

Abstract
Background:
Despite efforts to maintain the intestinal tissue and treat gastrointestinal disease, a large number of patients undergo ostomy surgery each year. Using stoma reduces the patient's quality of life (QOL) greatly. Although there are approximately 3000 patients in Iran; there is little information about the impact of stoma on their QOL.
Aims:
The study aims to evaluate QOL of stoma patients using a special measurement tool.
Settings and Design:
This survey was a cross-sectional study that was conducted on 102 random samples of stoma patients.
Materials and Methods:
The City of Hope Quality of Life-Ostomy Questionnaire was used for collecting demographic and clinical information and evaluating QOL.
Statistical Analysis Used:
Univariate and multiple regression analyses were performed to identify predictors of QOL.
Results:
The mean score for the overall QOL for stoma patients was 7.48 ± 0.9. 70% of patients were dissatisfied with sexual activities. More than half of them reported feelings of depression following stoma surgery. Univariate analysis indicated that factors such as the type of ostomy (temporary/permanent), the underlying disease that had led to the stoma, depression, problem with location of ostomy, and change in clothing style had significant effects on overall QOL and its subscales (P < 0.05). The results of the regression analyses showed that only depression and problem with the location of ostomy were statistically significant in predicting patients’ QOL and its subscales (P < 0.05).
Conclusions:
The findings demonstrated that living with stoma influences the overall aspect of QOL. Education for the patients and their families is important for improving the stoma patients’ QOL. Sexual and psychological consultation may also improve patients’ QOL.
Keywords: Depression, Ostomy, Quality of life, Sexual activity
INTRODUCTION
Nowadays, the conditions leading to stoma surgery are in the rise. Colorectal cancer is the most common cause of intestinal ostomy surgery.[1,2] For non-cancer patients, it is the inflammatory bowel disease which in most cases causes the creation of an ostomy.[3]
Despite efforts to maintain the intestinal tissue and treat these diseases, a large number of patients undergo ostomy surgery each year.[4] Using stoma, either permanent or temporary, greatly reduces the patient's quality of life (QOL).[5–7] Some patients complain about inflammation around the stoma, sleep disturbance, and inability to control gas.[4,8–10] Fear of the future and concerns about their relationships with families and friends are among some of the psychological problems these patients face.[4,8] The stoma patients suffered from sexual difficulties, restriction of physical activity, dietary restrictions, and in general changes in lifestyle.[2] Assessing QOL of stoma patients and its determinants will lead to better understanding of patient's QOL pattern and improving their QOL.
Although there are approximately 3000 patients currently living with ostomy in Iran (according to the Iranian ostomy society), quite a few studies have addressed the impact of stoma on patients’ QOL due to lack of specific valid and reliable instruments.[10,11] Only in one study, the QOL in stoma patients was evaluated without any use of specific tools for measuring the quality of life.[10] Therefore, this study aims to evaluate the QOL of stoma patients undergoing stoma surgery due to cancer or non-cancer diseases using a special measurement tool.
MATERIALS AND METHODS
This survey, which was designed as a cross-sectional study from March to October 2011, was carried out on 102 random samples of stoma patients who were referred to the Iranian Ostomy Society (IOS). The following are the criteria for inclusion of the patients to this study: Having adequate physical and mental health, having over 18 years of age, not having other chronic diseases affecting QOL, having had an ostomy in place for at least 3 months, and willingness to participate in the study. Any patient with psychological or emotional problems or a chronic disease affecting the QOL was excluded from the study.
To do the research, the aim of the study was first described for the patients and an informed consent was obtained from them to participate in the study and the patient's anonymity was also preserved.
In order to measure the stoma patient's QOL, the City of Hope Quality of Life-Ostomy Questionnaire (COH-QOL-Ostomy) was used. It is a disease-specific self-administrated questionnaire that is composed of two sections. The first section includes 46 questions about demographics, disease, treatment, ostomy specific, and other personal characteristics such as diet, work, and activity. The second section contains 43 items. These items are further divided into four subscales: physical (items 1-11), psychological (items 12-24), social (items 25-36), and spiritual (items 37-43) well-being and one global quality of life scale. A ten-point Likert scale questionnaire was used for this survey. The highest and the lowest points imply the highest and the lowest level of QOL, respectively. Subscale scores are calculated by the total scores of questions divided by the number of questions in each subscale. A total QOL score is obtained by the total scores of all questions divided by the number of questions; the score for each question varies from 0 to 10.[3,8,12]
The COH-QOL-Ostomy questionnaire was translated into Persian and validated. The findings showed high internal consistency of COH-QOL-Ostomy, interscale correlation, and discriminant validity (Anaraki F et al. 2011, unpublished data).
