

Abstract
Objectives:
The mitral valve is a complex structure that is altered by disease states. The classical image of the mitral valve is a bicuspid valve with two leaflets and two papillary muscles. The reason for the present study is to study the morphology and morphometry of the mitral valve.
Materials and Methods:
This study was carried out on 116 human cadaveric hearts. Hearts were opened along the left border through the atrioventricular valve. The diameter and circumference of the annulus was measured and the number of valve leaflets was observed.
Results:
The mean annular diameter was 2.22 cm. The mean circumference of mitral valve annulus was 9.12 cm. The standard description of the mitral valve is bicuspid. In the present study, we found the number of cusps to be variable, from monocuspid to hexacuspid and classified them accordingly.
Conclusions:
The mitral valve is not always a bicuspid valve. The number of cusps varies greatly. An increase in the number of the cusp and their improper approximation most likely causes various valvular disorders.
Keywords: Atrioventricular valve, leaflets/cusps, variation
INTRODUCTION
The mitral valve is a complex structure that is altered by various disease states and therefore is of great importance. Researchers are attracted to its study and clinical-based studies are frequently found in the literature. Anatomic and morphologic studies of the mitral valve are comparatively less. Those anatomic studies vary from paper to paper. Due to its clinical significance, paucity of anatomic studies and existing controversies, we had chosen this topic for research. The present study is about the morphology and morphometry of the mitral valve.
MATERIALS AND METHODS
This study was carried out on 116 human cadaveric hearts. The hearts were washed and opened along the left border through the atrioventricular valve. The cavity of the left atrium was opened. The left atrioventrcular orifice was cleared by removing the clots. The maximum diameter of the opening was measured with the Vernier caliper. Then the cavity of the left ventricle was opened and cleaned to visualize the mitral valve complex. Circumference of annulus was measured. Cusps of mitral valve were dissected. Number and the height of valve leaflets were measured.
RESULTS
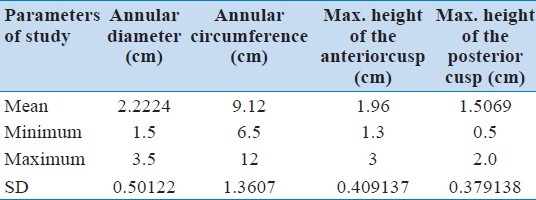
Morphometry of annular diameter, annular circumference, and height of anterior and posterior cusps are described in Table 1. The mean annular diameter was 2.22 cm, mean annular circumference was 9.12 cm. The mean of maximum height of anterior cusp and posterior cusp was 1.96 cm and 1.50 cm, respectively.
Table 1.
Morphometry of the mitral valve
In the present study the number of the mitral valve cusps was measured. The mitral valve was classified according to the number of the cusps [Table 2, Figures 1–9].
Table 2.
Classification of mitral valve according to the number of leaflets
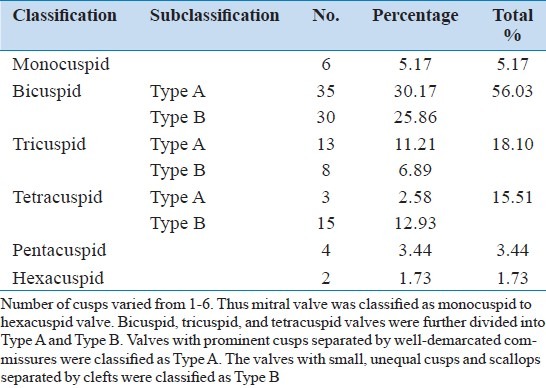
Figure 1.
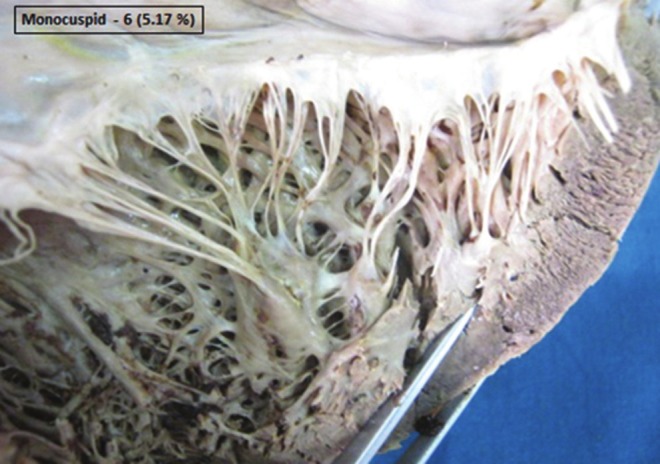
Monocuspid frill like mitral valve. In monocuspid valve, single frill like cusp was present. No well demarcated prominent commissure was seen
Figure 9.
