

Summary
A cross-sectional study was conducted to investigate the different characteristics of attempted suicide by self-inflicted burn cases compared with other accidental burn cases admitted to the Burns Unit in Al-Jumhoori Teaching Hospital in Mosul over a one-year period from March 1, 2011 to March 1, 2012. Of 459 burn cases, 103 (22.44%) had self-inflicted burns. The mean total body surface area of suicide attempters was 61%, markedly higher than in other cases (20%) (P= 0.0001). Among all self-inflicted burn cases, burns were caused by flame, while scald was the commonest cause (56.5%) in accidental burns. There was a significant difference in the sex ratio between self-inflicted burn cases (1:11.9) and accidental burn cases (1:1) (P = 0.0001). Case fatality rates for self-inflicted burn and accidental burn cases were 80.6% and 14.9%, respectively. The overall mean ages for self-inflicted burn and accidental burn cases were 24.3 and 15.6 years, respectively. Compared to all other burn cases, self-inflicted burn cases had a significantly larger mean percentage of surface body area burned (61.0±28.2 versus 20.7±15.8; P = 0.0001). In conclusion, self-inflicted burns remain a common cause of admission to our burn unit. The extent of burns is often large, since most suicide attempters use an accelerant that accounts for the high mortality in this group.
Keywords: self-inflicted, burn, suicide
Abstract
Les Auteurs ont effectué une étude comparative des modalités différentes entre les cas de tentatives de suicide manqué et les cas de brûlure pour d’autres causes traités à l’Unité de Brûlures auprès du Centre Universitaire Al-Jumhoori à Mosul, Irak, pendant la période d’un an (mars 2011/mars 2012). Sur 459 cas de brûlure, 103 patients (22,44%) présentaient des lésions autoinfligées. La surface cutanée moyenne brûlée dans le cas de suicide manqué était de 61%, un niveau plus élevé que les autres cas (20%) (P= 0.0001). Parmi tous les cas de brûlures autoinfligées, les lésions ont été causées par les flammes, tandis que l’ébouillantement a été la cause la plus commune des brûlures accidentelles (56.5%). La différence pour ce qui regarde le sexe dans les brûlures autoinfligées et accidentelles était significative (1:11.9) (1:1) (P = 0,0001). Les taux de mortalité pour les brûlures autoinfligées et accidentelles étaient 80,6% et 14,9%, respectivement. L’âge moyen de tous les cas était 24,3 ans (autoinfligés) et 15,6 ans (accidentelles), respectivement. Par rapport aux autres cas de brûlures les cas de brûlures autoinfligés avaient un pourcentage de surface corporelle brûlée significativement plus élevée (61,0±28,2 versus 20,7±15.8; P = 0,0001). Pour conclure, les brûlures autoinfligées restent une cause commune de l’hospitalisation dans autres unités de brûlures. L’extension de la brûlure est souvent très étendue puisque les personnes qui tentent le suicide utilisent fréquemment des substances qui favorisent les flammes, ce qui explique le taux élevé de mortalité dans ce type de brûlure.
Introduction
Self-inflicted burn (SIB) injuries account for a considerable number of burns admissions worldwide. While in western countries these injuries are relatively uncommon, in some parts of the world they are still a major cause of extensive burns, and consequently of burn deaths. This suicide method is most frequently reported in developing nations, being rather rare in developed countries.1 In fact, in developing countries like Iran, India, and Sri Lanka, it accounts for as many as 27% of all suicide attempts. 2-4
Patients with SIBs are important, as their burns are potentially avoidable, and they can be difficult to manage. In Iraq and other Middle East countries, suicide is an underestimated problem. Official statistics are likely to be lower than true rates because of religious and social reasons.
This study aims to assess the characteristics of patients who have attempted suicide by self-inflicting burns compared with other accidental burn patients admitted to the Burns Unit in Al-Jumhoori Teaching Hospital. The goal is to help improve the prognosis and development of a preventive program designed for the target population.