All data were entered in a database and analyzed with SPSS v.13.0 software. In accordance with the study objectives, descriptive analyses were used for different subscales and for the entire patients. Frequency distributions of demographic variables were obtained and the distribution of quantitative variables was described with the mean and standard deviation. To test the differences between the two groups, the Chi-square test was applied for binary and qualitative variables. For quantitative variables, t-test and ANOVA were used. A multivariate regression analysis was performed to identify predictors of QOL. For this procedure, the overall QOL score of the COH-QOL-Ostomy was treated as the dependent variable. Demographic data and variables relating to changes in life style were entered as explanatory factors in the model. Differences were considered significant at P < 0.05.
RESULTS
In total, 58 males (56.9%) and 44 females (43.1%) participated in the study. The mean age of the patients was 53.5 ± 12.3 years. The mean age of male patients was significantly higher than the female ones (56.6 ± 11.7 vs. 49.4 ± 11.9, P = 0.003). Colostomy was the most common type of stoma surgery (n = 69, 67.6%), and after that, ileostomy (n = 22, 21.6%) and urostomy (n = 11, 10.8%) were the common ones, respectively. In 80.4% of patients (n = 82), stoma had been permanently created. Stomas were made for 77.5% (n = 79) of the patients due to cancers. According to the patients’ reports, 83.3%, 82.4%, and 48% of stoma patients had been forced to change their job, diet, and clothing style, respectively. Considering the psychological implications after stoma surgery, approximately 63% (n = 64) had feelings of depression. Having problem with the location of ostomy was reported by 41.2% (n = 42) of the study sample.
While the majority of patients (81.4%) reported being sexually active before stoma surgery, only 33.3% resumed sexual activity after surgery. 32 patients (31.4%) were reported being satisfied with sexual activities, and 40.2% of male subjects had erectile problems.
