

Abstract
Background:
HelpAge India has been facilitating community-managed palliative care program in the villages of Tamil Nadu, India.
Objective:
To evaluate the effect of perceived quality of life in the elderly in the project villages in rural Tamil Nadu.
Materials and Methods:
It was a community-based evaluation study. Considering the mean difference of 0.6, design effect-2, precision-5%, power 80%, and 10% non-response, a sample size of 450 elderly persons (more than 60 years) was adequate. Sample was selected by two-stage cluster sampling. Tamil version of “WHO-Quality of Life-brief questionnaire” was used. Trained interviewers made house-to-house visits and obtained information by personally interviewing the subjects.
Results:
The mean score for perceived physical quality of life in the project area was (10.47 ± 1.80 SD) high than the mean score (10.17 ± 1.82 SD) in the control area (P = 0.013) and the mean score for psychological support (10.13 ± 2.25 SD) in project area was high than the mean score (9.8 ± 2.29 SD) in control area (P = 0.043). There was no effect on domain of social relationship and environment.
Conclusions:
In the project villages, the perceived physical quality of life and psychological support among elderly persons was significantly better than the control villages.
Keywords: Environment, India, Old age, Psychological, Physical, Quality of life, Rural, Social
INTRODUCTION
HelpAge India is a national-level voluntary organization, established with a mission to work for the cause and care of disadvantaged aged persons and to improve their quality of life.[1] Since the last 3 years, HelpAge India, has been facilitating community-managed palliative care program in 46 villages in Tamil Nadu, India. Similar to “neighborhood networks” in Kerala, the project strategy is based on mobilization of the elderly persons to form self-help groups (SHGs), SHG federations and facilitate activities for their own health care.[2] Community volunteers have been trained to identify the medical and social problems of the elderly and encouraged to intervene locally to help them.
A recent report on qualitative evaluation of this project anticipated a positive effect of this project on quality of life in the elderly in the project area.[3] The concept of quality of life encompasses wide range of aspects in human life, including physical, mental, social, spiritual, and environmental co-ordinates.[4] Health-related quality of life is increasingly used in health-care research, particularly in patient management, policy-level decisions, and resource allocation.[5] It has been found that individuals’ perception of their own health, perceived ability to manage financially, perception of poverty over time, and feelings of loneliness were found as important determinants of the quality of life of people aged 60 and more.[6] Quality of life and health care for elderly are upcoming issues in developing countries.[7] Hence, an objective of the present study was to evaluate the effect of perceived quality of life in the elderly in the project villages in rural Tamil Nadu.
MATERIALS AND METHODS
Settings
The present study was done in 46 project villages having total population of 131,114 in Tamil Nadu, a southern state of India. Adjacent 47 neighboring villages having a total population of 154,278 were selected as control.
Sample size
As there were no estimates available for quality-of-life scores in the area, we decided to use figures from a pilot study undertaken in the field practice area of Kasturba Rural Health Training Center, at village Anji, Mahatma Gandhi Institute of Medical Sciences (MGIMS), Sewagram during the year 2007-2008. The mean values for four domains – physical health, psychological support, social relations and environment were – 12.30 ± 1.69 SD, 12.09 ± 1.69 SD, 13.88 ± 1.77 SD, 13.16 ± 2.12 SD, respectively. Considering the mean difference of 0.6, design effect-2, precision-5%, and power 80%, the sample size was calculated for the mean values of each domain and the maximum sample size of 392 was considered (Calculated by Open Epi_info). The sample size of 392 was further inflated by 10% to cover the non-response. Thus, the final sample size was 432 in the project and the control area. It was rounded off to 450 in the project and control area.
Sampling technique
Two-stage cluster sampling was adapted to select a representative sample of the elderly persons (aged 60 or more years) from the study area (project area) and neighboring control area. In the first stage, 30 clusters were selected in each project and control villages by probability proportional to size technique. In the second stage, 15 elderly (above 60 years) were selected by systematic random sampling in each cluster. First household was selected randomly (r) and subsequently, next houses were selected by adding (K = Number of household/15, where 1 < r< K) interval in random number till the desired sample of 15 was achieved. If the selected house did not have any elderly or if house was locked, the immediate next house in the direction of movement was selected for that interview. If there were more than one elderly in the house, lottery method was used to select one. Sample of 450 was covered in Cuddalore, Nagapattinam, Vedharanyam (Project area). For comparison purpose, a sample of 450 was selected from the adjacent control area. Five percent of the questionnaires were re-checked by the supervisors to ensure the quality of data.
