

Abstract
Background:
Although high levels of subjective well-being (SWB) are common in old age, a subset of older individuals is disproportionately vulnerable to negative affect. Yoga has been shown to have many short-term benefits, but researchers have not determined whether a long-term or frequent yoga practice increasingly protects older women from low levels of psychological well-being.
Aims:
The purpose of this study was to examine the extent to which psychological attitudes, transcendence, mental mastery, and subjective vitality in a sample of female yoga practitioners over 45 years varied according to the length and frequency of yoga practice.
Materials and Methods:
We administered online surveys to a non-probability sample of 211 female yoga practitioners 45 to 80. We used weighted least squares regression analyses to evaluate the relationship of extent of yoga experience to the outcome variables after accounting for age and lifestyle factors.
Results:
Participants had practiced yoga for as long as 50 years and for up to 28 h per week. There were significant positive relationships between yoga experience and all outcome variables. These significant relationships remained after accounting for age and lifestyle factors. When we computed yoga experience in terms of total calendar years, without accounting for hours of practice, significant relationships did not remain. Transcendence of the ordinary was the most strongly associated with current yoga practice frequency, and positive psychological attitudes were the most strongly associated with total lifetime hours of practice.
Conclusions:
Among a non-probability sample of female yoga practitioners between 45 and 80 years, increased yoga experience predicted increased levels of psychological well-being. Results showed a dose-response effect, with yoga experience exercising an increasingly protective effect against low levels of SWB and vitality.
Keywords: Aging, vitality, well-being, women, yoga
INTRODUCTION
Wellness practices are believed to trigger self-healing mechanisms and intrinsic adaptogenic responses.[1] According to the theory of salutogenesis, the regular engagement in wellness practices, or salutary behaviors, creates steady improvements in physical and psychological health.[1,2] From the perspective of this theory, there is not an upper limit to the level of health that an individual can attain.
Well-being is not defined as the absence of problems.[3–8] Positive well-being is not the polar opposite of negative mood, and the inverse correlation between the two constructs is somewhat weak.[9,10] In the worldview of humanist and positive psychology, one cannot create a life worth living by focusing entirely on alleviating disease and discomfort.[11] The most serious psychopathologies are believed to result from an absence of strengths, rather than from symptoms such as depression and anxiety.[3] Although wellness practices protect against pathology,[1,3,12] a major and perhaps underrepresented purpose of lifestyle-based wellness choices is to maximize positive experiences such as joy, vitality, serenity, happiness, self-actualization, and other qualities that make life worth living.[13]
Yoga is an ancient set of integrated mental and physical practices designed to foster the long-term experience of positive psychological states, including transcendence of the ordinary, spirituality, self-awareness, and inner peace.[14,15] Historically, yoga has been practiced primarily not as a remedy for defined pathologies, but as a practice to enhance lifelong physical and spiritual well-being. Research studies have shown that yoga can provide a wide range of psychological benefits,[16,17] both in reducing negative affect[18–20] and in fostering positive wellness.[21–26]
Enduring well-being does not emerge in a brief time period in response to specific events.[27] A state of long-term, highly developed wellness is stable, yet can be developed and cultivated with time and effort.[28] The wellness process is recursive, and the outcomes of a long-term wellness practice are unpredictable and multifaceted.[29,30]
The frequent and long-term practice of Hatha yoga (a form of yoga with emphasis on physical postures) has been shown to predict physical wellness among older women, as measured by a lower body mass index and reduced medication load.[31] Yoga practitioners have maintained that the benefits of yoga, including positive attitudes, subjective vitality, transcendence of the ordinary, and mental mastery, accrue over a long timeframe or with more frequent practice.[32] However, most studies of the effects of yoga experience have involved short-term interventions with beginners, lasting between a few days and a few months.[16–25] The full benefits of yoga may therefore be underestimated in the literature.[32]
For this study, positive psychological attitudes are defined to include serenity under pressure, interest and satisfaction in life, a sense of purpose, contentment with self and life, meaning in one's work, low levels of worry and anxiety, a sense of self-worth, hope, and self-confidence.[33] Transcendence of the ordinary is described as awareness beyond day-to-day and rational existence.[26] Following Sell and Nagpal,[27] transcendence is defined for this study to include feelings of oneness with surroundings, intense happiness, ecstasy, bliss, or unity with the entire human community. Similarly, mental mastery is defined for this study as a low level of anxiety, sadness, irritability, and depression.[27] Subjective vitality is a construct that spans both psychological and physical wellness.[34] Defined as zest, enthusiasm, vigor, and the experience of having energy and aliveness, subjective vitality both correlates with and contributes to health and well-being across all age groups.[34]
Overall, subjective well-being has been found to decline in midlife and rise in old age.[35] These increases in emotional well-being and life satisfaction in old age occur despite both material and social losses.[35,36] Conversely, longitudinal studies have shown that high levels of SWB predict reduced odds of mortality and disability.[35]
In a brief experimental study, Stanley and Isaacowitz[37] found that the happiest group of individuals included a higher proportion of older adults, but the same was true of the unhappiest group. Thus, although there are clearly age-related factors involved in enhancing SWB in the elderly, there is value in discovering lifestyle factors that may protect from low levels of SWB even among a population in which high levels of SWB are common. Health is an important predictor of subjective well-being (SWB) for all age groups and the strongest predictor during late life.[35]
MATERIALS AND METHODS
In this observational, cross-sectional study, we tested the hypothesis that an increasing level of Hatha yoga practice was associated with higher levels of positive psychological attitudes, mental mastery, subjective vitality, and transcendence of the ordinary in women over 45 years. We located participants through postings to senior lists, health clubs, religious organizations, social action networks, online university lists, and charitable organizations. In addition, we asked yoga teachers to distribute flyers and notifications to yoga students, and we invited members of online yoga lists to participate. We defined yoga practitioners as individuals who reported nonzero hours per week of current yoga practice and nonzero prior history of yoga practice. We defined yoga to include asana (postures), practiced along with controlled breathing and meditation.