83.3% of patients (n = 85) were members of an ostomy-specific support group. The mean length of time for patients to complete ostomy care was 39 min every day.
According to the reports of most patients, it took them at least 6 months to feel comfortable with the daily care and diet. The majority of ostomy patients had no restrictions on the consumption of specific foods such as carbonated beverages, dairy products, fruits, snacks, and vegetables.
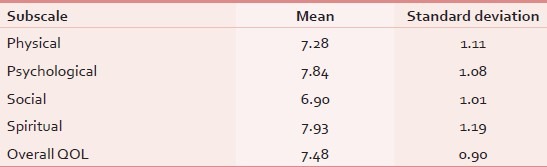
The mean score for the overall QOL in stoma patients was 7.48 ± 0.9. The best outcomes were found for the spiritual subscale and the social subscale scored the lowest [Table 1].
Table 1.
Mean and standard deviation of COH-QOL-Ostomy subscale scores
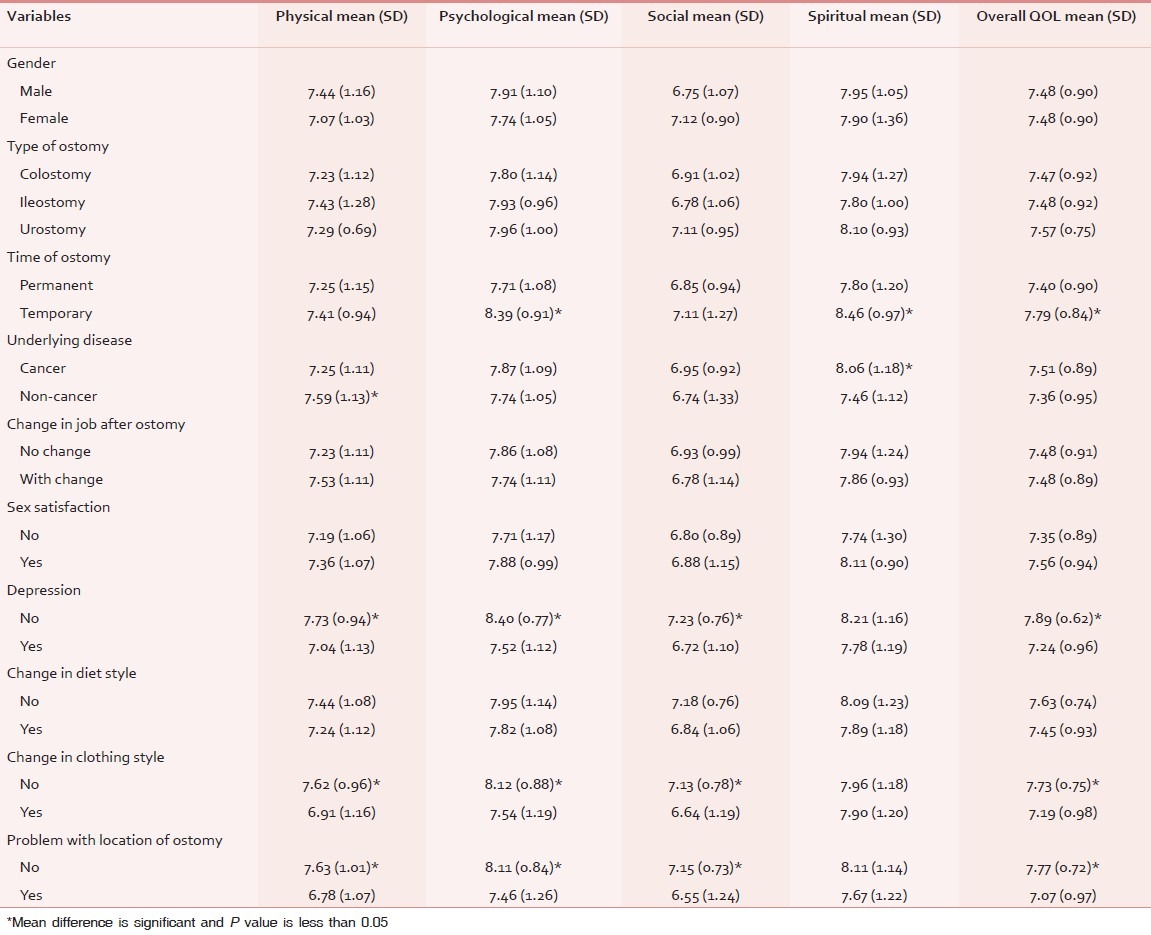
Univariate analysis indicated that the time of ostomy, the underlying disease that led to the stoma surgery, depression, problem with location of ostomy, and change in clothing style had significant effects on overall and its subscales. Findings of univariate analysis are shown in Table 2.
Table 2.
Mean difference of COH-QOL-Ostomy subscale scores according to demographic and clinical characteristics
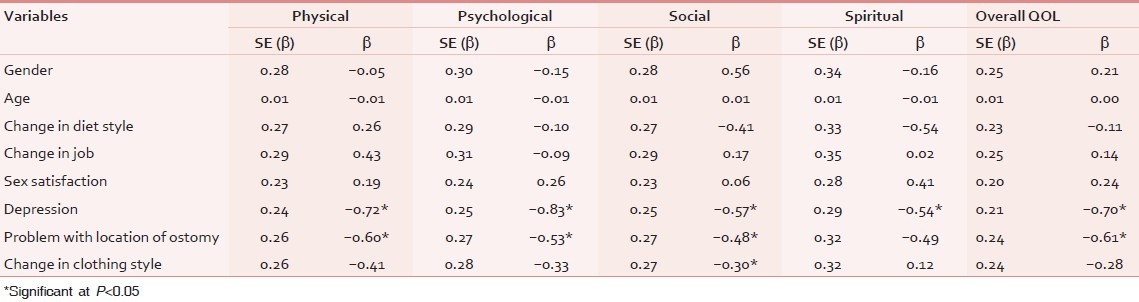
The results of the regression analyses showed that only depression and problem with location of ostomy were statistically significant in predicting patients’ physical, psychological, spiritual, and overall QOL subscales scores ( P < 0.05). In addition to the variables mentioned above, change in the way of dressing (due to stoma) was effective in predicting the social subscale score (P < 0.05) [Table 3].
Table 3.
Predictors of overall quality of life and its subscales in the linear regression model
DISCUSSION
Findings of the current study suggest that living with a stoma affects QOL. However, participants of this study, despite stoma surgery, had relatively good quality of life. The results also showed that these patients had more problems in social subscale and relatively good condition in spiritual subscale.