Interview tool
“WHO-Quality of Life-brief questionnaire” was used.[8] We have obtained permission from the World Health Organization to use this questionnaire for research purpose. It is developed by the WHOQOL Group with fifteen international field centers, in which one of the centers was Chennai, Tamil Nadu. We obtained a validated “Tamil” version of the questionnaire from World Health Organization (WHO). WHOQOL-brief allows detailed assessment of four domains of quality of life – physical health, psychological support, social relationships, and environment. It was developed considering different age groups, gender, and health conditions. It can be used for epidemiological studies for assessment of quality of life, establishing baseline scores in range of areas, looking at changes in quality of life over the course of interventions.
Interviewers and supervisors
A representative sample of elderly (aged 60 or more years) from the study area (project area) and neighboring control area was selected and interviewed by the trained interviewers. The interviewers were students of Masters in Social Work and Post-graduates in Community Medicine and supervisors were teaching faculties in the college of Social Work and in the department of Community Medicine. All of them were well-versed with the local language Tamil. All of them received training in communication skills required for administration of questionnaire. In a 2-day residential training program, they were explained the purpose and design of the study and importance of respondents’ consent. The training sessions were interactive and participatory in nature. We followed the guidelines by the National Family Health Survey-III, for training of interviewers and supervisors of the survey.[9] Training was followed by hands-on experience. Interviewers were taken to a nearby village, which did not have any cluster selected either in the project or control area. Interviewers were asked to interview at least two elderly and fill-up WHOQOL-brief questionnaires. They were asked to obtain the respondent's consent and administer the questionnaire. It was followed by feedback and discussion to resolve some problems faced during the hands-on experience. All the interviewers were given an identity card, a writing pad, questionnaires, and consent forms.
Administration of the questionnaire
Interviewers were instructed to greet the house members, show their identity cards, and introduce themselves. Later, interviewers were asked to read out the consent form to begin with and make them understand the purpose of the study. After obtaining the consent from the respondent, socio-demographic information was obtained. Interviewers were asked to read each question and rate the scale on the point which is most close to the response given by the respondents.
Data entry and analysis
The data was entered and analyzed by using Statistical Package for Social Sciences 12.0.1 software. We used WHOQOL syntax for calculation of mean values of four domains. The mean scores for “perceived” quality of life for domains such as – physical health, psychological health, social relations, and control of environments were calculated and compared for the sample of study and control area. High mean values signified better quality of life. Statistical significance was set at 5% (P < 0.05).
Ethics
The ethical clearance from the Institutional Ethics Committee of Sri Manakula Vinayagar Medical College and Hospital, Pondicherry was obtained.