Further details for the recruitment of the sample of 211 yoga practitioners, along with data collection methods, have been reported in a previous publication.[31] The Institutional Review Board of Northcentral University granted permission in October 2009 to conduct the study. Data were collected in October and November 2009. Participants indicated informed consent by a selection on the first screen of the survey. All measures were self-reported.
Measures
Predictor and outcome variables
The predictor variables for this study were current hours per week of Hatha yoga, total lifetime hours of Hatha yoga practice, and total calendar years of Hatha yoga practice. Participants entered one line of information for each period of yoga practice in their lives, indicating the years and months of the practice and the hours per week practiced during that period. Definitions and data collection methods for the predictor variables have been reported in further detail in a previous publication.[31]
Participants provided data for age, educational level, marital status, height, weight, levels of processed food consumption, hours of non-yogic exercise per week, and hours of seated meditation per week. Participants reported the level of processed food consumption on a Likert-type scale in response to the question, “I eat a lot of refined sugar, refined flour, and processed food.” Values ranged from 1 (very true) to 7 (not at all true), with higher scores representing lower levels of processed food consumption. Further definitions and data collection methods of covariates were reported in a previous publication.[31] The outcome variables were positive psychological attitudes, mental mastery, transcendence, and subjective vitality.
Positive attitudes
The Inventory of Positive Psychological Attitudes[33] was used to identify positive psychological attitudes that promote health. Questions were asked about daily satisfaction, responses to stress, personal growth, life purpose, self-image, joy, and hope. The scale contained 32 items, with each item measured on a semantic differential scale with responses ranging from 1 to 7. Definitions of the anchors of the scale varied from one question to the next. For example, an item introduced with the phrase, “When I think about what I have done with my life, I feel” had anchors of “worthwhile” and “worthless.” Thirteen of the items were reverse scored. The composite scale has been shown to be reliable and to have good concurrent validity. The author of the instrument granted permission for use. The instrument was designed for electronic collection of data.[33]
Transcendence and mental mastery
The Subjective Well-Being Inventory, published by the World Health Organization, was developed in India and has been tested in several different population groups and languages.[27] The instrument was developed in response to a dearth of measures for positive mental health, in contrast to the many studies available on disease, disability, and disorders.[27] The scale consisted of semantic differential items with values ranging from 1 to 3. We selected the three-item Transcendence subscale (SUBI-T) and the five-item Inadequate Mental Mastery subscale (SUBI-MM) for use in this study. As increased transcendence was represented with lower scores, we reverse-coded the values for transcendence. Increased levels of inadequate mental mastery were represented with lower scores. Therefore, higher scores on the SUBI-MM indicated higher levels of mental mastery, and we did not reverse-code the scale.
The Subjective Well-Being Inventory was developed and validated primarily by a systematic qualitative process known as the stepwise ethnographic method.[27] Researchers began with unstructured interviews with participants, conducted meetings with interviewers and experts, and proceeded iteratively to clarify concepts. Final qualitative validation was achieved by means of focus group discussions with participants. Factor analyses were then used to verify the subscales, and normal distribution was confirmed. Although the entire instrument was in the public domain, permission was granted for the use of the selected subscales and for online data collection. Questions for the SUBI-T addressed feelings of ecstasy, bliss, and unity with the cosmos. The SUBI-MM included questions such as, “Do you sometimes feel sad without reason?” and “Do you feel disturbed by feelings of anxiety and tension?”
Subjective vitality
As a marker for psychological wellness, subjective vitality has been inversely associated with conditions such as depression and anxiety, and positively associated with life satisfaction, self-actualization, self-efficacy, self-determination, pain tolerance, positive mood states, and adherence to exercise.[34] Subjective vitality has also been positively correlated with long-term personality traits such as autonomy and the capacity for intimacy. As a marker for physical wellness, subjective vitality is positively correlated with measures of physical self-efficacy and bodily functioning, and has been shown to decline with age.[34] Subjective vitality has been inversely associated with increased tension, immunological dysfunction, and various physical illnesses[38] and has been shown to be undermined by lifestyle behaviors such as poor diet, smoking, and lack of exercise. Subjective vitality was found to be lower among patients in a pain clinic, and much lower among patients who experienced the pain as disabling or frightening.[34]
The Subjective Vitality Scale[34] originally contained seven items, but the more recent version of six items was found to be more internally reliable and to load on only one factor.[39] The instrument included questions such as, “I have energy and spirit” and “I feel alive and vital.” Items were represented on a Likert-type scale with values ranging from 1 (not at all true) to 7 (very true). Correlations with moods, as assessed by the Profile of Mood States, were non-significant except for scales of fatigue, depression, and particularly vigor. The author of the Subjective Vitality Scale granted permission to use the scale. The instrument was designed for electronic collection of data.