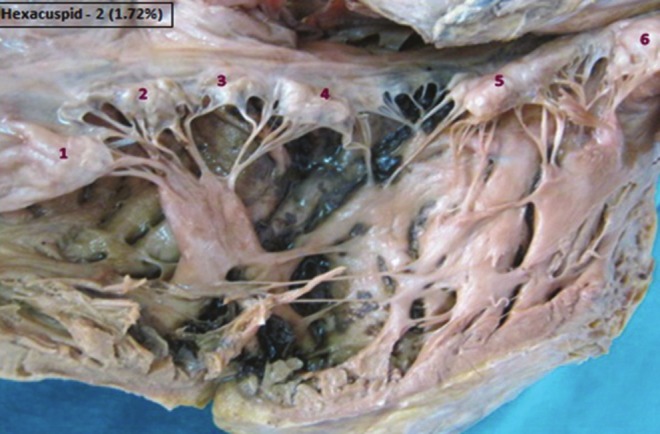
Hexacuspid mitral valve. Six unequal cusps (1, 2, 3, 4, 5, 6) were seen clearly
Figure 2.

Bicuspid mitral valve (Type A). In Bicuspid mitral valve two prominent cusps (1 and 2) were seen divided by two well marked commissures. So it is called as Type A of Bicuspid mitral valve
Figure 3.

Bicuspid mitral valve (Type B). In Type B of Bicuspid mitral valve, only one cusp was prominent (1). The next cusp was frill like with uniform height (2). Commissure between the two cusp was not well marked
Figure 4.

Tricuspid mitral valve (Type A) Three prominent cusps (1, 2 and 3) of equal size and shape separated by well marked commissure were present in Type A of tricuspid mitral valve
Figure 5.

Tricuspid mitral valve (Type B). In Type B of tricuspid mitral valve only one cusp (1) was large and prominent. The other cusp was divided into the two smaller cusps (2 and 3)
Figure 6.
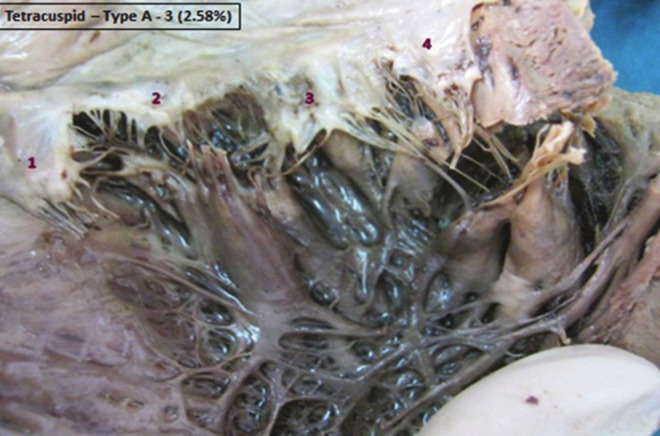
Tetracuspid mitral valve (Type A). Four promonent cusps (1, 2, 3, 4) separated by well marked commissures were present in Type A of tetracuspid valve
Figure 7.
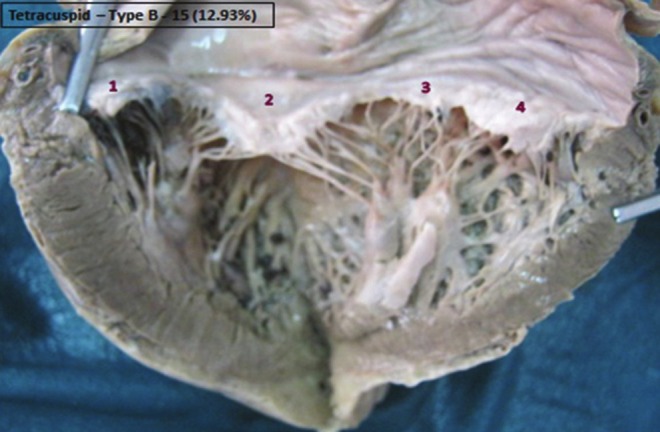
Tetracuspid mitral valve (Type B). In Type B of tetracuspid mitral valve four different cusps were seen clearly (1, 2, 3, 4). Out of those only one cusp was prominent (2). The other cusp was divided into three smaller cusps
Figure 8.