Material and methods
Before starting the data collection, an official permission was obtained from Nineveh Directorate of Health (scientific and ethical committees) to conduct the present study. In order to achieve the purpose of the study, a cross-sectional study design was adopted. All burn patients (SIBs and accidental) admitted to the Burns Unit in Al-Jumhoori Teaching Hospital, Nineveh Directorate of Health over one year, from March 1, 2011 to March 1, 2012, or their relatives, were interviewed. Self-inflicted burn cases were defined as those who had attempted suicide; they were identified from the history given by the patient or by a reliable eyewitness with explicit evidence of deliberate selfharm;5 the others were considered as accidental burns.
Data from both self-inflicted and accidental burn cases were collected by a specially designed questionnaire which included: age, sex, occupation, education, body surface area (BSA) involved, anatomical location of the burn, etiology, hospital stay, and treatment outcome.
Statistical analysis was performed using Minitab version 14.1. Differences between various groups were assessed by using the Chi-square and independent t-test for 2 means. A mean value (P) lower than 0.05 was considered significant. Odds ratio (OR) was used to identify the presence of significant association between characteristics of interest and SIB. It is defined as the odds ratio that the cases (SIB cases) were exposed to (characteristics of interest) on the odds that the controls (accidental burns cases) were exposed to. It is regarded as an excellent measure of whether the presence of a certain exposure (characteristic) is associated with specific injury (SIB).6
Results
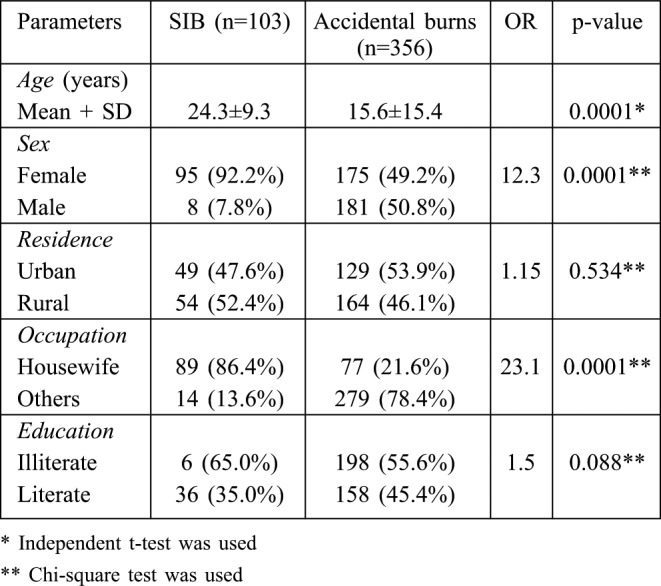
Of the 459 emergency burn admissions over the oneyear period, 103 (22.2%) cases presented with SIB and 356 (77.6%) with accidental burns. The socio-demographic characteristics of the study population are shown in Table I. The mean age of the SIB cases was 24.3±9.3 years; with a range of 11 to 75 years, while the mean age of cases with accidental burn was 15.6±15.4 years; and the range was 1 to 70 years. A highly significant difference was found between two means (P=0.0001). Male to female ratio among SIB cases was 1:12, significantly higher than that of accidental burn cases (1:1) (P = 0.0001). Male sex appeared to be significantly protective against SIB in an extremely significant way (P=0.0001). In other words, females were considerably more likely to attempt suicide than males (OR=12.3, P=0.0001).
Table I. Socio-demographic profile of study groups.