Statistical analyses
We computed bivariate correlations to determine the relationship between yoga experience and all outcome variables. We then performed weighted least-squares (WLS) regression analyses to determine the contribution of yoga practice to outcome variables after correcting for covariates. The covariates evaluated included age, marital status, educational level, BMI, hours of non-yogic exercise per week, level of processed food consumption, and hours of seated meditation per week. For the purposes of these analyses, we deconstructed yoga experience to represent experience in the practice of asana (yoga postures) practiced with breathing and conscious awareness, and we reported hours per week of seated meditation as a separate variable. However, in the interpretation of the results, we recognized asana and seated meditation as part of a unified system of yoga practice.
We initially entered all covariates into each model. We then removed non-significant covariates and entered a reduced model, including only the covariates that were significant in the previous model. We continued this process iteratively until all covariates showed significant results. Both standardized and non-standardized coefficients are reported, together with significance levels for each covariate in the model.
RESULTS
There were 211 usable records for yoga participants, representing a completion rate of 80.9%. For 14 participants, data were incomplete for total calendar years and total lifetime hours of practice. Participants exercised an average of 4.21 h per week (SD = 2.80), excluding yoga practice, and engaged in seated meditation an average of 2.56 h per week (SD = 3.26). Frequency distributions for the sample and the handling of outliers were reported in further detail in a previous publication.[31]
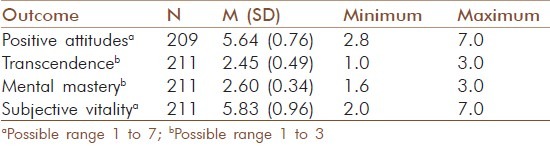
Table 1 shows the frequency distributions of all outcome variables. All mean scores exceeded the scale midpoint. As outcome measures showed a normal distribution of residuals, we used parametric statistics to conduct the analyses.
Table 1.
Mean scores, psychological outcomes
Bivariate correlations
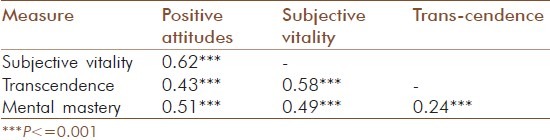
Measures of Hatha yoga experience (current hours per week, total lifetime hours, and total calendar years) were significantly intercorrelated [Table 2]. Psychological measures (positive psychological attitudes, transcendence, mental mastery, and subjective vitality) were also significantly intercorrelated, P < 0.001 [Table 3].
Table 2.
Intercorrelations for measures of Hatha yoga experience
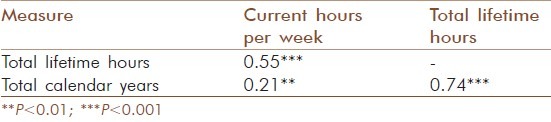
Table 3.
Intercorrelations for psychological outcomes
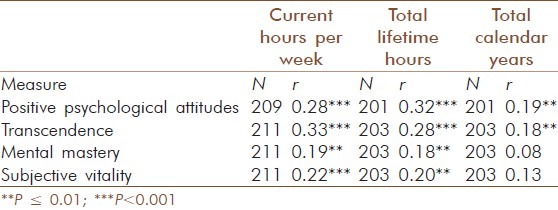
Current hours per week of Hatha yoga experience and total lifetime hours of yoga practice were positively correlated with all outcome variables [Table 4]. Total calendar years of Hatha yoga experience were positively correlated with positive psychological attitudes, r (207) = .19, P = .007; and with transcendence, r (209) = .18, P = 0.01. The bivariate relationships of total calendar years with mental mastery and subjective vitality were not significant.
Table 4.
Bivariate correlations: Hatha yoga experience with psychological outcomes
Weighted least squares regressions
The variances of the scores were not distributed equally. High levels of yoga experience predicted high outcome scores, but low levels of yoga experience did not predict low outcome scores [Figure 1]. Therefore, WLS regressions were used to perform the regression analyses.
Figure 1.