RESULTS
Socio-demographic characteristics of sample inproject and control villages
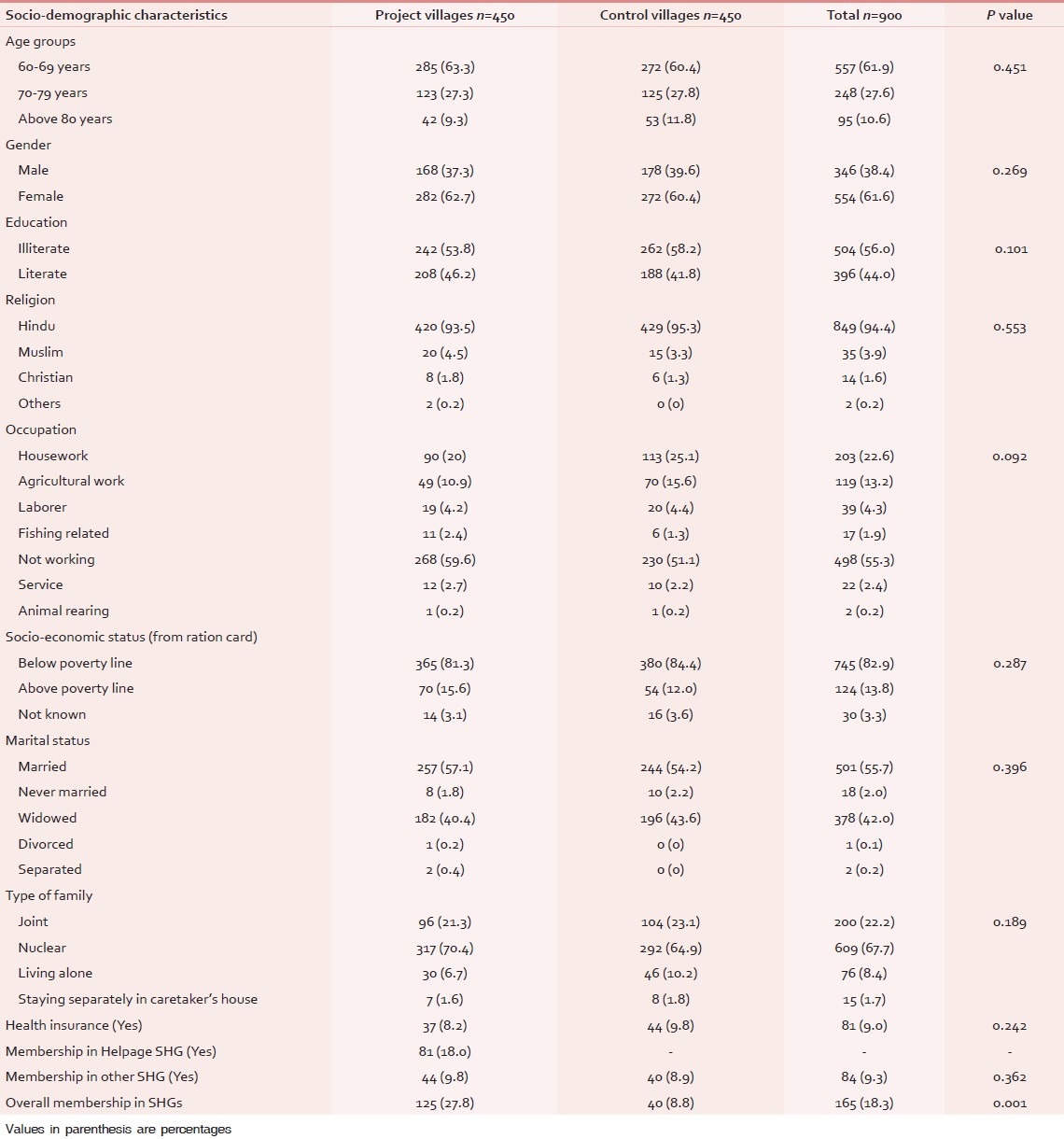
There was no significant difference in the project villages and control villages with respect to age groups, gender, religion, occupation, socio-economic status, marital status, and type of family. Noteworthy, 125 elderly (27.8%) were members in SHGs in project villages and 40 elderly (18.7%) were members in SHGs in control villages (P < 0.05) [Table 1]. There was no statistically significant difference in project and control villages with respect to utilization of government schemes. Thus, except for significant social mobilization in project villages, proportions of other variables are same in both the project and control villages. This makes the two samples comparable in further analysis.
Table 1.
Socio-demographic profile of sample in the project and control villages
Self-reported chronic morbidities and health care seeking among theelderly
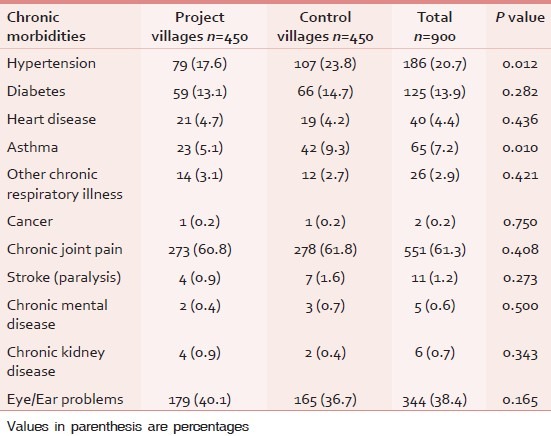
Most common self-reported chronic morbidities among elderly people in the project and control villages were chronic joint pain (61.3%) and eye/ear problems (38.4%). The difference in prevalence of these chronic morbidities was not statistically significant in the project and control villages. Other common morbidities were hypertension (HT) (20.7%) and diabetes (13.9%). The prevalence of hypertension and asthma was significantly low in the project villages (Hypertension-17.6% in project vs. 23.8% in control villages, asthma – 5.1% in project villages vs. 9.3% in control villages). In other chronic morbidities such as heart disease (4.4%), chronic respiratory illness (2.9%), stroke (1.2%), chronic mental illness (0.6%), there was no significant difference in the prevalence of chronic morbidities in project and control villages [Table 2].