Pentacuspid mitral valve. Five unequal cusps (1, 2, 3, 4, 5) were present in a pentacuspid mitral valve
DISCUSSION
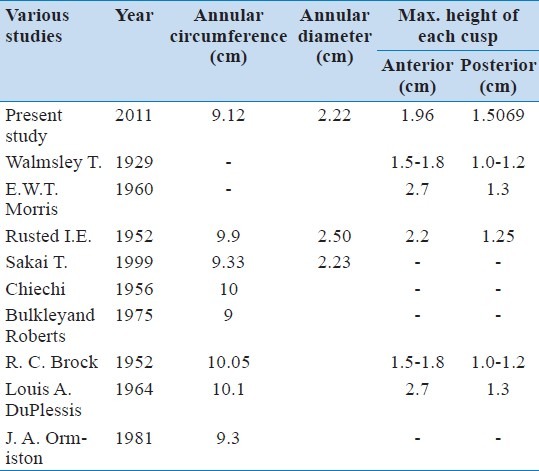
Variations of cusps described in the present study have their own morphologic significance: developmental, physiologic and surgical because of its great clinical importance, the mitral valve is the most common choice of research workers. There are numerous studies on mitral valve repair and its morphometry.[1–9] Table 3 shows the comparison of morphometry of the mitral valve. Results of the present study are in the range of previous studies.
Table 3.
Comparison of morphometry of mitral valve
As compared with the studies on the morphometry of the mitral valve, there are very few studies on the number of cusps present in the mitral valve. Distinctly different from the tricuspid valve, the mitral valve has two (2) leaflets. According to different books of anatomy it is fixed in our mind that there are 2 cusps present in the mitral valve, although some research workers argue that it has 4 leaflets.[10]
The free edge of the posterior leaflet is often divided into 3 or more scallops or described as lateral, middle, and medial or P1, P2, and P3 segments.[11] Although 3 scallops are most common, the scallops are not equal in size. Ranganathan and colleagues[12] found the middle scallop to be larger in the majority of hearts.
The standard book of Gray's Anatomy 39th ed.[13] (2005) stated that there was confusion and controversy in quantitation, because small accessory cusps are almost always found between the 2 major cusps.
Skwarek et al.[14] had studied the tricuspid valve and divided it into different types and subtypes depending on the number of leaflets and the location of accessory leaflets. On that basis the classification of mitral valve is done in the present study according to the number of leaflets. This easy and simple classification of mitral valve is done for the first time in the present study. There is no such classification found in the literature searched so far by us.
Kalangos et al.[15] have reported a rare case of congenital mitral insufficiency characterized by 6 well-demarcated leaflets of mitral valve. Such a type with 6 leaflets was seen in the present study in 1.72%. Increase in the number of cusps in a valve may not show any change in echocardiography unless and until there is any pathology. Increase in the number of cusps may increase the chances of Mitral regurgitation (MR) with the disturbances in edge-to-edge cusp closure.
Carpentier[11] developed a functional classification used to describe the mechanism of valvular dysfunction. Type I MR is characterized as normal leaflet motion. Type II MR lesions are related to leaflet prolapsed. Type III MR lesions are caused by restricted leaflet motion. Type IIIA MR shows restricted opening and type IIIB MR shows restricted closure.
Mitral valve repair is considered as the gold standard to treat mitral regurgitation. The re-emergence of the edge-to-edge approximation of the leaflets is commonly called the Alfieri technique.[16] This technique involves suturing together anterior and posterior leaflets at a single point midway between the circumferences of the leaflets creating the double-orifice. This technique in mitral valve repair is a simple solution for complex problems.
The mitral valve develops from cushion tissue and myocardium of the ventricle. Abnormal splitting of the cushion tissue may result in the increased number of cusps.[17] The technique of cusp commissuroplasty can be used to reconstruct atrioventricular valves that have been damaged by endocarditis of the commissure and adjacent cusps.[18]
An increase in the number of the cusp and their improper approximation will more likely cause various valvular disorders.