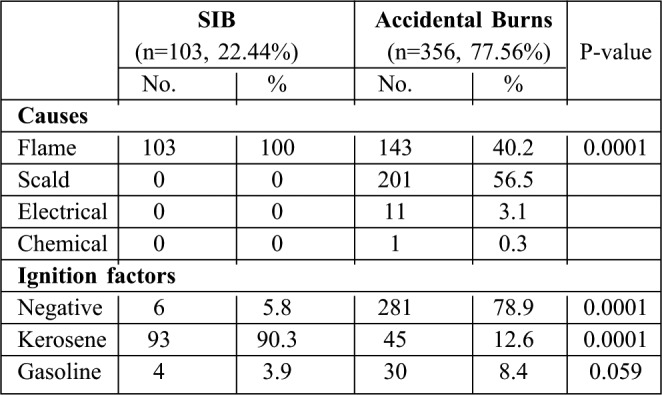
Amongst all SIB patients, the place of attempted suicide was home. As to accidental burns, 82.9% occurred at home, 10.1% at the workplace, 0.6% in the farm, and 6.4% in the street. Kerosene was the accelerant material used by 90.3% of the SIB cases, compared to 12.6% in accidental burn cases, a highly significant difference (P=0.0001). Most cases attempted suicide by pouring an inflammable fluid over themselves and then igniting it, or by directly setting on fire their own clothes or surroundings. All cases had deep partial or full thickness burns. In all SIB cases, burns were significantly caused by flame, compared to 40.2% among accidental burn cases (P=0.0001); while scald was the commonest cause (56.5%) within accidental burns, followed by flame (40.2%), electricity (3.1%), and chemicals (0.3%) (Table II).
Table II. Causes of burns and ignition factor of the study sample.
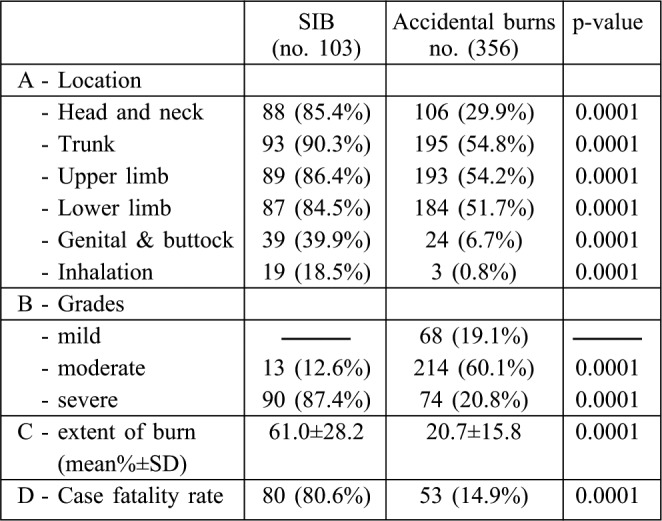
The proportion of total body surface area (BSA%) involved was significantly larger (P=0.0001) in the SIB population (mean 61.0% ± 28.2) compared to the accidental burn population (mean 20.7 ± 15.8). Severe burns (>30% TBSA) were more frequently observed in SIB cases (87.4%). Head and neck were significantly more affected in SIB cases than in accidental burn cases (85.4% and 29.9% respectively) (P=0.0001). Self-inflicted burn cases experienced a significantly higher fatality rate than accidental burn cases (80.6% versus 14.9%) (P=0.0001). Moreover, they showed a significantly higher prevalence of inhalation injuries (P=0.0001) (Table III).
Table III. Clinical findings and case fatality among study groups.
Although urban residency was less frequent among SIB cases (47.6%), no meaningful association was found with this factor. Unfortunately, housewives appeared to be 23 times more prone to try SIB than other categories of workers (OR=23.03, P=0.0001). Education of SIB cases played no noteworthy role.
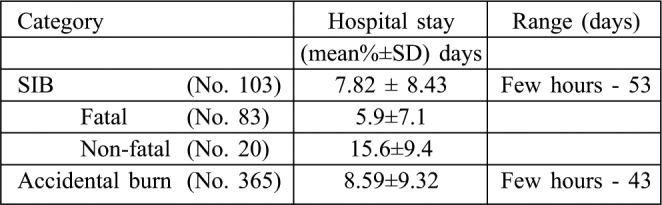
Accidental burn cases have a mean duration of hospital stay of 8.59± 9.32 days, ranging from a few hours to 43 days, while the mean hospital stay for SIB cases was 7.82±8.43 day, ranging from a few hours to 53 days. Nonfatal SIB cases have a significantly longer mean duration of stay (P=0.0001) than fatal cases (15.6 ± 9.9 days compared to 5.9 ± 7.1 days) (Table IV).
Table IV. Mean duration of hospital stay ± SD of study groups.