Table 2.
Self-reported chronic illnesses among the elderly in the project and control villages
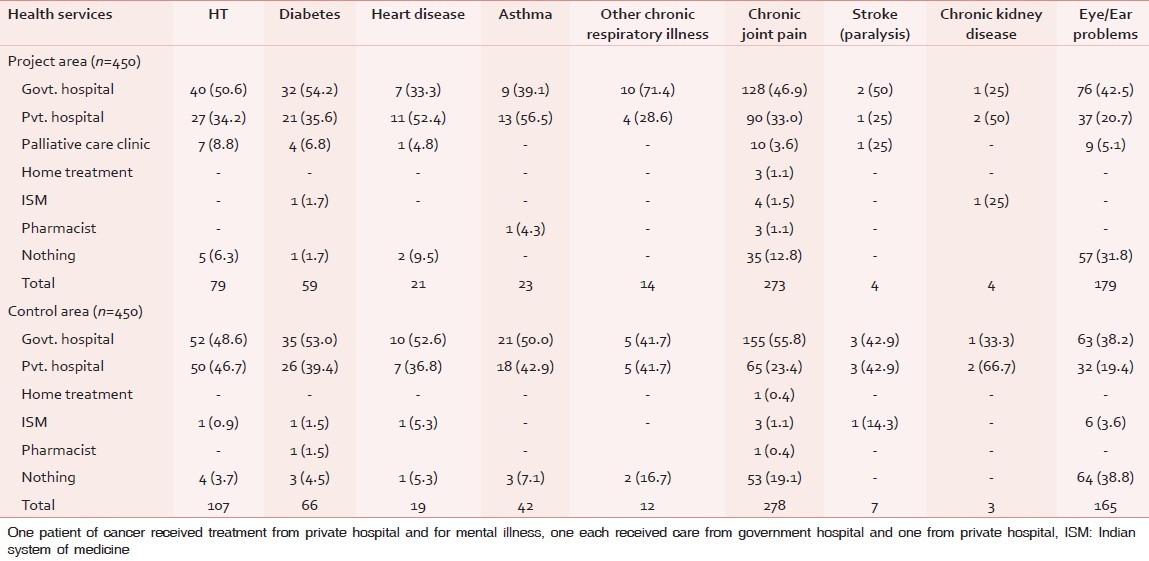
In both the project and control villages, most of the elderly with chronic morbidities accessed the government health-care services followed by the private health-care providers. The utilization of Indian systems of Medicine (Ayurveda, Siddha, and Unani) was 3.6% in control villages [Table 3].
Table 3.
Health care seeking of the elderly people with chronic morbidities
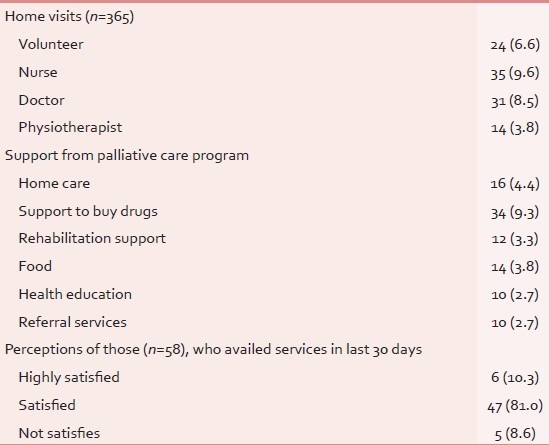
In a month, out of 365 elderly respondents in project area, having at least one chronic morbidities, 31 (8.5%) received home care from a medical doctor, 35 (9.6%) got home care from the Nurses, 24 (6.6%) received home visits by the community volunteers, and 14 (3.8%) received physiotherapy services at the village level. About 34 (9.3%) elderly received help to buy medicine, 16 (4.4%) received home care, 12 (3.3%) elderly reported that they were rehabilitated, 14 (3.8%) got food support and remaining 10 each (2.7%) got health education and referral services. Noteworthy, out of 58 elderly, who availed services in the last 30 days, 6 (10.3%) were highly satisfied, 47 (81%) were satisfied, and five (8.6%) were not satisfied [Table 4].