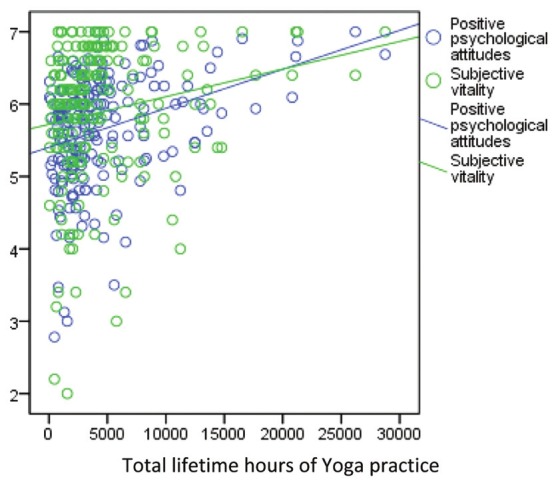
Yoga practice (total lifetime hours) versus positive attitudes and subjective vitality
Positive psychological attitudes
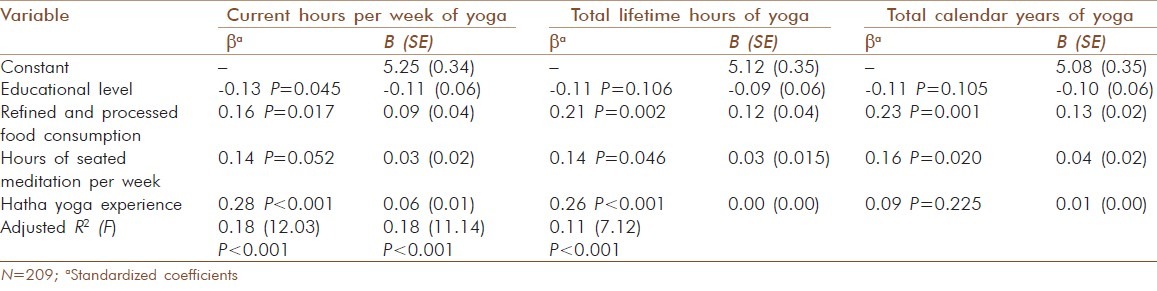
We evaluated the extent of yoga experience as a predictor of the level of positive psychological attitudes over and above significant covariates. Age, marital status, BMI, and hours of non-yogic exercise per week did not contribute significantly to positive psychological attitudes for any regression model. Therefore, we used a reduced model, including only educational level, level of refined and processed food consumption, and hours of seated meditation per week as covariates. Educational level predicted a significant outcome only when current hours per week were used as a predictor, P = 0.045. The relationship was inverse. Both current hours per week and total lifetime hours accounted for a significant proportion of the variance in the level of positive psychological attitudes, P < 0.001, over and above the contribution of covariates [Table 5]. The contribution of total calendar years was not significant.
Table 5.
Predictors of positive psychological attitudes
Transcendence of the ordinary
We evaluated the extent of yoga experience as a predictor of the level of transcendence of the ordinary over and above significant covariates. Hours of seated meditation per week were the only covariate to contribute significantly to the outcome for any regression model. The contribution of current hours per week to the outcome was significant, P < 0.001. The contribution of total lifetime hours to the outcome was significant, P = 0.001 [Table 6]. The contribution of total calendar years to the outcome was not significant.
Table 6.
Predictors of transcendence

Mental mastery
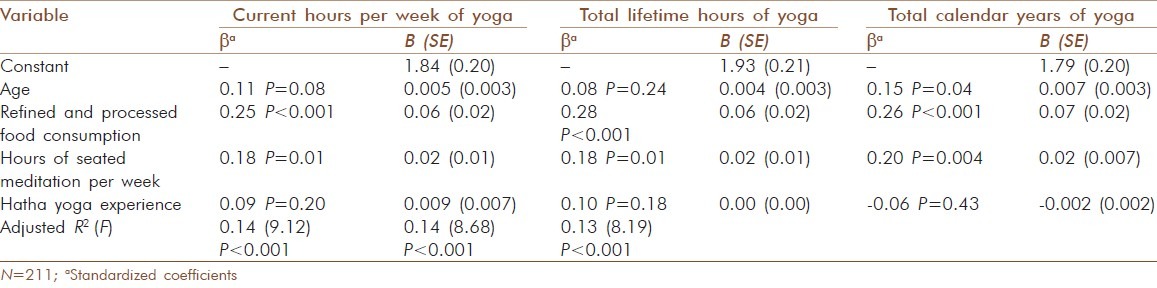
We evaluated the extent of yoga experience as a predictor of the level of mental mastery over and above significant covariates. Education, marital status, BMI, and hours of non-yogic exercise per week did not contribute significantly to mental mastery for any regression model. Therefore, we used a reduced model, including age, level of refined and processed food consumption, and hours of seated meditation per week as covariates. The contribution of Hatha yoga experience to the outcome was not significant for any regression model. However, the contribution of hours of seated meditation per week was significant for current hours per week, P = 0.01; for total lifetime hours, P = 0.01; and for total calendar years, P = 0.004 [Table 7]. The strongest predictor for all models was the level of refined and processed food consumption, P < 0.001, with lower levels of processed food consumption predicting higher levels of mental mastery.
Table 7.
Predictors of mental mastery
Subjective vitality
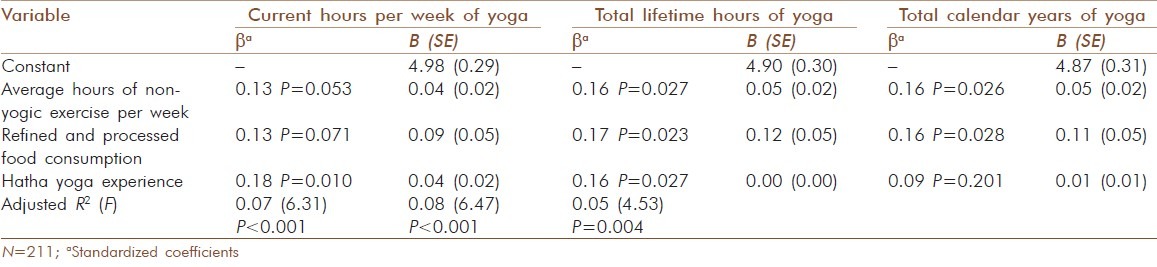
We evaluated the extent of yoga experience as a predictor of the level of subjective vitality over and above significant covariates. Age, education, marital status, BMI, and hours of seated meditation per week did not contribute significantly to subjective vitality for any regression model. We, therefore, used a reduced model, including only average hours of non-yogic exercise per week and level of refined and processed food consumption as covariates. The contribution to the outcome was significant for current hours per week, P = 0.01; and total lifetime hours, P = 0.03 [Table 8]. The contribution of total calendar years was not significant.