Discussion
The sample analyzed in this study is regarded as a representative epidemiological sample of burn cases in Mosul City. This city is located in the North of Iraq; it has only one burns unit attached to Al-Jumhoori Teaching Hospital. This unit virtually treats all severe burn cases occurring in Mosul. Furthermore, it is designated by the Nineveh Health Directorate as a referral center for the entire Nineveh Province. On this basis, the present study population can be considered as a good model for epidemiological research.
The relatively large number of SIB cases (103), and of accidental burn cases in particular (356), was an asset for statistical analysis. On the other hand, the main limitation of the present study, as in all earlier reports, was the limited information on the psychiatric morbidity underlying the suicidal attempt.
Self-burning is relatively uncommon in western countries, while in some parts of the world it is a major cause of exclusive burns and subsequently of burn death.7 In the present study, 22.44% of burned cases were SIB. The highest rates of SIB as a cause of burn admission were reported from Mumbai India (40%), Batticaloa Sri Lanka (25%), Egypt (17%), Iran (14.5%), and Kurdistan Iran (9.0%).7
Initially, most cases insisted on claiming that it was an accident, and individuals went to great lengths to explain how the kerosene lamp had fallen over them, or how their clothes had caught fire. With time, denial recedes, and the true story emerges. Usually, at the time of admission, patients were excited, restless, confused, and gave unreliable information. This fact suggests that the real number of suicide attempts is higher than those reported in the present study. Meanwhile, because of social and religious reasons, some victims and their families denied that the event was SIB. Social stressors, such as financial problems, marital dispute and relationship conflicts, traditional male dominance, and illiteracy have been implicated by many studies.8-12 Although stressors are not documented in the present study, religion, culture, and tradition are likely to play a major role.
In the present study, the mean age of SIB patients was close to other reports from Iran, Sri Lanka, India, Jordan, and Egypt,7,12 but it was much lower than reports from Ireland. 13 This might be explained, at least in part, by the fact that the Iraqi population is young, with people younger than 20 representing over 50% of the general population. Victims in Asia were roughly about 10 years younger than in Europe, and the vast majority were females. This may be related to the major changes happening at this age, the transition from youth to adulthood and adolescent marriages, with all the responsibilities that are placed particularly on young girls who are very often ill-prepared to play the housewife role. Soni Raleigh and Balarajan14 favoured this explanation. It is noteworthy that in the present study the highest proportion of SIB cases were females (92.2%), and similar findings were also reported by others. 5,7
Furthermore, a highly significant association was found with female sex (P=0.0001). Similar findings were reported by Andreassen and Noyes,15 Ben Meir et al.,16 and Sheth et al.17 On the other hand, Davidson and Brown,18 and Sanchez et al.19 showed no sex difference in their study. Conversely, Cameron et al.20 reported male preponderance. Variations in findings among different studies may be due to differences in demographic, cultural, and social characteristics of studied populations. In this study, most victims were young housewives who had attempted suicide at home. Most likely, housewives are at a greater risk of self-burning since they typically stay home, a factor that probably limits their access to other suicide methods.21
In this study, the average BSA burned was significantly larger in the SIB population than in the accidental injury population (61% vs. 20.7%) (P=0.0001). This is not surprising, because SIB intentionally self-inflict a major burn injury, whereas victims of accidental burns try to minimize the extent of the burn. This high BSA burned in SIB cases is similar to other reports from Iran, Israel, Turkey, Greece, Florida, and Zimbabwe, yet it is higher than in most European, American, and Indian subcontinent populations. 5,7
The use and nature of fire accelerants varies according to availability in various parts of the world. In this work, kerosene and gasoline were the most frequently used substances by victims. When reported, burn sizes were usually extensive. Furthermore, the present study data showed that the self-inflicted method was almost always a flame burn injury, while scalds predominate over other causes of accidental burns, and flame was the second commonest cause. This finding is in agreement with a number of studies reporting that scalds are the most important cause of minor burns throughout the world.22-24 It seems that most young women doused themselves with kerosene after a home dispute, or a divergence with their spouse, parent in law or other intimate relatives.