Table 4.
Village-level services from “palliative care program” in last 30 days to elderly in the project area
Quality of life in the elderly in project and control villages
The mean scores of “perceived physical health” in project villages (10.47 ± 1.80 SD) was significantly higher than the mean score in control villages (10.17 ± 1.82 SD) (P = 0.013). The mean scores of “perceived psychological health” in project villages (10.13 ± 2.25 SD) was significantly higher than the mean score in control villages (9.8 ± 2.29 SD) (P = 0.043).There was no significant difference in mean scores of “perceived social relations” and “perceived environment” among elderly in the project and control villages [Table 5].
Table 5.
Perceived quality of life in the elderly in the project and control area
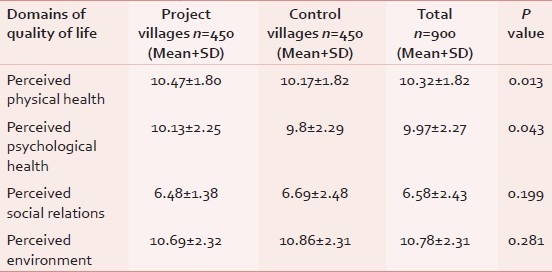
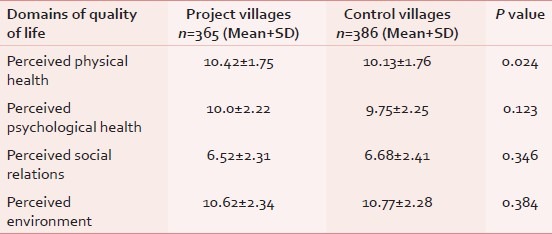
Table 6 shows perceived quality of life among the elderly who had at least one of the chronic morbidities. The mean score for “perceived physical health” among elderly in project villages (10.42 ± 1.75 SD) is high than the mean score of perceived physical health among the elderly in control villages (10.13 ± 1.76 SD; P = 0.024). There was no significant difference between mean scores of “perceived social relations” and mean scores of “perceived environment” among elderly with chronic morbidities in the project and control villages.
Table 6.
Perceived quality of life in the elderly with atleast one of the chronic morbidities
DISCUSSION
We found that the model of “community-managed” palliative care program could improve perceived physical quality of life and psychological support among the elderly. The project activities could successfully involve the elderly in their own care. Health clinics and physiotherapy units at village level, support of local community volunteers, and partnership with the government health-care providers ensured the continuum of medical care to sick elderly from village to district level. Noteworthy, the National policy on older persons, 1999 by the Government of India recommends an establishment of elderly managed “National Association of Elderly Persons” to mobilize senior citizens to carry out program and activities for their wellbeing.[10] The present model was found effective to improve quality of life in the elderly and appears as an effective approach for up-scaling in other rural settings of India.
However, as perceived by the elderly in the project villages, there was no effect on domain of social relationship and environment which also determines the quality of life. Those elderly people, who received care by the project team perceived better “social relationship” than those who did not receive any care. The quality of life has been regarded as a multi-dimensional construct related to health, economic circumstances, social support, participation in social activities, and housing issues, which may vary according to the nature of sample studied, the contextual or environmental situation, and the methodology and design of the study.[6]
Most of the medical problems among elderly people were chronic in nature which needed long- term care and follow-up. Such chronic conditions produce stress in patients and in their family caregivers. Thus, educating family caregivers in nature, progress, and the role of treatment in such chronic health conditions becomes an essential step to ensure elderly friendly environment at the family level. National old age policy 1999, also recommended strengthening of counseling services to relieve intra-familial stresses.[10]
The prevalence of chronic morbidities was found to be high among the elderly people. Noteworthy, the chronic conditions such as hypertension, diabetes, and other vascular conditions are the risk factors for vascular dementia – a degenerative mental health condition among the elderly. Hence, apart from medical care and follow-up, there is a need for risk factors reduction (reducing tobacco, alcohol consumption, promoting physical activity, etc.) program and mental health care program for the elderly people.