Table 8.
Predictors of subjective vitality
DISCUSSION
We used four outcome measures in this study to evaluate whether a longer-term and more frequent yoga practice was associated with higher levels of psychological wellness in a group of women aged 45 to 80 years. Three of these outcome measures – positive attitudes,[33] transcendence,[27] and subjective vitality[34] – were designed to measure long-term, stable, and enduring wellness. The Inadequate Mental Mastery subscale[27] was designed to measure sadness, irritability, anxiety, and other indicators of negative affect. Higher levels of negative affect were represented with lower scores on the Inadequate Mental Mastery subscale. Therefore, for this discussion, higher scores on the scale are assumed to indicate more positive moods.
Increasing levels of yoga practice were associated with higher levels of psychological wellness and subjective vitality in this study, regardless of age. Age contributed to mental mastery scores, but not to any other measure, when total calendar years of yoga practice were used as the main predictor. A higher age predicted improved moods. After correcting for covariates, total calendar years of yoga practice (without accounting for practice frequency) were not significantly related to any outcome variable. All significant findings were related to a measure of hours of practice, including hours per week and total lifetime hours. Although marital status has been found throughout the literature to predict increased SWB,[35] no relationship between marital status and SWB was found in this study. Body mass index was also unrelated to any outcome measures. Levels of processed food consumption contributed significantly to the outcomes for positive attitudes, mental mastery, and subjective vitality, with lower levels of processed food consumption predicting higher levels of wellness. Refined and processed food consumption was the most significant predictor in the mental mastery model, P < 0.001, for all measures of yoga experience.
All multiple regression analyses in this study required the use of WLS regression, because variances were unequal for each bivariate correlation evaluated. Scores of individuals with little yoga experience ranged in outcome from the lowest to the highest levels of wellness measured, including scores equal to the highest scores measured for yoga practitioners. However, as the Hatha yoga experience (measured both as current hours per week and as total lifetime hours) increased, minimum outcome scores steadily increased. The result was the right-triangular pattern typified in Figure 1. Findings were consistent with an interpretation that an increased yoga practice exercises an increasingly protective effect against low levels of wellness in women over 45 years. Practicing yoga for many years, but not often, generally did not offer these apparent protections.
Hours of seated meditation per week, a component of a yoga practice, contributed significantly to the outcome for positive attitudes, mental mastery, and transcendence of the ordinary. The contribution of Hatha yoga practice to mental mastery, the only measure of negative affect in the study, was not significant after correcting for hours of seated meditation per week. This finding departed from findings in the literature according to which levels of depression and anxiety declined significantly after brief Hatha yoga interventions. Although several of these studies[39–42] involved integrated interventions including asana, breathing exercises and seated meditation, other studies of depression and anxiety involved primarily Hatha yoga interventions. Cohen[21] examined Hatha yoga intervention and seated meditation separately, and found that in the first 8-week session, Hatha yoga had a stronger effect on improving mood than did the seated meditation. Three interventions[43–45] were based on Iyengar yoga, a method that focuses on carefully executed physical postures and typically does not involve separate breathing and meditation exercises. In all cases, participants showed significant improvements in depression and anxiety levels after Hatha yoga practice. Further research is needed to confirm or disconfirm the finding of this study that yoga asana (practiced with conscious breathing and awareness) did not predict improved moods after correcting for food patterns and seated meditation practice.
Findings of this study were generally consistent with prior research findings showing improved well-being after brief yoga interventions.[16–26] However, this study is the first to demonstrate a dose-response relationship between extent of yoga experience and measures of psychological wellness. For current hours of yoga practice per week, the strongest effect was shown for transcendence of the ordinary, a measure indicating feelings of unity with the surrounding world, intense happiness, joy, ecstasy, or bliss. For total lifetime hours of yoga practice, the strongest effect was shown for positive psychological attitudes. Although yoga experience (including both Hatha yoga and seated meditation) predicted all measures of wellness used, the weakest effect was shown for the single measure of negative affect used in this study. All outcome measures were strongly correlated, P < = 0.001, but distinct.
Assumptions and limitations
We assumed that participants had a working knowledge of English sufficient to understand and respond to questions. We assumed that responses to self-report questions were truthful and accurate. The study was limited by a non-probability sample selection, with uneven representation in terms of ethnicity and geographic location. Individuals more subjectively committed to a yoga practice may have been more inclined to participate in the study. Recruitment of some participants from yoga lists and through yoga networks may have also created bias in the sample selection. The study was limited by the lack of a control group. The lack of a question on income or socioeconomic status was also a limitation.