In this study, most patients (90.3%) used kerosene as a fire accelerant. This is close to the reports from Iran, India, Sri Lanka, Jordan, Korea, and Zimbabwe, while in European and North American populations, gasoline was used most frequently.5,7 In the Middle East, kerosene is available in every household since it is used for cooking and heating purposes. As one would expect, subjects who set their clothes on fire using an accelerant have more extensive and deeper burns than those who use other methods.
Mortality rates among SIB cases vary from 14% in the USA25 to 90% in India.26 In this study, the SIB population had more serious burns, and also a markedly higher death rate compared to accidental burn cases. Therefore, the case fatality rate in SIB cases was significantly higher (80.6%) than in accidental burn cases (14.95%) (P=0.0001). This could be attributed to the greater use of flammable liquids as kerosene and gasoline (94.2% versus 21%, respectively), and to the higher proportion of BSA burned with a mean of 61% compared to 20.7% in accidental burn cases. More or less similar findings were reported by other workers such as Davidson and Brown18 (48%), Ben Meir et al.16 (77%), and Mabrouk et al. in Egypt (73%).12
Conclusion
Suicide attempts by means of SIB are a serious social problem. Its solution calls for the joint efforts of physicians, psychiatrists, and sociologists. Further in-depth research to determine the psychiatric and social backgrounds of such cases is necessary. Efforts to inform the public about the dangers of gasoline stoves as a cause of accidental and suicidal burns are recommended through the media.
Acknowledgments
The author would like to thank Dr. Humam Al-Zubeer, Ph.D., Lecturer, Department of Community Medicine, College of Medicine, University of Mosul for his valuable help and assistance in the statistical analysis of data. Thanks and appreciation are due to Dr. Rasha A. Fathel, Senior House Officer, Burns Unit, Al- Jumhoori Teaching Hospital, for her help in data collection and daily support to burns victims.
References
- 1.Ahmadi A, Mohammadi R, Schwebel DC, et al. Psychiatric disorders (Axis I and Axis II) and self-immolation: a case–control study from Iran. J Forensic Sci. 2010;55:447–50. doi: 10.1111/j.1556-4029.2009.01268.x. [DOI] [PubMed] [Google Scholar]
- 2.Ahmadi A, Mohammadi R, Schwebel DC, et al. Classic philosophy lessons and preventing self-inflicted burns: a call for action. Burns. 2009;35:154–5. doi: 10.1016/j.burns.2008.05.022. [DOI] [PubMed] [Google Scholar]
- 3.Ahmadi A, Mohammadi R, Schwebel DC, et al. Familial risk factors for self-immolation: a case–control study. J Womens Health (Larchmt) 2009;18:1025–31. doi: 10.1089/jwh.2008.1192. [DOI] [PubMed] [Google Scholar]
- 4.Ahmadi A, Ytterstad B. Prevention of self-immolation by community-based intervention. Burns. 2007;33:1032–40. doi: 10.1016/j.burns.2006.11.015. [DOI] [PubMed] [Google Scholar]
- 5.Maghsoudi H, Garadagi A, Jafary G, et al. Women victims of selfinflicted burns in Tabriz, Iran. Burns. 2004;30:217–20. doi: 10.1016/j.burns.2003.10.010. [DOI] [PubMed] [Google Scholar]
- 6.Gordis L. Epidemiology. (3rd ed.) Philadelphia: Elsevier Saunders; 192 [Google Scholar]
- 7.Laloe V. Patterns of deliberate self-burning in various parts of the world. A review. Burns. 2004;30:207–15. doi: 10.1016/j.burns.2003.10.018. [DOI] [PubMed] [Google Scholar]