Considering the high utilization of government and private health services by sick old people, there is a need to improve the readiness of government health facilities and build partnership with the private providers/non-government organizations. Also, Indian system of Medicine may be utilized for the care of chronically sick old people to provide them better medical care. There is a need of integrated team work to ensure continuum of care from home to hospital. At village level, support group of community volunteers, Auxiliary Nurse Mid-wife (ANM), Accredited Social Health Activist (ASHA) – community-based female health worker, can ensure screening and referral of the patients. At the secondary level, as done in this project of HelpAge India, helpdesk at health-care facilities and palliative care centers can be set up through community participation. Apart from this, health-care staff at all levels needs training in geriatric care. Notably, it is one of the objectives of recently proposed “National Program for the National Care of the Elderly (NPHCE).”[11]
Most of our recommendations are in alignment with the policy prescriptions of the National policy for elderly, 1999 in India. The present project was based on the philosophy of participatory research where community was empowered by their active involvement in program planning and implementation. It has shown a positive effect on perceived quality of life in the elderly people.
ACKNOWLEDGMENT
We are thankful to WHOQOL group, Program on Mental Health, World Health organization, Geneva for their permission to use WHOQOL brief questionnaire. We are thankful to HelpAge India for funding this study.
Footnotes
Source of Support: HelpAge India and Coraid, Netherlands.
Conflict of Interest: None declared.
REFERENCES
- 1.HelpAge India. Online. [Last accessed 2012 May 15]. Available from: http://www.helpageindia.org/about.us.php .
- 2.Paleri A, Numpeli M. The evolution of palliative care programs in North Kerala. Indian J Palliat Care. 2005;11:15–8. [Google Scholar]
- 3.Evaluation of Community-managed Palliative Care Plus Project. [Last accessed 2012 May 15]. Available from: http://www.helpageindiaprogramme.org/RURAL/Elder_Self_Help_Groups (ESHGs)/Success_so_far/success_so_far_pdf/Evaluation%20of%20Community%20Based%20Palliative%20Care.pdf .
- 4.Farquhar M. Elderly people's definitions of quality of life. Soc Sci Med. 1995;41:1439–46. doi: 10.1016/0277-9536(95)00117-p. [DOI] [PubMed] [Google Scholar]
- 5.Hoi LV, Chuc NT, Lindholm L. Health-related quality of life, and its determinants, among older people in rural Vietnam, BMC Public Health. [Last accessed 2012 May 15];2010 10 doi: 10.1186/1471-2458-10-549. Available from: http://www.biomedcentral.com/1471.2458/10/549 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Smith AE, Sim J, Scharf T, Phillipson C. Determinants of quality of life amongst older people in deprived neighbourhoods. Ageing Soc. 2004;24:793–814. [Google Scholar]
- 7.Smith AE. Quality of life: a review. Educ Aging. 2000;15:419–35. [Google Scholar]
- 8.Geneva: The World Health Organization; 2000. World Health Organization – Quality of life: WHOQOL-BREF: Australian version. [Google Scholar]
- 9.National Family Health Survey. Interviewer's manual. (Online) [Last accessed 2010 Mar 03]. Available from: http://www.nfhsindia.org/manuals.html .
- 10.National Policy on Older Persons. Ministry of Social Justice and Empowerment. Government of India. Online. [Last accessed 2012 Jan 25]. Available from: http://www.socialjustice.nic.in/hindi/pdf/npopcomplete. pdf .
- 11.National Program for the National Care of the Elderly. Online. [Last accessed 2012 Jan25]. Available from: http://www.jkhealth.org/notifications/bal456.pdf .