As all data were self-reported, the reliability of the information regarding lifestyle factors for this study is unknown. Fourteen records were unusable for the total lifetime hours calculation because the respondents entered total years without entering corresponding hours for each period of past practice. We noted these and other limitations to this study in a previous publication.[31]
The study was also limited by the cross-sectional, observational design. Cause and effect could not be determined. However, as noted in a previous publication,[31] a dose-response effect is sometimes considered evidence of a causal relationship even in the absence of a controlled experiment,[46,47] particularly when supported by prior research[48,49] and biological plausibility.[46] Of note, researchers have argued that for evaluating a self-selected, long-term, complex practice such as yoga, observational studies are preferable to experimental studies with fixed protocols and random assignment of participants, neither of which is generally applicable to a yoga practice in natural settings.[32,47,50–52]
On the basis of the results of this study, we were unable to rule out the possibility of ceiling effects in evaluating experienced yoga practitioners. The measures used in this study were designed for use with typical populations, but there is a need for more sensitive measures to detect unusually high levels of psychological and physical wellness in an older population. Most available measures of self-reported physical health show ceiling effects, in that 90% of respondents report their health as good or excellent.[9] Analogously, measures of spirituality showed ceiling effects when used with evangelical Christian populations.[53]
In terms of directions for future research, longitudinal studies are needed to track beginning yoga students over 2 to 5 decades. As income and socioeconomic status have been found to be a strong predictor of SWB,[35] we recommend including income as a covariate in future studies. We also suggest further investigations into other wellness practices, such as Tai Ch’i, seated meditation without asana, and whole-foods diets, to determine whether the statistical patterns found are similar to the heteroskedastic patterns found in this study. Although findings from many brief interventions have shown that Hatha yoga is of benefit to beginners for depression and anxiety, further research is needed to deconstruct the effects of Hatha yoga and seated meditation in evaluating effects on anxiety, depression, sadness, and irritability among long-term yoga practitioners.
CONCLUSION
In this non-probability sample of 211 women aged 45 to 80 years, we found a dose-response effect, with higher levels of yoga experience predicting increasingly high levels of psychological well-being on all outcomes measured. When yoga experience was measured as total calendar years, without considering the hours of yoga practice, we generally did not find a dose-response effect. A frequent yoga practice was the most consistent predictor of psychological wellness tested in this study. The regularity and frequency of the practice appears to be an essential component of the relationships discovered. Hours of seated meditation per week and avoidance of processed and refined food were also strong predictors.
Age was a predictor in only one of the 12 analyses conducted. In that instance, increased age predicted decreased levels of sadness, depression, anxiety and irritability. This finding was consistent with the preponderance of the literature showing overall increases in positive affect among older individuals. High levels of SWB were found among participants in this study regardless of the extent of yoga experience. However, Stanley and Isaacowitz[37] found that although older adults constituted a higher proportion of individuals with the most positive affect, they also constituted a higher proportion of individuals with the most negative affect. In contrast, low levels of SWB steadily disappeared from the scores on all measures used for this study as the extent of yoga experience increased. The results suggest that yoga, when practiced regularly and with commitment, may exercise a protective effect against low levels of SWB and subjective vitality among older adults.
Health is the strongest predictor of SWB among the elderly.[35] The frequent and long-term practice of Hatha yoga has been shown to predict increased physical wellness among older women.[31] These increases in physical wellness may be a component of the protective effects for SWB found in this study.
The results of this study were consistent with the teaching of yoga master B. K. S. Iyengar: “Daily practice of yoga will keep old age at bay. It enables us to endure what cannot be cured and makes the entire cycle of life worth living.”[54]
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Jonas WB, Beckner W, Coulter I. Proposal for an integrated evaluation model for the study of whole systems health care in cancer. Integr Cancer Ther. 2006;5:315–9. doi: 10.1177/1534735406295565. [DOI] [PubMed] [Google Scholar]