- 8.Rashid A, Gowar JP. A review of the trends of self-inflicted burns. Burns. 2004;30:573–6. doi: 10.1016/j.burns.2004.03.010. [DOI] [PubMed] [Google Scholar]
- 9.Wallace KL, Pegg SP. Self-inflicted burn injuries: an 11-year retrospective study. J Burn Care Rehabil. 1999;20:191–4. [PubMed] [Google Scholar]
- 10.Askari S. Special report on women. Farhang-e-Tose’e J. 1998:37–42. [Google Scholar]
- 11.Maghsoudi H. Women victims of self-inflicted burns in Tabriz, Iran. Burns. 2004;30:217–20. doi: 10.1016/j.burns.2003.10.010. Statistics were published by the Ministry of Interior of Iran for years 1989-1990. [DOI] [PubMed] [Google Scholar]
- 12.Mabrouk A, Omar A, Massoud K, et al. Suicide by burns: a tragic end. Burns. 1999;25:337–9. doi: 10.1016/s0305-4179(98)00179-x. [DOI] [PubMed] [Google Scholar]
- 13.O’Donoghue J, Panchal J, O’Sullivan S, et al. A study of suicide and attempted suicide by self-immolation in an Irish psychiatric population: an increasing problem. Burns. 1998;24:144–6. doi: 10.1016/s0305-4179(97)00096-x. [DOI] [PubMed] [Google Scholar]
- 14.Soni Raleigh V, Balarajan R. Suicide and self-burning among Indians and West Indians in England and Wales. Br J Psychiatry. 1992;161:365–8. doi: 10.1192/bjp.161.3.365. [DOI] [PubMed] [Google Scholar]
- 15.Andreassen N, Noyes R. Suicide attempts by self-immolation. Am. J. Psychiatry. 1975;132:554–5. doi: 10.1176/ajp.132.5.554. [DOI] [PubMed] [Google Scholar]
- 16.Ben Meir P, Sagi A, Ben Yakar Y, et al. Suicide attempts by selfimmolation: our experience. Burns. 1990;16:257–8. doi: 10.1016/0305-4179(90)90135-j. [DOI] [PubMed] [Google Scholar]
- 17.Sheth H, Dziewulski P, Settle J. Self-inflicted burns: a common way of suicide in the Asian population. A 10 year retrospective study. Burns. 1994;20:334–5. doi: 10.1016/0305-4179(94)90062-0. [DOI] [PubMed] [Google Scholar]
- 18.Davidson T, Brown L. Self-inflicted burns: a five year retrospective study. Burns. 1985;11:157–8. doi: 10.1016/0305-4179(85)90061-0. [DOI] [PubMed] [Google Scholar]
- 19.Sanchez G, Palao R, Legarre F. Self-inflicted burns. Burns. 1994;20:535–6. doi: 10.1016/0305-4179(94)90016-7. [DOI] [PubMed] [Google Scholar]
- 20.Cameron D, Pegg S, Muller M. Self-inflicted burns. Burns. 1997;23:519–21. doi: 10.1016/s0305-4179(97)00039-9. [DOI] [PubMed] [Google Scholar]
- 21.Laloe V, Ganesan M. Self-immolation a common suicidal behavior in eastern Sri Lanka. Burns. 2002;28:475–480. doi: 10.1016/s0305-4179(02)00047-5. [DOI] [PubMed] [Google Scholar]
- 22.Saadat M. Epidemiology and mortality of hospitalized burn patients in Kohkiluye va Boyerahmad province (Iran): 2002–2004. Burns. 2005;31:306–9. doi: 10.1016/j.burns.2004.10.012. [DOI] [PubMed] [Google Scholar]
- 23.Ansari-Lari M, Askarian M. Epidemiology of burns presenting to an emergency department in Shiraz, south Iran. Burns. 2003;29:579–81. doi: 10.1016/s0305-4179(03)00066-4. [DOI] [PubMed] [Google Scholar]
- 24.Barret J, Gomes P, Solano I, et al. Epidemiology and mortality of adult burns in Catalonia. Burns. 1999;25:325–9. doi: 10.1016/s0305-4179(98)00190-9. [DOI] [PubMed] [Google Scholar]
- 25.Antonowicz J, Taylor L, Showalter P, et al. Profiles and treatment of attempted suicide by self-immolation. Gen Hosp Psychiatry. 1997;19:51–5. doi: 10.1016/s0163-8343(96)00136-3. [DOI] [PubMed] [Google Scholar]
- 26.Subrahmanyam M. Epidemiology of burns in a district hospital in western India. Burns. 1996;22:439–42. doi: 10.1016/0305-4179(96)00001-0. [DOI] [PubMed] [Google Scholar]