According to the results, most patients reported that they have lost their sexual activity after stoma surgery. The findings of the current study are consistent with other studies.[1,2,4,8,13] In a study conducted by Gemmill et al.,[14] it has been shown that 70% of patients had sexual activity before stoma surgery, while only 55% of patients resumed their sexual activity after surgery. In this study, the number of people who resumed their sexual activity after surgery is far less than (31%) the number reported in the Gemmill study.[14] This may be due to lack of proper training on sexuality issues to stoma patients in Iran. Therefore, it may be useful to refer stoma patients for counseling and training about sexual health.
In this study, most patients had a change in their diet due to problems in gas control; but most of them had coped with these conditions over time. Going on a diet can be effective to these patients in order to minimize gas and similar problems.[4,12]
About 40 percent of patients had problems with the stoma location which could be due to poor placement, use of improper appliance, development of a hernia, and leakage from stoma.[8,10,15,16] Another problem reported by the patients was a change in clothing style due to stoma surgery. Stoma patients, for reasons such as location of ostomy, weight changes, and changes in body appearance, were forced to change their clothing style, which itself reduced their quality of life.[6,8,12,14]
Like other studies,[12–14,17,18] more than half of the patients in this study were suffering from depression following stoma surgery. Since the depression had not been evaluated before stoma surgery, the relevant results should be interpreted cautiously.
Patients had a relatively good performance with regard to physical subscales, although reported some degree of physical problems. And this is perhaps because they had adapted themselves to these problems over time.
The results showed that social subscale scored the lowest among the other QOL subscales. It is perhaps because of the fact that physical and psychological disorders resulting from stoma may gradually reduce a person's confidence and reduce his social relations. These factors go hand in hand and lead to some degree of social isolation.[4,19,20] Like another study conducted in Iran,[4] the patients in this study had a favorable status in terms of the spiritual subscales. The findings have also been confirmed by another study conducted in the United States.[21]
As mentioned above, depression and problems with the location of ostomy were considered as predictors of overall QOL. But interpretation of these results is limited due to insufficient information about other factors affecting QOL.
This study faced some limitations. Causal inferences could not be made due to the cross-sectional design of the study. Also the study was only conducted on the patients of Iranian Ostomy Association and this undermines generalizability of the research findings.
In conclusion, the findings of this study showed that living with stoma influences the overall aspect of QOL. Proper placement of the stoma can decrease the patients’ difficulties. Pre-and post-operative education for the patients and their families is important so that the stoma patients’ QOL can be improved. Sexual disorders and feeling of depression were major problems of stoma patients. Sexual and psychological consultation may improve patients’ QOL. However, as the first study of its kind, this study needs other studies using multicenter data to confirm its results.
ACKNOWLEDGMENTS
We would like to express our appreciation to Mrs Minai (the ET nurse of IOS), Mrs Rostamzadegan, and Mrs Choopani (the secretariats of IOS) for their assistance in data collection.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Carlsson E, Berndtsson I, Hallen AM, Lindholm E, Persson E. Concerns and quality of life before surgery and during the recovery period in patients with rectal cancer and an ostomy. J Wound Ostomy Continence Nurs. 2010;37:654–61. doi: 10.1097/WON.0b013e3181f90f0c. [DOI] [PubMed] [Google Scholar]
- 2.Marquis P, Marrel A, Jambon B. Quality of life in patients with stomas: The Montreux Study. Ostomy Wound Manage. 2003;49:48–55. [PubMed] [Google Scholar]