- 2.Antonovsky A. The salutogenic model as a theory to guide health promotion. Health Promot Int. 1996;11:11–8. [Google Scholar]
- 3.Duckworth AL, Steen TA, Seligman MEP. Positive psychology in clinical practice. Annu Rev Clin Psychol. 2005;1:629–51. doi: 10.1146/annurev.clinpsy.1.102803.144154. [DOI] [PubMed] [Google Scholar]
- 4.Frankl VE. Man's search for meaning. New York: Washington Square Press; 1995. [Google Scholar]
- 5.Rogers C. On becoming a person: A therapist's view of psychotherapy. New York: Houghton Mifflin; 1961/1995. [Google Scholar]
- 6.Maslow A. Toward a psychology of being. Princeton (NJ): D. Van Nostrand Company, Inc; 1962. [Google Scholar]
- 7.Peterson C. A primer in positive psychology. New York: Oxford University Press; 2006. [Google Scholar]
- 8.Jung CG. The undiscovered self. New York: New American Library; 1957/2006. [Google Scholar]
- 9.Becker CM, Moore JB, Whetstone L, Glascoff M, Chaney E, Felts M, et al. Validity evidence for the Salutogenic Wellness Promotion Scale (SWPS) Am J Health Behav. 2009;33:455–65. doi: 10.5993/ajhb.33.4.11. [DOI] [PubMed] [Google Scholar]
- 10.Ryff CD, Singer BH. Know thyself and become what you are: A eudaemonic approach to psychological well-being. J Happiness Stud. 2008;9:13–39. [Google Scholar]
- 11.Gable SL, Haidt J. What (and why) is positive psychology? Rev Gen Psychol. 2005;9:103–10. [Google Scholar]
- 12.Seligman M, Csikszentmihalyi M. Positive psychology: An introduction. Am Psychol. 2000;55:5–14. doi: 10.1037//0003-066x.55.1.5. [DOI] [PubMed] [Google Scholar]
- 13.Peterson C, Park N, Seligman ME. Orientations to happiness and life satisfaction: The full life versus the empty life. J Happiness Stud. 2005;6:25–41. [Google Scholar]
- 14.Bijlani RL, Vempati RP, Yadav RK, Ray RB, Gupta RB, Sharma R, et al. A brief but comprehensive lifestyle education program based on yoga reduces risk factors for cardiovascular disease and diabetes mellitus. J Altern Complement Med. 2005;11:267–74. doi: 10.1089/acm.2005.11.267. [DOI] [PubMed] [Google Scholar]
- 15.Iyengar BK. Light on Life: The Yoga Journey to Wholeness, Inner Peace, and Ultimate Freedom. US: Holtzbrinck Publishers; 2005. [Google Scholar]
- 16.Khalsa SB. Yoga as a therapeutic intervention: A bibliometric analysis of published research studies. Indian J Physiol Pharmacol. 2004;48:269–84. [PubMed] [Google Scholar]
- 17.Lipton L. Using yoga to treat disease: An evidence-based review. JAAPA. 2008;21:34–6. doi: 10.1097/01720610-200802000-00012. 38, 41. [DOI] [PubMed] [Google Scholar]
- 18.Kirkwood G, Rampes H, Tuffrey V, Richardson J, Pilkington K. Yoga for anxiety: A systematic review of the research evidence. Br J Sports Med. 2005;39:884–91. doi: 10.1136/bjsm.2005.018069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Pilkington K, Kirkwood G, Rampes H, Richardson J. Yoga for depression: The research evidence. J Affect Disord. 2005;89:13–24. doi: 10.1016/j.jad.2005.08.013. [DOI] [PubMed] [Google Scholar]
- 20.Chong CS, Tsunaka M, Tsang HW, Chan EP, Cheung WM. Effects of yoga on stress management in healthy adults: A systematic review. Altern Ther Health Med. 2011;17:32–8. [PubMed] [Google Scholar]
- 21.Cohen DR. A comparative study of Hatha yoga and seated meditation on mood elevation. Unpublished master's thesis. Philadelphia, PA: University of Pennsylvania; 2007. [Google Scholar]
- 22.Danhauer SC, Mihalko SL, Russell GB, Campbell CR, Felder L, Daley K, et al. Restorative yoga for women with breast cancer: Findings from a randomized pilot study. Psychooncology. 2009;18:360–8. doi: 10.1002/pon.1503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Khemka SS, Ramarao NH, Hankey A. Effect of integral yoga on psychological and health variables and their correlations. Int J Yoga. 2011;4:93–9. doi: 10.4103/0973-6131.85492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Khalsa SB. Presented at Symposium on Yoga Therapy and Research. Los Angeles, CA: International Association of Yoga Therapists; 2009. Research update: Mental health. [Google Scholar]
- 25.Eggleston B, Middlestadt SE, Lindeman A, McCormick B, Koceja D. Yoga's therapeutic value: Perceptions of yoga as serious leisure and the flow experience. International Journal of Yoga Therapy. 2009;(Supplement 43) [Google Scholar]
- 26.Sharma R, Gupta N, Bijlani RL. Effect of yoga based lifestyle intervention on subjective well-being. Indian J Physiol Pharmacol. 2008;52:123–31. [PubMed] [Google Scholar]
- 27.Sell H, Nagpal R. Regional Health Paper, SEARO, No 24. New Delhi: World Health Organization, Regional Office for South-East Asia; 1992. Assessment of subjective well-being: The Subjective Well-Being Inventory (SUBI) [Google Scholar]
- 28.Ryff CD, Singer BH, Love GD. Positive health: Connecting well-being with biology. Philos Trans R Soc Lond B Biol Sci. 2004;359:1383–94. doi: 10.1098/rstb.2004.1521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Bell IR, Koithan M. Models for the study of whole systems. Integr Cancer Ther. 2006;5:293–307. doi: 10.1177/1534735406295293. [DOI] [PubMed] [Google Scholar]
- 30.Quinn JF, Smith M, Ritenbaugh C, Swanson K, Watson MJ. Research guidelines for assessing the impact of the healing relationship in clinical nursing. Altern Ther Health Med. 2003;(Supplement 9):A65–79. [PubMed] [Google Scholar]