CONCLUSION
The present study has classified the mitral valve from monocuspid to hexacuspid valve as per the number of cusps. The most commonly described mitral valve is bicuspid but it was present in only 56% in present study. The mitral valve is not always a bicuspid valve. The number of cusps in it varies. Improper cusps approximation may cause mitral regurgitation. This knowledge may be useful for cardiothoracic surgeons in surgical repair of the mitral valve.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Walmsley T. The heart. In: Sharpey-Schafer E, Symington J, Bryce TH, editors. Quain's elements of anatomy. 11th ed. Vol. 4. London: Greens and Co; 1929. p. 42. Pt. 3. [Google Scholar]
- 2.Rusted IE, Schiefley CH, Edwards JE. Studies of the mitral valve I.Anatomic features of the normal mitral valve and associated structures. Circulation. 1952;6:825–31. doi: 10.1161/01.cir.6.6.825. [DOI] [PubMed] [Google Scholar]
- 3.Sakai T, Okita Y, Ueda Y, Tahata T, Ogino H, Matsuyama K, et al. Distance between mitral annulus and papillary muscles: Anatomic study in normal human hearts. J Thorac Cardiovasc Surg. 1999;118:636–40. doi: 10.1016/S0022-5223(99)70008-5. [DOI] [PubMed] [Google Scholar]
- 4.Morris EW. Some features of the mitral valve. Thorax. 1960;15:70. doi: 10.1136/thx.15.1.70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bulkley BH, Roberts WC. Dilatation of the mitral anulus.A rare cause of mitral regurgitation. Am J Med. 1975;59:457. doi: 10.1016/0002-9343(75)90252-1. [DOI] [PubMed] [Google Scholar]
- 6.Chiechi MA, Lees WM, Thompson R. Functional anatomy of the normal mitral valve. J Thorac Surg. 1956;32:378. [PubMed] [Google Scholar]
- 7.Brock RC. The surgical and pathological anatomy of the mitral valve. Br Heart J. 1952;14:489–513. doi: 10.1136/hrt.14.4.489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Du Plessis LA, Marchand P. The anatomy of the mitral valve and its associated structures. Thorax. 1964;19:221. doi: 10.1136/thx.19.3.221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ormiston JA, Shah PM, Tei C, Wong M. Size and motion of the mitral valve annulus in man. I. A two- dimensional echocardiographic method and findings in normal subjects. Circulation. 1981;64:113–20. doi: 10.1161/01.cir.64.1.113. [DOI] [PubMed] [Google Scholar]
- 10.Yacoub M. Anatomy of the mitral valve, chordae and cusps. In: Kalmanson D, editor. The mitral valve. London: Edward Arnold; 1976. pp. 15–20. [Google Scholar]
- 11.Carpentier A. Cardiac valve surgery: The “French correction”. J Thorac Cardiovasc Surg. 1983;86:323–37. [PubMed] [Google Scholar]
- 12.Ranganathan N, Lam JH, Wigle ED, Silver MD. Morphology of the human mitral valve II. The valve leaflets. Circulation. 1970;41:459–67. doi: 10.1161/01.cir.41.3.459. [DOI] [PubMed] [Google Scholar]
- 13.Standring S. Gray's Anatomy. 39th ed. Edinburgh: Elsevier-Churchill Livingstone; 2005. pp. 1006–8. [Google Scholar]
- 14.Skwarek M, Grzybiak M, Kosiñski A, Hreczecha J. Notes on the morphology of the tricuspid valve in the adult human heart. Folia Morphol. 2004;63:319–24. [PubMed] [Google Scholar]
- 15.Kalangos A, Oberhansli I, Khatchatourian G, Friedli B, Faidutti B. Multiple-leaflet mitral valve as a rare cause of congenital mitral insufficiency. Ann Thorac Surg. 1997;63:1452–5. doi: 10.1016/s0003-4975(97)00108-2. [DOI] [PubMed] [Google Scholar]
- 16.Alfieri O, Maisano F, De Bonis M, Stefano PL, Torracca L, Oppizzi M, et al. The double-orifice technique in mitral valve repair: A simple solution for complex problems. J Thorac Cardiovasc Surg. 2001;122:674–81. doi: 10.1067/mtc.2001.117277. [DOI] [PubMed] [Google Scholar]
- 17.Oosthoek PW, Wenink AC, Wisse LJ, Gittenberger-de Groot AC. Development of the papillary muscles of the mitral valve: Morphogenetic background of parachute-like asymmetric mitral valves and other mitral valve anomalies. J Thorac Cardiovasc Surg. 1998;116:36–46. doi: 10.1016/S0022-5223(98)70240-5. [DOI] [PubMed] [Google Scholar]
- 18.Lai DT, Chard RB. Commissuroplasty: A method of valve repair for mitral and tricuspid endocarditis. Ann Thorac Surg. 1999;68:1727–30. doi: 10.1016/s0003-4975(99)00663-3. [DOI] [PubMed] [Google Scholar]