:70–80. doi: 10.1016/S0002-8223(01)00018-9. [DOI] [PubMed] [Google Scholar]
- 38.Prentice RL, Sugar E, Wang CY, Neuhouser M, Patterson R. Research strategies and the use of nutrient biomarkers in studies of diet and chronic disease. Public Health Nutr. 2002;5:977–984. doi: 10.1079/PHN2002382. [DOI] [PubMed] [Google Scholar]
- 39.US Department of Health and Human Services. Physical activity and health: A report of the surgeon general. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion; 1996. [Google Scholar]
- 40.Strauss R, Rodzilsky D, Burack G, Colin M. Psychosocial correlates of physical activity in healthy children. Arch Pediatr Adolesc Med. 2001;155(8):897–902. doi: 10.1001/archpedi.155.8.897. [DOI] [PubMed] [Google Scholar]
- 41.Bungum TJ, Vincent ML. Determinants of physical activity among female adolescents. Am J Prev Med. 1997;13(2):115–122. [PubMed] [Google Scholar]
- 42.French SA, Story M, Fulkerson JA, et al. Increasing weight-bearing physical activity and calcium-rich foods to promote bone mass gains among 9 – 11 year old girls: outcomes of the Cal-Girls study. Int J Behavioral Nutrition and Physical Activity. 2005;2:8. doi: 10.1186/1479-5868-2-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.DeBar LL, Ritenbaugh C, Aickin M, et al. YOUTH: A health-plan based intervention increases bone density among teen girls. Arch Pediatr Adolesc Med. 2006;160(12):1269–76. doi: 10.1001/archpedi.160.12.1269. [DOI] [PubMed] [Google Scholar]
- 44.Owen N, Humpel N, Leslie E, Bauman A, Sallis JF. Understanding the environmental influences on walking: review and research agenda. Am J Prev Med. 2004;27(1):67–76. doi: 10.1016/j.amepre.2004.03.006. [DOI] [PubMed] [Google Scholar]
- 45.Frank LD, Schmid TL, Sallis JF, Chapman J, Saelens BE. Linking objectively measured physical activity with objectively measured urban form: findings from SMARTRAQ. Am J Prev Med. 2005;28(2S2):117–125. doi: 10.1016/j.amepre.2004.11.001. [DOI] [PubMed] [Google Scholar]
- 46.Atkinson JL, Sallis JF, Saelens BE, Cain KL, Black JB. The association of neighborhood design and recreational environments with physical activity. Am J Health Promot. 2005;19(4):304–309. doi: 10.4278/0890-1171-19.4.304. [DOI] [PubMed] [Google Scholar]
- 47.King A, Castro C, Wilcox S, Eyler A, Sallis J, Brownson R. Personal and environmental factors associated with physical inactivity among different racial-ethnic groups of U.S. middle-aged and older-aged women. Health Psychol. 2000;19(4):354–364. doi: 10.1037//0278-6133.19.4.354. [DOI] [PubMed] [Google Scholar]
- 48.Brownson R, Baker E, Houseman R, Brennan L, Bacak S. Environmental and policy determinants of physical activity in the United States. Am J Public Health. 2001;91(12):1995–2003. doi: 10.2105/ajph.91.12.1995. [DOI] [PMC free article] [PubMed] [Google Scholar]