- 31.Moliver N, Mika EM, Chartrand MS, Burrus SW, Haussmann RE, Khalsa SB. Increased Hatha yoga experience predicts lower body mass index and reduced medication use in women over 45 years. Int J Yoga. 2011;4:77–86. doi: 10.4103/0973-6131.85490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.McGonigal K. Interview: A conversation with Timothy McCall, MD. International Journal of Yoga Therapy. 2009;19:143–7. [Google Scholar]
- 33.Kass JD, Friedman R, Lesserman J, Caudill M, Zuttermeister P, Benson H. An inventory of positive psychological attitudes with potential relevance to health outcomes: Validation and preliminary testing. Behav Med. 1991;17:121–9. doi: 10.1080/08964289.1991.9937555. [DOI] [PubMed] [Google Scholar]
- 34.Ryan RM, Frederick C. On energy, personality, and health: Subjective vitality as a dynamic reflection of well-being. J Pers. 1997;65:529–65. doi: 10.1111/j.1467-6494.1997.tb00326.x. [DOI] [PubMed] [Google Scholar]
- 35.George LK. Still happy after all these years: Research frontiers on subjective well-being in later life. J Gerontol B Psychol Sci Soc Sci. 2010;65B:331–9. doi: 10.1093/geronb/gbq006. [DOI] [PubMed] [Google Scholar]
- 36.Charles ST, Carstensen LL. Social and emotional aging. Annu Rev Psychol. 2010;61:383–409. doi: 10.1146/annurev.psych.093008.100448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Stanley JT, Isaacowitz DM. Age-related differences in profiles of mood-change trajectories. Dev Psychol. 2011;47:318–30. doi: 10.1037/a0021023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Peterson C, Seligman MS. Character strengths and virtues: A handbook and classification. New York: Oxford University Press; 2004. [Google Scholar]
- 39.Bennett SM, Weintraub A, Khalsa SB. Initial evaluation of the LifeForce Yoga program as a therapeutic intervention for depression. International Journal of Yoga Therapy. 2008;18:49–58. [Google Scholar]
- 40.Butler LD, Waelde LC, Hastings TA, Chen XH, Symons B, Marshall J, et al. Meditation with yoga, group therapy with hypnosis, and psychoeducation for long-term depressed mood: A randomized pilot trial. J Clin Psychol. 2008;64:806–20. doi: 10.1002/jclp.20496. [DOI] [PubMed] [Google Scholar]
- 41.Kjellgren A, Bood SA, Axelsson IK, Norlander T, Saatcioglu F. Wellness through a comprehensive Yogic breathing program – A controlled pilot trial. BMC Complement Altern Med. 2007;7:43–50. doi: 10.1186/1472-6882-7-43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Krishnamurthy MN, Telles S. Assessing depression following two ancient Indian interventions: Effects of yoga and Ayurveda on older adults in a residential home. J Gerontol Nurs. 2007;33:17–23. doi: 10.3928/00989134-20070201-05. [DOI] [PubMed] [Google Scholar]
- 43.Michalsen A, Grossman P, Acil A, Langhorst J, Ludtke R, Esch T, et al. Rapid stress reduction and anxiolysis among distressed women as a consequence of a three-month intensive yoga program. Med Sci Monit. 2005;11:CR555–61. [PubMed] [Google Scholar]
- 44.Shapiro D, Cook IA, Davydov DM, Ottaviani C, Leuchter AF, Abrams M. Yoga as a complementary treatment of depression: Effect of traits and moods on treatment outcome. Evid Based Complement Alternat Med. 2007;4:493–502. doi: 10.1093/ecam/nel114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Woolery A, Myers H, Sternlieb B, Zeltzer L. A yoga intervention for young adults with elevated symptoms of depression. Altern Ther Health Med. 2004;10:60–3. [PubMed] [Google Scholar]
- 46.Heaney RP. Long-latency deficiency disease: Insights from calcium and vitamin D. Am J Clin Nutr. 2003;78:912–9. doi: 10.1093/ajcn/78.5.912. [DOI] [PubMed] [Google Scholar]
- 47.Seligman M. The effectiveness of psychotherapy: The consumer reports study. Am Psychol. 1995;50:965–74. doi: 10.1037//0003-066x.50.12.965. [DOI] [PubMed] [Google Scholar]
- 48.Kristal AR, Littman AJ, Benitez D, White E. Yoga practice is associated with attenuated weight gain in healthy, middle-aged men and women. Altern Ther Health Med. 2005;11:28–33. [PubMed] [Google Scholar]
- 49.Lazar SW, Kerr CE, Wasserman RH, Gray JR, Greve DN, Treadway MT, et al. Meditation experience is associated with increased cortical thickness. Neuroreport. 2005;16:1893–7. doi: 10.1097/01.wnr.0000186598.66243.19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Concato J. Observational versus experimental studies: What's the evidence for a hierarchy? NeuroRx. 2004;1:341–7. doi: 10.1602/neurorx.1.3.341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Ligthelm RJ, Borzi V, Gumprecht J, Kawamori R, Wenying Y, Valensi P. Importance of observational studies in clinical practice. Clin Ther. 2007;29:1284–92. [PubMed] [Google Scholar]
- 52.Forbes B. Yoga and managed care: A cautionary tale. International Journal of Yoga Therapy. 2010;20:22–5. [Google Scholar]
- 53.Bufford RK, Paloutzian RF, Ellison CW. Norms for the Spiritual Well-Being Scale. J Psychol Theol. 1991;19:56–70. [Google Scholar]
- 54.Iyengar BKS. Forward. In: Francina S, editor. The new yoga for people over : A comprehensive guide for midlife and older beginners. Deerfield Beach (FL): Health Communications; 1997. pp. xiii–iv. [Google Scholar]