- 3.Grant M, Ferrell B, Dean G, Uman G, Chu D, Krouse R. Revision and psychometric testing of the City of Hope Quality of Life-Ostomy Questionnaire. Qual Life Res. 2004;13:1445–57. doi: 10.1023/B:QURE.0000040784.65830.9f. [DOI] [PubMed] [Google Scholar]
- 4.Dabirian A, Yaghmaei F, Rassouli M, Tafreshi MZ. Quality of life in ostomy patients: A qualitative study. Patient Prefer Adherence. 2010;5:1–5. doi: 10.2147/PPA.S14508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Taylor C, Morgan L. Quality of life following reversal of temporary stoma after rectal cancer treatment. Eur J Oncol Nurs. 15:59–66. doi: 10.1016/j.ejon.2010.06.002. [DOI] [PubMed] [Google Scholar]
- 6.Neuman HB, Patil S, Fuzesi S, Wong WD, Weiser MR, Guillem JG, et al. Impact of a temporary stoma on the quality of life of rectal cancer patients undergoing treatment. Ann Surg Oncol. 18:1397–403. doi: 10.1245/s10434-010-1446-9. [DOI] [PubMed] [Google Scholar]
- 7.Siassi M, Hohenberger W, Losel F, Weiss M. Quality of life and patient's expectations after closure of a temporary stoma. Int J Colorectal Dis. 2008;23:1207–12. doi: 10.1007/s00384-008-0549-2. [DOI] [PubMed] [Google Scholar]
- 8.Krouse R, Grant M, Ferrell B, Dean G, Nelson R, Chu D. Quality of life outcomes in 599 cancer and non-cancer patients with colostomies. J Surg Res. 2007;138:79–87. doi: 10.1016/j.jss.2006.04.033. [DOI] [PubMed] [Google Scholar]
- 9.Silva MA, Ratnayake G, Deen KI. Quality of life of stoma patients: Temporary ileostomy versus colostomy. World J Surg. 2003;27:421–4. doi: 10.1007/s00268-002-6699-4. [DOI] [PubMed] [Google Scholar]
- 10.Mahjoubi B, Kiani Goodarzi K, Mohammad-Sadeghi H. Quality of life in stoma patients: Appropriate and inappropriate stoma sites. World J Surg. 2010;34:147–52. doi: 10.1007/s00268-009-0275-0. [DOI] [PubMed] [Google Scholar]
- 11.Momeni M, Ghanbari A. Comparison of Specific Quality of Life Between Urban and Rural Colorectal Cancer Patients. Govaresh. 2011;15:263–70. [Google Scholar]
- 12.Grant M, McMullen CK, Altschuler A, Mohler MJ, Hornbrook MC, Herrinton LJ, et al. Gender differences in quality of life among long-term colorectal cancer survivors with ostomies. Oncol Nurs Forum. 2011;38:587–96. doi: 10.1188/11.ONF.587-596. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Aronovitch SA, Sharp R, Harduar-Morano L. Quality of life for patients living with ostomies: Influence of contact with an ostomy nurse. J Wound Ostomy Continence Nurs. 2010;37:649–53. doi: 10.1097/WON.0b013e3181f90d16. [DOI] [PubMed] [Google Scholar]
- 14.Gemmill R, Sun V, Ferrell B, Krouse RS, Grant M. Going with the flow: Quality-of-life outcomes of cancer survivors with urinary diversion. J Wound Ostomy Continence Nurs. 2010;37:65–72. doi: 10.1097/WON.0b013e3181c68e8f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Colquhoun P, Kaiser R, Jr, Efron J, Weiss EG, Nogueras JJ, Vernava AM, 3rd, et al. Is the quality of life better in patients with colostomy than patients with fecal incontience? World J Surg. 2006;30:1925–8. doi: 10.1007/s00268-006-0531-5. [DOI] [PubMed] [Google Scholar]
- 16.Gooszen AW, Geelkerken RH, Hermans J, Lagaay MB, Gooszen HG. Quality of life with a temporary stoma: Ileostomy vs.colostomy. Dis Colon Rectum. 2000;43:650–5. doi: 10.1007/BF02235581. [DOI] [PubMed] [Google Scholar]
- 17.Black PK. Hidden problems of stoma care. Br J Nurs. 1994;3:707–11. doi: 10.12968/bjon.1994.3.14.707. [DOI] [PubMed] [Google Scholar]
- 18.Ito N, Tanaka M, Kazuma K. Health-related quality of life among persons living in Japan with a permanent colostomy. J Wound Ostomy Continence Nurs. 2005;32:178–83. doi: 10.1097/00152192-200505000-00006. quiz 184-5. [DOI] [PubMed] [Google Scholar]
- 19.Brown H, Randle J. Living with a stoma: A review of the literature. J Clin Nurs. 2005;14:74–81. doi: 10.1111/j.1365-2702.2004.00945.x. [DOI] [PubMed] [Google Scholar]
- 20.Fucini C, Gattai R, Urena C, Bandettini L, Elbetti C. Quality of life among five-year survivors after treatment for very low rectal cancer with or without a permanent abdominal stoma. Ann Surg Oncol. 2008;15:1099–106. doi: 10.1245/s10434-007-9748-2. [DOI] [PubMed] [Google Scholar]
- 21.Baldwin CM, Grant M, Wendel C, Rawl S, Schmidt CM, Ko C, et al. Influence of intestinal stoma on spiritual quality of life of U.S. veterans. J Holist Nurs. 2008;26:185–94. doi: 10.1177/0898010108315185. discussion 95-6; quiz 97-9. [DOI] [PubMed] [Google Scholar]